

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since its adoption in 2003, robot-assisted radical cystectomy (RARC) has been steadily increasingly used worldwide, as a minimally invasive alternative to open radical cystectomy (RC) with comparable perioperative and oncologic outcomes [12]. Recently, the International Robotic Cystectomy Consortium collected 2,125 RARC cases and reported that the use of intracorporeal urinary diversion (ICUD) increased from 9% in 2005 to 97% in 2015 (rate of increase, 11% per year) [3].
Recent studies have suggested that RARC improves perioperative morbidity and facilitates recovery, which would theoretically allow for an earlier initiation of adjuvant systemic therapies [45]. These benefits result from the robot-assisted surgery itself, which is, by definition, a minimally invasive technique. Presently, clinicians have been debating whether urinary diversion (UD) during RARC is best completed extracorporeally or intracorporeally [6789]. As most complications after RARC occur in association with UD, ICUD has been investigated as a way to reduce the rate of complications [10].
To maximize the advantages of minimally invasive surgery, a total ICUD approach may be a possible alternative. It is known that ICUD minimizes evaporative fluid loss; reduces the risk of fluid imbalance, estimated blood loss, and incisional pain; and restores bowel function more quickly [11]. However, despite these potential perioperative benefits, the use of ICUD has been criticized because there is uncertainty on whether it could be performed during surgery without increasing the rate of complications and whether it truly benefits the patient [12].
In this multicenter retrospective study, we analyzed the complications, perioperative outcomes after RARC with extracorporeal urinary diversion (ECUD) or ICUD, and oncologic outcomes in 362 patients with bladder cancer (BC).
Go to : 
MATERIALS AND METHODS
This retrospective cross-sectional study included 362 patients who underwent RARC with bilateral pelvic lymph node dissection (PLND) at 6 tertiary institutions between 2007 and 2017. A total of 6 surgeons from participating centers performed the procedures, and all of them were experts who had performed >30 RARCs. Of them, 4 surgeons performed ECUD only and 2 surgeons performed both ICUD and ECUD. The final patient cohort consisted of 278 patients who underwent ECUD and 84 patients who underwent ICUD. This study conformed to the standards of the Declaration of Helsinki and current ethical guidelines, and was approved by the Institutional Review Board of Korea University Anam Hospital (approval number: ED10120). The need for informed consent was waived by the board.
1. Inclusion and exclusion criteria
The study participants included patients with muscleinvasive BC or recurrent high grade non muscle invasive BC [13]. We excluded patients with stage cM1 disease, prior extensive abdominal surgery, complicated surgery or any contraindication to the Trendelenburg position. Tumor/pathologic grade were determined according to the TNM staging system and the 2004 World Health Organization/International Society of Urologic Pathologists classification of papillary urothelial neoplasms, respectively [14]. All research and data collection followed the tenets of the Declaration of Helsinki.
2. Primary endpoints
The primary endpoints were the complication rates. Comparisons were made in accordance with the standardized complications within 90 days of surgery (reported using the Clavien–Dindo classification). The specific complications that were investigated in each complication group were depicted as follows: infectious—urinary tract infection, peritonitis, and fever; respiratory—pneumonia and pulmonary embolism; gastrointestinal—ileus (mechanical and paralytic), jaundice, and hematochezia; procedure related—transfusion, incisional hernia, bowel injury, and lymphocele; genitourinary—hydronephrosis, uretero-ileal anastomosis site stricture/leakage, and scrotal edema; nervous—obturator injury; vascular—heart failure. In addition, we selected and compared 2 surgeons who could be representative of each group (1 for ECUD and 1 for ICUD). Each surgeon has mastered the learning curve by performing >100 RARCs [6]. A total of 75 operations (150 cases) were performed by each surgeon during the same period. The types of complications were described in detail, and statistical differences were analyzed.
3. Secondary endpoints
The secondary endpoints included perioperative parameters, recurrence patterns, and oncologic outcomes. Perioperative recovery parameters included time to passage of flatus, time to starting oral intake (from liquid diet), time to urinary catheter removal, and length of hospital stay. Then, the recurrence pattern after RARC with ECUD or ICUD was studied. The recurrence type was divided into local and distant, and the specific prevalence of recurrence was determined. Furthermore, for the analysis of oncologic outcomes, margin positivity rates and 2-year recurrence-free survival (RFS) rates were analyzed. Recurrence was defined as the time from cystectomy to local or metastatic recurrence, based on histologic or radiologic evidence.
4. Statistical analysis
Continuous variables were expressed as mean±standard deviation, and 1-way analysis of variance was used for the analysis. Additionally, Pearson chi-square test and Fisher exact test were used for analyzing data. The estimated distribution of RFS was obtained using Kaplan-Meier analysis, and the log-rank test was used to compare the Kaplan-Meier curves between the groups. All analyses were performed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). Results were considered statistically significant if the p-value was less than 0.05.
Go to :
RESULTS
The mean duration of follow-up was 34.7±25.5 months. We observed no difference in age, sex, body mass index, incidence of previous abdominal surgery, incidence of neoadjuvant chemotherapy, and type of UD (ileal conduit or orthotopic neobladder substitution) between the 2 groups. In the ICUD group, the rate of performing extended PLND was significantly higher than that of standard PLND (p<0.001) (Table 1).
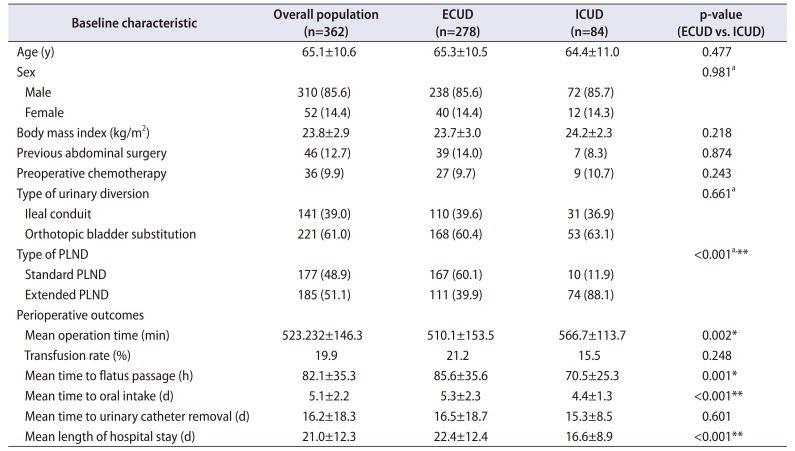
Table 1
Baseline patient characteristics and perioperative parameters
![]()
1. Complications I
In the ECUD group, 171 patients (61.5%) experienced at least 1 complication of any grade within 90 days of surgery, whereas there were 35 such patients (41.7%) in the ICUD group (p=0.001). In the analysis of overall complication and major complication rates (grade 3–5), there were no significant differences between the 2 groups. The incidence of gastrointestinal complications in the ICUD group showed a decreasing trend (p=0.036), and there were no major complications in the ICUD group. The incidence of genitourinary complications was also lower (p=0.036) in the ICUD group (Table 2). In the analysis of complication rates in the genitourinary tract, there were significant differences between the 2 groups (p=0.036). In terms of the type of complication, hydronephrosis (20 of 28) was the most common, followed by acute kidney injury (5 of 28), urinary stone (2 of 28), and bladder neck stricture (1 of 28).
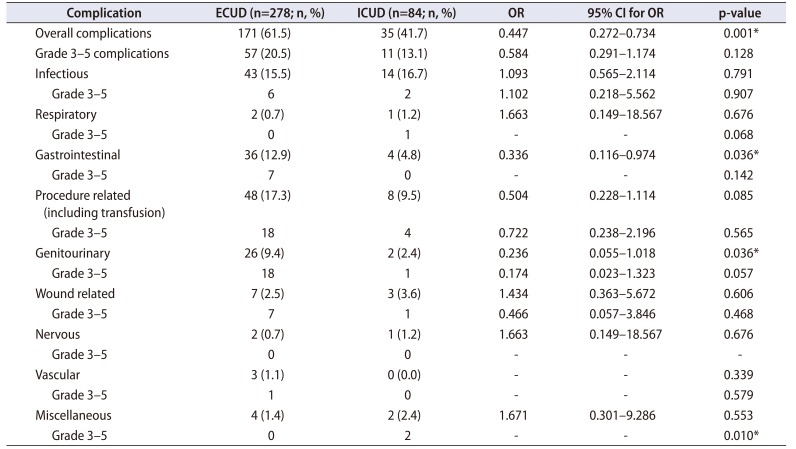
Table 2
Overall 90-day complications defined according to a modified Clavien system (grade 1–5)
![]()
2. Complications II
We performed a head-to-head comparison between 2 expert surgeons from each group. The total complication and major complication rates showed no difference, whereas the minor complication rates showed a decreasing trend in the ICUD group (ECUD vs. ICUD: 31 [41.3%] vs. 20 [26.7%], p=0.058). The urine leakage rates were significantly lower (ECUD vs. ICUD: 9 [12.0%] vs. 0 [0.0%], p=0.002) in the ICUD group (Table 3).
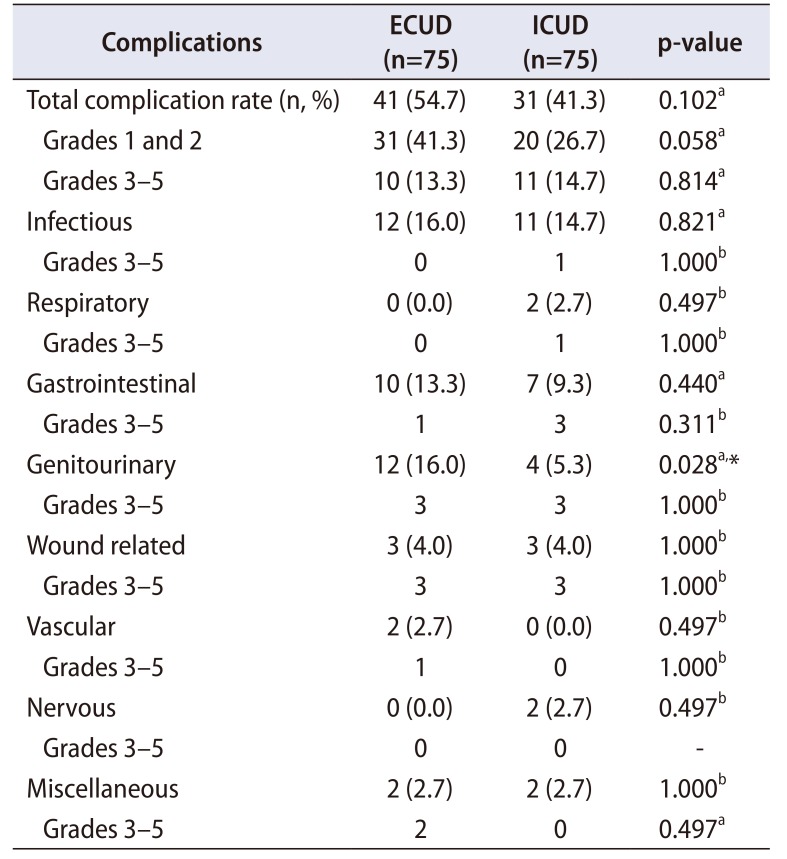
Table 3
Comparison of complication (defined according to a modified Clavien system) rates between ECUD and ICUD performed by 2 expert surgeons (experienced with >100 RARC cases)
![]()
3. Perioperative parameters
The ICUD group had significantly longer total operation time and console time, whereas the postoperative transfusion rate showed no difference (21.2% vs. 15.5%, p=0.248). Recovery parameters, such as mean time to passage of flatus, start of oral intake, and length of hospital stay, were significantly shorter in the ICUD group than in the ECUD group (p=0.001, p<0.001, and p<0.001, respectively), except for the mean time to Foley catheter removal (p=0.601) (Table 1, Fig. 1).
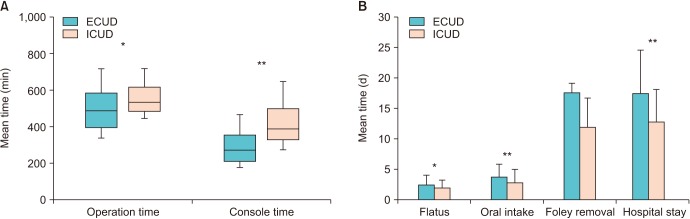 | Fig. 1Comparison of perioperative valuables between the extracorporeal urinary diversion (ECUD) and intracorporeal urinary diversion (ICUD) groups. (A) Total operation time and console time and (B) recovery parameters (time to flatus, time to oral intake, time to urinary catheter removal, and length of hospital stay). *p<0.05, **p<0.001.
|
4. Recurrence patterns
Local/distant recurrence occurred in 10 (3.6%) and 25 (9.0%) patients in the ECUD group and in 2 (2.4%) and 7 (8.3%) patients in the ICUD group, respectively. Concerning both types of recurrence, there were no significant differences in the recurrence pattern between the 2 groups. Only 3 patients experienced recurrence of secondary urothelial carcinoma in the upper urinary tract (2 patients) and urethra (1 patient). The diversion of recurrence locations is shown in Table 4.
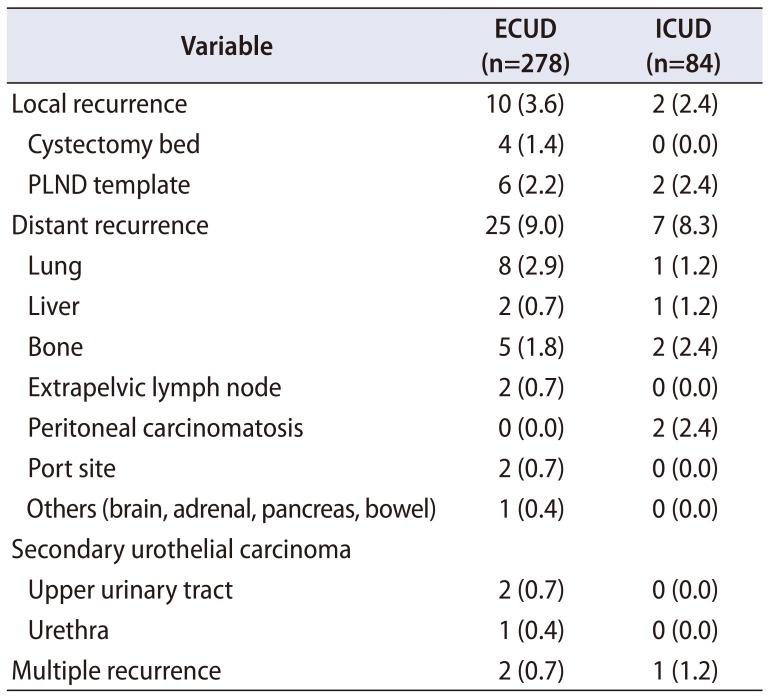
Table 4
Distribution of recurrence locations among patients with recurrence after RARC with ECUD or ICUD
![]()
5. Oncologic outcomes
There was no difference in the margin positivity rate (p=0.944). In pathologic results, there were no differences between the 2 groups in numbers of lymph-node-positive patients (p=0.523), lymph node density (p=0.127), and pathologic tumor stage or nodal stage (p=0.152, p=0.116). The lymph node yield was significantly higher in the ICUD group than in the ECUD group (29.8±13.6 vs. 15.1±12.1, p<0.001). The 2-year RFS showed no significant difference between the 2 groups (ECUD vs. ICUD: 83.2% vs. 88.6%, p=0.496) (Table 5).
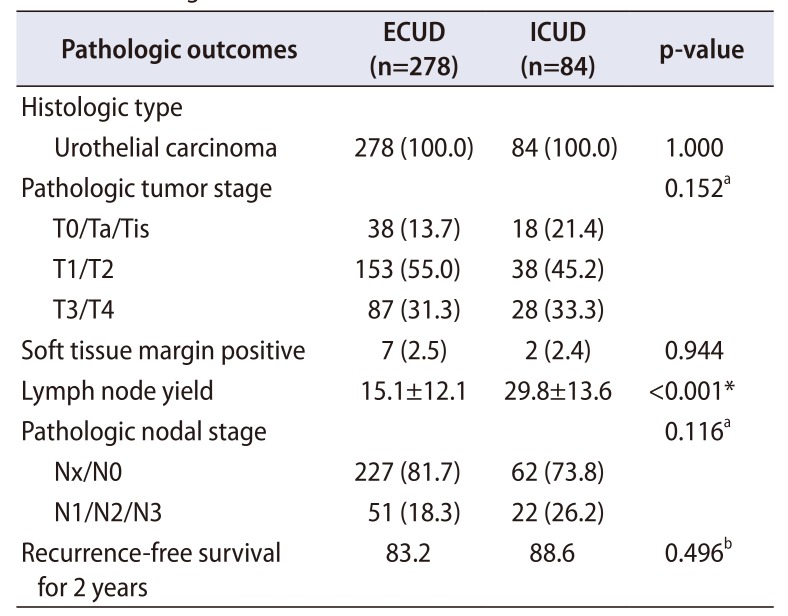
Table 5
Oncologic outcomes
![]()
Go to :
DISCUSSION
The aim of our study was to determine whether ICUD has clinical benefits compared with ECUD. Our results suggest that the ICUD approach is beneficial in terms of lower complication rates and better perioperative outcomes, as indicated by recovery parameters, while maintaining similar oncologic outcomes to those of ECUD.
Our study showed a significant advantage of ICUD over ECUD for patients with regard to overall complication rates and gastrointestinal-related complications. The International Robotic Cystectomy Consortium conducted a comparative analysis of ICUD and ECUD. Overall, a trend favoring ICUD over ECUD was noted (41% vs. 49%, p=0.05). Gastrointestinal complications were significantly lower in the ICUD group (p<0.001). Additionally, Bochner et al. [12] reported that the most common complications during cystectomy were gastrointestinal-, infection-, and wound-related problems in their prospective study. Complications related to bowel resection are undoubtedly one of the biggest problems faced by urologists and an important reason for prolonged hospital stays. In this regard, the exposure time of the peritoneum to external air was proportional to intestinal inflammation and oxidative stress response in experimental models using white rats. This leads to intestinal paralysis or intestinal obstruction and delayed restoration of bowel function [15]. Other studies comparing laparoscopy and laparotomy in bowel surgery have shown a decrease in the levels of cytokines, including interleukin (IL)-1, IL-6, and tumor necrosis factor-alpha, and a reduction in systemic immunosuppression in endoscopic surgery as compared with open surgery [1516].
In our study, the ICUD group showed a decreasing trend of genitourinary complications, which consisted mostly of urinary leakage or anastomosis site stricture. Furthermore, as shown in Table 5, in the analysis of the surgeons who overcame the learning curve, lower minor complication rates were found in the ICUD group in terms of ureteral complications, whereas the major complication rates were similar. ECUD requires more ureteral mobilization and longer ureteral length, which can result in ureteral redundancy, kinking, and devascularization [10]. On the other hand, in the ICUD approach, anastomoses are made at the position, resulting in less ureter mobilization and tension. In several large ICUD series, a low stricture rate of approximately 3% was reported [1718].
Considering the potential advantages of ICUD, patients undergoing RC are often older and have several comorbidities, which are risk factors for increased complications [19]. There is evidence that RARC may have an advantage in reducing the surgical stress response compared with open surgery in older patients or other vulnerable patients [2021]. Reduction in the stress response can be achieved through minimal-access surgery [22]. These concepts are in line with the benefits of ICUD, such as minimizing the handling time of organs in the abdominal cavity, as well as decreasing bowel manipulation/exposure and reducing insensible fluid losses [2324]. Our results showed a relatively shorter length of stay (days) in patients who underwent ICUD than in those who underwent ECUD (16.6±8.9 vs. 22.4±12.4, p<0.001), as well as shorter time to passage of flatus and time to starting oral intake. Improvements in recovery parameters are especially important in elderly patients with comorbidities who undergo RARC. There is increasing evidence showing that patients who are susceptible to the morbidity of major surgery may be the ones who will benefit from a robotic approach [20].
In the analysis of recurrence patterns, the overall rates of local and distant recurrence did not show any difference between the 2 groups. With respect to incidence of distant recurrence of solid organs, lung, bone and liver remain the most frequent sites and homologous to previous studies [25]. The incidence rates of peritoneal carcinomatosis and port site recurrence were not significantly different between the 2 groups. Although no statistically significant differences were found, more attention is needed to avoid urine leakage when performing the procedure (after removing the specimen and transferring it into the endopouch). This is important because the follow-up strategy should reflect the risk of extravesical recurrence [26], and this type of recurrence was observed in the ECUD group only.
Despite several potential perioperative benefits, the use of RARC has been criticized owing to the paucity of reports about a few oncologic concerns. According to the data available to date, RARC can implement adequate PLND in terms of its territory and yield, and has an acceptable positive surgical margin (PSM) rate. In addition, it is possible to avoid urine leakage or inadvertent bladder injury and safely perform the surgery while adhering to the oncologic principles. Furthermore, it showed similar results to those of an open series in patients with mostly T3 or higher stages. In our study, the PSM (p=0.944) and lymph-node-related factors did not differ, except that the lymph node yield and short-term RFS (p=0.496) did not show inferior results to those of ECUD. Although ICUD remains a complex procedure, the outcomes of this study agree with those of previous studies, thereby demonstrating the potential benefits of ICUD after RARC. This will contribute to ICUD gaining popularity as a viable alternative to ECUD. Theoretically, there is no difference in the oncologic outcome between ECUD and ICUD. Nevertheless, the reason why we evaluated the oncologic outcome is that there is a slight procedural difference between the 2 methods after a cystectomy. In the case of ICUD, the time during which the specimen stays inside the body is inevitably longer, according to the surgical principle. Accordingly, precaution is needed because of the possibilities of local tumor spillage and urine leakage even after removing the specimen.
There are some limitations in this study. First, the medical records of consecutive patients were retrospectively reviewed. The number and timing of operations performed in each surgeon are different, and this may have affected the outcome of our study. Therefore, this study is limited by biases such as lack of randomization, patient selection bias. Better designed research would be needed in the future.
Go to :
CONCLUSIONS
In this multicenter trial, there were decreasing trends in overall, gastrointestinal, and genitourinary complications in the ICUD group. The ICUD group showed significantly improved recovery parameters compared with the ECUD group. Analysis of oncologic outcomes at intermediate-term follow-up revealed no differences in the PSM rate, recurrence pattern, or RFS between the 2 UD techniques. In the future, the results of prospective, randomized controlled trials between RARC and open RC are awaited to confirm the current findings.
Go to :
 XML Download
XML Download