

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Urothelial carcinoma, also known as transitional cell carcinoma, originates in the urothelium that lines the urethra, bladder, ureters, and renal pelvis. Although upper tract urothelial carcinoma (UTUC) accounts for approximately 5% to 10% of urothelial tumors, it is becoming increasingly prevalent [12]. Radical nephroureterectomy (RNU) with bladder cuff removal represents the standard surgical treatment for UTUC, while segmental ureterectomy has been recently considered in imperative (e.g., renal insufficiency and solitary functional kidney) or elective cases [3].
Due to the aggressive nature of this cancer, the prognosis of UTUC is generally poor, and its oncologic outcomes are unsatisfactory. Therefore, many researchers have attempted to identify its prognostic factors [4]. Postoperatively pathologic T stage, lymph node involvement (LNI), and lymphovascular invasion (LVI) are known as the prognostic factors for UTUC. Similarly, preoperative factors, including increased age, presence of hydronephrosis, tumor location and neutrophil-to-lymphocyte ratio have reportedly been associated with poor prognosis [2456].
Intravesical recurrence (IVR) is known to occur in 30%–50% of patients within the first year after RNU for UTUC [7]. Recently, a series of studies including meta-analyses have reported that prophylactic intravesical chemotherapy decreased bladder tumor recurrence after surgical treatment [278]. Therefore, in order to predict IVR after RNU, many studies have been conducted to identify factors such as positive urine cytology, multifocality and the use of diagnostic ureteroscopy [8910].
Pyuria, easily identified using low-cost non-invasive urine tests, reflects the inflammatory state of the urinary tract. Numerous studies have reported that pyuria is a significant prognostic factor in urothelial carcinomas [1112131415]. However, to date, only a few studies have evaluated whether sterile pyuria can be a predictive factor for IVR [1213]. Thus, the purpose of this study was to evaluate if preoperative sterile pyuria can be a prognostic factor for IVR and overall survival (OS) in patients with UTUC undergoing surgery.
Go to : 
MATERIALS AND METHODS
After institutional review board approval, we retrospectively reviewed the medical records of patients who were diagnosed with UTUC and treated at Korea University Medical Center from October 2003 to December 2016. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in a prior approval by the Institutional Review Board of Korea University Medical Center (approval number: 2018AS0011). Due to retrospective enrollment, written informed consent from patients was waived. After excluding patients who had insufficient clinical data, metastatic disease, undergone previous or concomitant radical cystectomy, received preoperative antibiotics due to urinary tract infections, and positive identification of bacteria in urine culture, a total of 176 patients who underwent laparoscopic/open RNU or open segmental ureterectomy were finally included in this study. Sterile pyuria was defined as urine containing five or more white blood cells (WBCs) per high-power field (HPF) in the absence of bacteria in urine culture. The urine analysis and urine culture were performed on all patients before any manipulation such as cystoscopy, ureteroscopy, or surgery. A standard RNU with bladder cuff removal was performed on most patients, while segmental ureterectomy was conducted on selected patients, considering the following: age, comorbidities such as chronic renal failure, location, number, size, and grade of the tumor, as well as previous or concomitant bladder cancer. Extended lymphadenectomy was not performed routinely if clinically apparent lymphadenopathy was not present on intraoperative or preoperative imaging. In addition, transurethral resection was performed before RNU or segmentectomy if patients were diagnosed with synchronous non-muscle invasive bladder cancer (NMIBC). Among 176 patients with UTUC, a total of 42 patients with non-metastatic, locally advanced upper tract urothelial cell carcinoma (pT3, pT4, or pT1-2N1-3) after undergoing RNU received adjuvant chemotherapy. To meet the criteria for adjuvant chemotherapy, treatment must have started within 3 months of undergoing RNU. Cisplatin-based chemotherapy was the most common regimen; 26 patients received gemcitabine/cisplatin regimen, and 10 received methotrexate/vinblastine/doxorubicin/cisplatin regimen. Six patients with impaired renal function received a gemcitabine/carboplatin regimen.
All clinicopathological data including age; sex; body mass index; microscopic WBC count in the urine; preoperative cytology; presence of smoking, hypertension, diabetes mellitus (DM), and preoperative hydronephrosis; tumor side, size, and site (renal pelvis, ureter, or both); surgical method (RNU or segmentectomy); type of surgery (open or laparoscopy); previous or synchronous NMIBC; pathologic T stage; tumor grade (according to the TNM classification and World Health Organization grade); concomitant carcinoma in situ; lymph node status; LVI; positive surgical margin; and IVR were collected from the hospital records. Postoperative follow-up including cystoscopy, blood or urinary cytology, abdominal or chest computed tomography and bone scans were performed in accordance with the routine surveillance protocol. Patients were subjected to a general follow-up every 3 months for 2 years after surgery and every 6 months from the third year.
Chi-square tests and Student t-tests were used for comparisons of clinicopathological features between the pyuria group and non-pyuria group. After confirming the significant factors in the previous analysis, univariate and multivariable Cox proportional hazard models were used. The intravesical recurrence-free survival (IVRFS) and OS curves were calculated using the Kaplan–Meier method. The IVRFS was defined as the time from the date of the RNU or segmentectomy to the date of the transurethral resection of bladder tumor (TURBT) for IVR. For all analyses, differences were considered significant at a p-value of <0.05. Statistical analyses were performed using the IBM SPSS Statistics ver. 21.0 software (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
The mean age of patients was 66.1 years old and the mean follow-up period was 36.9 months. Patients were divided into two groups according to the presence, or absence of sterile pyuria, with the former condition occurring in 91 of 176 patients. Table 1 details the characteristics of UTUC patients presenting with, and without pyuria. There were no significant differences in the baseline characteristics between the pyuria group and the non-pyuria group regarding age, sex, follow-up period, body mass index, smoking, comorbidities, tumor grade, T stage, multiplicity, or recurrence history. Bladder cancer recurred in 49 (53.8%) patients with pyuria and in 16 (18.8%) patients without pyuria, showing a significant statistical difference (p<0.05).
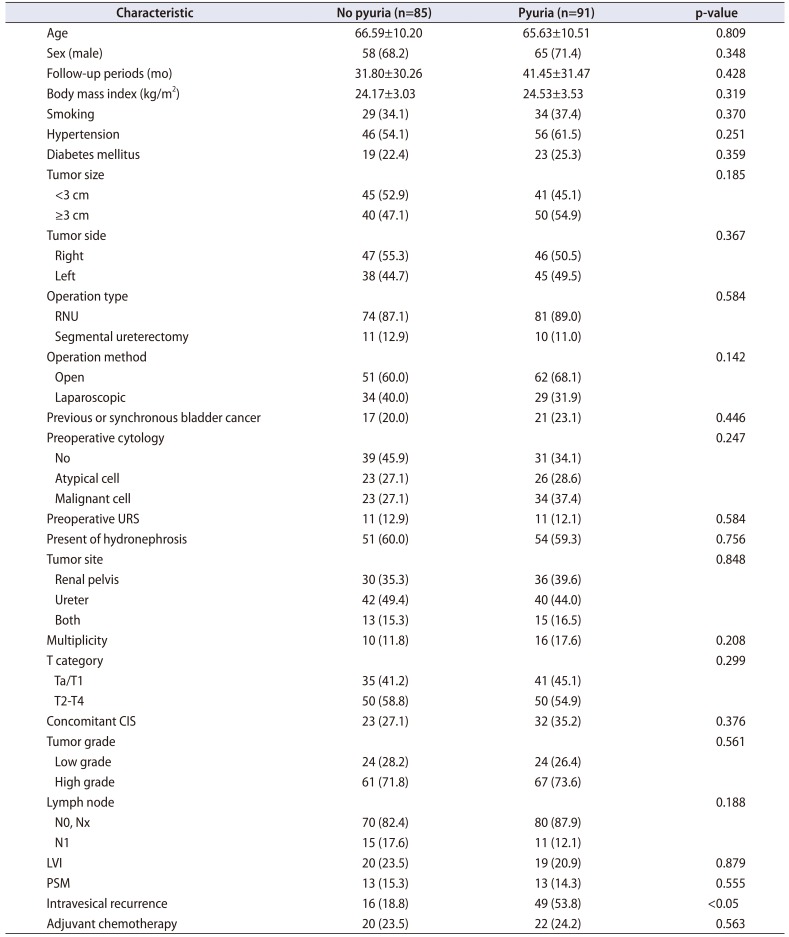
Table 1
Characteristics of UTUC patients presenting with pyuria and without pyuria
![]()
Results of the univariate and multivariable Cox proportional hazards analyses that predict IVR and the OS in all patients with UTUC are detailed in Tables 2 and 3, respectively. In the multivariable model, sterile pyuria (hazard ratio [HR], 3.504; p=0.001) was an independent prognostic factor for IVR. Moreover, the other factors significantly associated with IVR were DM (HR, 2.056; p=0.022), high-grade tumor (HR, 1.865; p=0.037), and LVI (HR, 2.620; p=0.019) (Table 2). In the univariate analysis, OS was associated with the tumor stage (p=0.007), tumor grade (p=0.037), LNI (p=0.009), and LVI (p=0.001). However, in the multivariable analysis, OS was not significantly related to other factors, except for LVI (HR, 3.713; p=0.018) (Table 3).
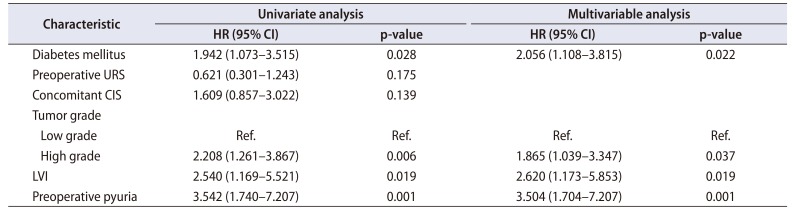
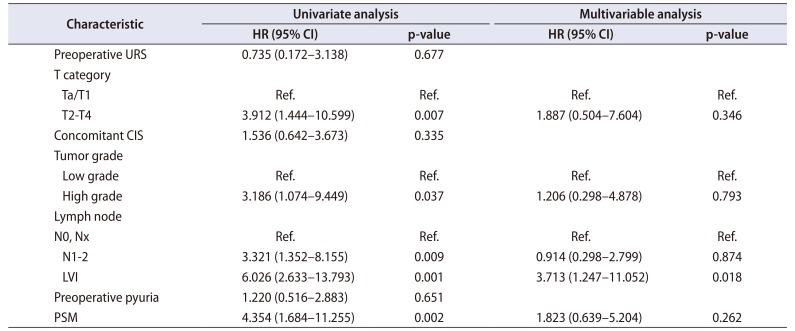
Table 2
Univariate and multivariable analysis of intravesical recurrence
![]()
Table 3
Univariate and multivariable analysis of overall survival
![]()
The Kaplan–Meier analysis showed that IVRFS (12 months) was significantly shorter for sterile pyuria (58.8% vs. 30.5%, respectively; p=0.001), LVI (48.6% vs. 28.6% respectively; p=0.032), DM (45.6% vs. 37.5%, respectively; p=0.019), and high-grade tumor (62.2% vs. 27.3%, respectively; p=0.003) (Fig. 1). Additionally, in the 2-year OS, the tumor stage (94.9% vs. 87.5%, respectively; p=0.004), tumor grade (94.9% vs. 89.0%, respectively; p=0.027), LNI (94.6% vs. 62.2%, respectively; p=0.005), LVI (95.4% vs. 73.6%, respectively; p=0.001), and positive surgical margin (93.9 vs. 67.7%, respectively; p=0.001) showed a significantly worse outcome. Conversely, the pyuria group had a lower OS than the non-pyuria group, without a significant difference (92.8% vs. 87.6%, respectively; p=0.650).
 | Fig. 1Kaplan–Meier plots showing the probability of intravesical recurrence-free survival in 176 patients with upper tract urothelial carcinoma, stratifiedby the following predictors for intravesical recurrence: (A) preoperative pyuria, (B) lymphovascular invasion (LVI), (C) diabetes mellitus (DM), and (D) tumorgrade.
|
Go to :
DISCUSSION
Many studies on prognostic biomarkers such as tumor stage, tumor grade, positive surgical margin, and LVI that affect the prognosis of UTUC have been conducted [456]. The functional relationship between inflammation and cancer is well documented. Many studies have shown that inflammation plays a crucial role in tumor development during various stages, from tumor initiation to promotion, malignant conversion, invasion, and tumor metastasis [1617]. Recently, a novel inflammatory index such as the neutrophil-to-lymphocyte ratio has been used as a prognostic factor in various malignancies, and several studies have reported that systemic inflammation has a significant association with IVR and poor prognosis of UTUC [101819]. Moreover, Tanaka et al. [20] reported the prognosis of UTUC using C-reactive protein as an inflammatory biomarker.
Previously, pyuria has been used as an indicator to reflect the inflammatory status of the urinary tract, such as urinary tract infection, genitourinary tuberculosis, urinary tract stone, autoimmune disease, interstitial cystitis, or urinary tract neoplasm [21]. Recently, pyuria has been regarded as a valuable prognostic indicator for urothelial carcinoma Azuma et al. [11] first reported that the presence of pyuria could be used as an indicator of recurrence and progression of NMIBC. Other researchers have also shown a significant association between preoperative pyuria and IVR in patients with NMIBC treated with TURBT and suggested the usefulness of pyuria as a prognostic factor in patients undergoing bacillus Calmette–Guérin therapy [1222].
In UTUC, preoperative pyuria has also been reported as a prognostic biomarker. Liang et al. [13] first reported the association between preoperative pyuria and UTUC prognosis. Their retrospective analysis indicated that preoperative pyuria was significantly associated with advanced pathologic T stage. In addition, pyuria has been described as an independent prognostic factor for postoperative survival. Yoshida et al. [14] also revealed that preoperative pyuria has a significant association with poor recurrence-free survival, cancer-specific survival (CSS), and OS in their multivariable analyses. Fukushima et al. [23] first reported that there was a significant relationship between preoperative pyuria and IVR in UTUC. However, they demonstrated that preoperative pyuria and bacteriuria (≥5 bacteria/HPF) were associated with a longer IVRFS, which was inconsistent with our findings. They suggested that bacteriuria and pyuria may have a protective effect against IVR after RNU. The reason for this result is assumed to be the inclusion of preoperative bacteriuria in their analysis. Also, they used a retrospective analysis of a relatively small study sample (97 patients). Milojevic et al. [24] recently published a study indicating that preoperative pyuria is not associated with bladder cancer recurrence and survival. In that study, multivariable analysis showed that preoperative pyuria was not significantly associated with IVR and CSS (p=0.56 and 0.79). However, in the univariate analysis, preoperative pyuria showed a tendency to be associated with IVR and CSS (p=0.01 and 0.02). Thus, a large-scale study may be required. To the best of our knowledge, the present study is the first to evaluate the prognostic value of preoperative sterile pyuria as an early sign of IVR in patients with UTUC, which may help clinicians in planning subsequent treatment after radical surgery.
The mechanism of preoperative pyuria as an indicator of the inflammatory status of the urinary tract affecting IVR has not yet been elucidated. Pyuria is a condition wherein the urine contains WBCs. Thus, neutrophils have a dominant role in IVR based on these findings. A high neutrophil count seems to be correlated with a pro-tumor inflammatory state reflecting an impaired tumor immunity and enhanced tumor promotion, which may be associated with an advanced tumor stage or grade. In addition, malignant transformation can be promoted through cytokines such as interleukin 6, tumor necrosis factor-alpha, and plasminogen activator inhibitor-1, in an inflammatory microenvironment [1719].
The preoperative finding that predicts IVR is useful in many ways. Ito et al. [25] indicated that early intravesical instillation of pirarubicin seemingly reduced IVR after surgery in UTUC in their prospective randomized phase II trial. Wu et al. [7] also reported in their meta-analysis that prophylactic intravesical instillation of chemotherapy can prevent IVR in patients with primary UTUC after surgery. Therefore, if IVR can be predicted post-surgery, patients who can be actively considered for early intravesical treatment after surgery may be selected. However, most of the prognostic factors that have suggested IVR in UTUC are related to pathologic findings. There are limitations to pathologic findings when selecting patients who need immediate treatment because of the time required for pathologic confirmation. Therefore, the fact that preoperative factors such as sterile pyuria are related with postoperative IVR can assist clinicians to decide on a suitable patient treatment strategy.
Although sterile pyuria was considered as a predictor of IVR in the current study, the concept of recurrence was limited only to the bladder. Basically, recurrence is defined as a tumor relapse in the surgical field or regional lymph node and/or distant metastasis, including urothelial carcinoma in the bladder or contralateral upper tract. In the present study, the T stage, tumor grade, LNI, LVI, and positive surgical margins had significant correlations (p-value of <0.05) in the univariate analysis, as in the study of Yoshida et al. [14]. Conversely, only LVI had a significant correlation in the multivariable analysis of OS. Furthermore, sterile pyuria had no significant association with OS in the Cox proportional hazards analysis in this study because the number of patients who died during the study was insufficient for statistical significance, due to censored survival data and a relatively short-term follow-up period. DM, high-grade tumor, and LVI, were also analyzed as independent factors for IVR in our study. Hu et al. [26] demonstrated that DM was a significant factor in the IVR of patients who underwent RNU. They revealed that there was an association with reduced antioxidative capacity and DM, and that oxidative stress could cause malignant transformations, such as genomic instability and DNA mutation. Although it was not analyzed as a significant factor in meta-analysis, high-grade tumors were analyzed as a predictive factor, as noted in the study published by Narukawa et al. [27] which reported that UTUC cells from multifocal and high-grade tumors might have intravesical implantation potential.
There are some limitations to this study. Firstly, the study has a retrospective design and is composed of data from two hospitals. Thus, a larger, prospective multicenter study is needed to validate our findings. Second, the surgeries were performed by multiple surgeons, and a selection bias such as each surgeon's surgical method and presence or absence of lymph node dissection may affect the oncological outcomes. Third, we defined the cut-off value of pyuria as ≥5 WBCs per HPF according to the study conducted by Hooker et al. [28] However, the cut-off value needs to be validated. Despite these limitations, preoperative pyuria is expected to be useful as a predictor of IVR because it can be easily identified using low-cost non-invasive tests.
Go to :
CONCLUSIONS
This study demonstrated that preoperative sterile pyuria is significantly associated with IVR in patients with UTUC undergoing surgery, but not associated with OS. Furthermore, DM, high-grade tumor, and LVI are also independent prognostic factors for these patients. Preoperative sterile pyuria in this cohort can be a useful prognostic factor for predicting IVR, and it will be helpful in determining the treatment or monitoring strategy of UTUC after surgery. A larger study cohort is required to determine the correlation between sterile pyuria and IVRFS in UTUC.
Go to :
 XML Download
XML Download