

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Septic shock is a life-threatening complication of infection that has increased in incidence in the past 15 years.1 Pathogenically, septic shock is characterized by hypovolemia and decreased vascular resistance, leading to arterial hypotension and multiple organ dysfunctions.2 Therefore, fluid expansion and catecholamines are crucial for hemodynamic stability and adequate perfusion to vital organs.3 However, high doses of norepinephrine (NE) often fail to reverse shock, and arginine vasopressin (AVP) can be added with the intent of either increasing mean arterial pressure (MAP) or decreasing NE dosage.3 The rationale behind AVP use is its vasoconstrictive action and its ability to correct the deficiency of naturally occurring AVP in septic shock.4 Given these characteristics, there has been increasing interest in early AVP treatment as an adjunct to NE,56 although the evidence of a clinical benefit of AVP is weak.3
Once vascular tone begins to return to normal, vasopressors are gradually tapered,7 which can decrease the adverse events from long-term use of vasopressors.89 Even in the recovery phase, clinically significant hypotension after discontinuation of vasopressors has been seen10111213141516 and can cause subsequent organ injury.17 Therefore, during the discontinuation of vasopressors, clinicians should consider both the risks for adverse events from continuous infusion of vasopressors and subsequent development of hypotension from discontinuation of infused vasopressors. The current Surviving Sepsis Campaign guidelines recommend NE as the initial vasopressor of choice, with AVP as a second-line adjunct.3 However, there has been no consensus regarding the safe discontinuation order of vasopressors in the recovery phase of septic shock.1213141516
Therefore, we performed a systematic review of the incidence of hypotension within 24 hours based on the discontinuation order of NE and AVP in patients recovering from septic shock, and we examined, as a secondary objective, whether the discontinuation order of vasopressor influenced patients' outcomes.
METHODS
Data sources and search strategy
The present meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.18 We performed a search of electronic databases, MEDLINE, Embase, and Cochrane Library. All searches for studies published in English were conducted from inception through to April 7, 2018. We used the following keywords: “vasopressors or arginine vasopressin or norepinephrine, vasoactive agents,” “discontinuation or tapering or withdrawal,” and “sepsis or septic shock.” We investigated reference lists of every article and performed a manual search of the references listed in the relevant review articles.
Inclusion and exclusion criteria
Studies were included in this meta-analysis if they met the following inclusion criteria: 1) a randomized controlled or non-randomized cohort study that directly compared NE and AVP for discontinuation of vasopressors; 2) adult patients (i.e., 18 years or older) with a diagnosis of septic shock; 3) reported the incidence of hypotension within 24 hours after the discontinuation of one of two vasopressors; and 4) reported the risk estimates and 95% confidence intervals (CIs) or the information from which these could be calculated. We considered studies published as full-length articles or letters in peer-reviewed English language journals. Review articles, case reports, abstracts, and commentaries were excluded. The full details of the electronic search strategy are available in the Supplementary Data 1 and 2.
Data extraction and quality assessment
Two authors independently retrieved potentially relevant studies, reviewed each study according to the predefined criteria for eligibility, and extracted data. Any discrepancies that arose during the process of study selection or data extraction were resolved by discussion. A predefined form was used to extract data from each study. We extracted all available data as outlined in the form, including characteristics of the included studies, details of the population enrolled, and outcome measures. The primary outcome was incidence of hypotension within 24 hours after discontinuation of vasopressors. Secondary outcomes were intensive care unit (ICU) mortality, in-hospital mortality, 28-day mortality, and ICU length of stay. Methodological quality and risk of bias were evaluated for each trial using the Newcastle-Ottawa quality assessment for non-randomized studies.19 Discrepancies were resolved by consensus between the two authors.
Data synthesis and statistical analysis
All analyses were conducted using weighted frequencies for categorical variables and weighted means and ranges for continuous variables, with the weight corresponding to the sample size of each study. We extracted the risk ratios (RRs) and mean differences with associated 95% CIs for clinical outcomes after discontinuation of two vasopressors, and calculated the pooled relative risk using the Mantel-Haenszel method. Between-study statistical heterogeneity was assessed using I2 and Cochran's Q test.20 Heterogeneity was assessed using I2 statistics on a scale of 0%–100%. A fixed-effects model was used unless I2 was > 50%, indicating a substantial level of between-study heterogeneity, in which case a random-effects model was used.20 If evidence of substantial heterogeneity was found, stratified analyses via meta-regression were performed to identify the factors that contributed to the heterogeneity.21 When the number of enrolled studies was more than 10, publication bias for the primary outcome was assessed using Egger's regression tests.22 The level of statistical significance for the two-tailed test of each hypothesis was 0.05. Statistical analyses were performed using Stata statistical software (version 14.2; StataCorp LLC, College Station, TX, USA) and Review Manager (version 5.3; Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark).
RESULTS
Study search and characteristics and quality of included studies
A total of 128 published articles were initially identified (74 articles from MEDLINE, 20 articles from Embase, and 33 articles from the Cochrane library) (Fig. 1). After the literature search process, five studies1213141516 were included in our final analysis. Table 1 summarizes the features of the included studies. The total number of patients in our systematic review and meta-analysis was 930, of whom 631 (67.8%) discontinued NE first and 299 (32.2%) discontinued AVP first. All studies were single center, retrospective cohort studies and published between 2010 and 2018. Assessment of quality is presented in Table 2. All studies were considered to be high quality. However, publication bias could not be assessed because the number of studies was less than 10.
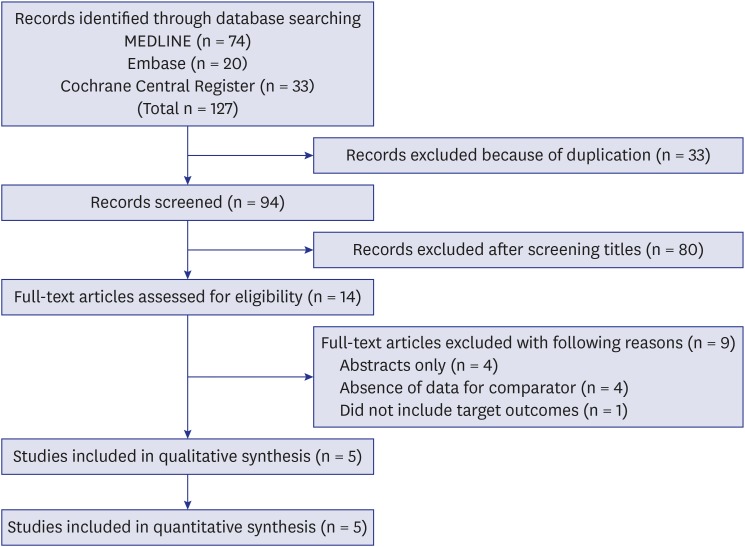
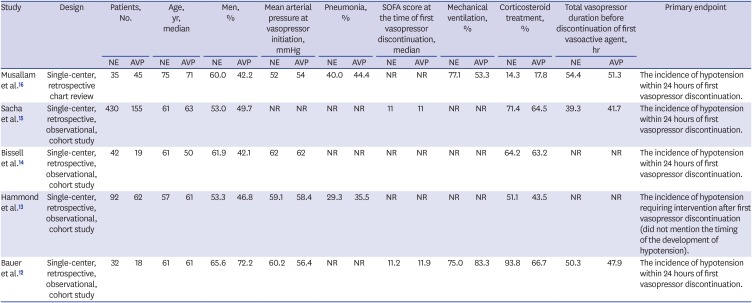
Table 1
Characteristics of the studies included in the meta-analysis
| Study | Design | Patients, No. | Age, yr, median | Men, % | Mean arterial pressure at vasopressor initiation, mmHg | Pneumonia, % | SOFA score at the time of first vasopressor discontinuation, median | Mechanical ventilation, % | Corticosteroid treatment, % | Total vasopressor duration before discontinuation of first vasoactive agent, hr | Primary endpoint | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NE | AVP | NE | AVP | NE | AVP | NE | AVP | NE | AVP | NE | AVP | NE | AVP | NE | AVP | NE | AVP | |||
| Musallam et al.16 | Single-center, retrospective chart review | 35 | 45 | 75 | 71 | 60.0 | 42.2 | 52 | 54 | 40.0 | 44.4 | NR | NR | 77.1 | 53.3 | 14.3 | 17.8 | 54.4 | 51.3 | The incidence of hypotension within 24 hours of first vasopressor discontinuation. |
| Sacha et al.15 | Single-center, retrospective, observational, cohort study | 430 | 155 | 61 | 63 | 53.0 | 49.7 | NR | NR | NR | NR | 11 | 11 | NR | NR | 71.4 | 64.5 | 39.3 | 41.7 | The incidence of hypotension within 24 hours of first vasopressor discontinuation. |
| Bissell et al.14 | Single-center, retrospective, observational, cohort study | 42 | 19 | 61 | 50 | 61.9 | 42.1 | 62 | 62 | NR | NR | NR | NR | NR | NR | 64.2 | 63.2 | NR | NR | The incidence of hypotension within 24 hours of first vasopressor discontinuation. |
| Hammond et al.13 | Single-center, retrospective, observational, cohort study | 92 | 62 | 57 | 61 | 53.3 | 46.8 | 59.1 | 58.4 | 29.3 | 35.5 | NR | NR | NR | NR | 51.1 | 43.5 | NR | NR | The incidence of hypotension requiring intervention after first vasopressor discontinuation (did not mention the timing of the development of hypotension). |
| Bauer et al.12 | Single-center, retrospective, observational, cohort study | 32 | 18 | 61 | 61 | 65.6 | 72.2 | 60.2 | 56.4 | NR | NR | 11.2 | 11.9 | 75.0 | 83.3 | 93.8 | 66.7 | 50.3 | 47.9 | The incidence of hypotension within 24 hours of first vasopressor discontinuation. |
Table 2
Quality assessment for the studies included in the meta-analysis

| Study | Selection of exposed and non-exposed cohorts | Comparability | Outcome of interest | Overall qualitya | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of exposed cohort | Selection of non-exposed cohort | Ascertainment of exposure | Outcome present at start of study | Comparability of cohorts | Assessment of outcome | Length of follow-up | Adequacy of follow-up | ||
| Musallam et al.16 | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | High |
| Sacha et al.15 | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | High |
| Bissell et al.14 | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | High |
| Hammond et al.13 | ★ | ★ | ★ | ★ | ★ | ★ | NR | NR | High |
| Bauer et al.12 | ★ | ★ | ★ | ★ | ★ | ★ | ★ | ★ | High |
Primary outcome
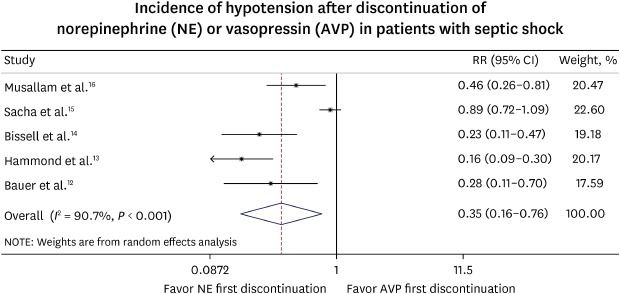
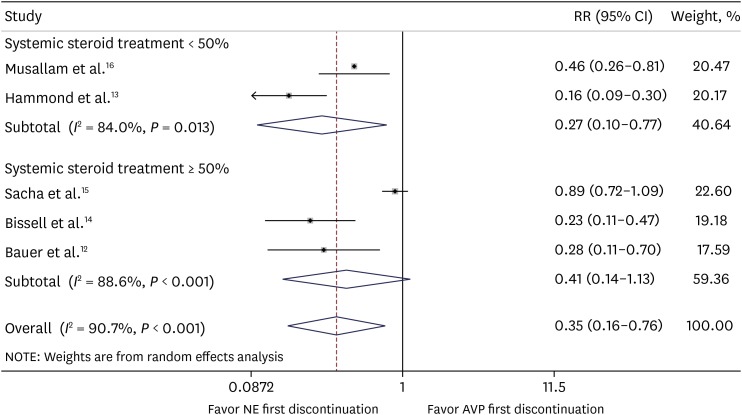
A forest plot of primary outcome, effect of first discontinuation of NE or AVP at endpoint on incidence of hypotension, is shown in Fig. 2. Overall, a random effect model showed that discontinuation of NE first resulted in a significant reduction in incidence of hypotension compared with discontinuation of AVP first (31.8% vs. 54.8%; RR, 0.35; 95% CI, 0.16–0.76; P = 0.008; I2 = 90.7%) (Fig. 2). Because a substantial degree of heterogeneity existed among the trials, the meta-regression technique was used to explore heterogeneity. Specifically, we performed stratified meta-regression analyses in accordance with the study year (≥ 2015 vs. < 2015), age of the patients (≥ 60 vs. < 60 years), and use of systemic steroid treatment (≥ 50 vs. < 50% of the patients), and we did not observe any significant factor (Table 3).
Fig. 2
Paired forest plots of RRs for the incidence of hypotension according to vasoactive agents discontinuation in patients with septic shock.
RR = risk ratio, CI = confidence interval, NE = norepinephrine, AVP = arginine vasopressin.
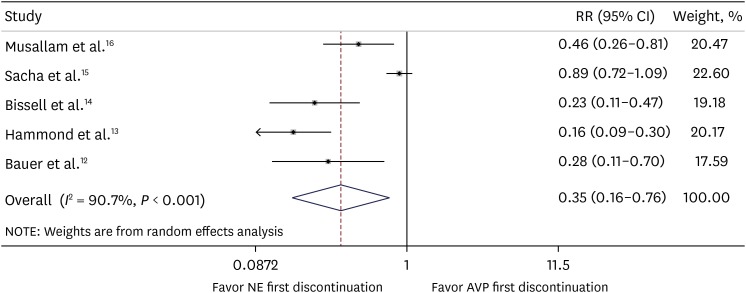
Table 3
Meta-regression analysis performed using the model weighted by the inverse of the variance

In a subgroup analysis for the use of systemic steroid treatment in < 50% of the enrolled patients, discontinuation of NE first resulted in significant reductions in incidence of hypotension compared with discontinuation of AVP first (15.7% vs. 65.4%; RR, 0.27; 95% CI, 0.10–0.77; P = 0.015; I2 = 84.0%) (Fig. 3). On the other hand, a subgroup analysis for use of systemic steroid treatment among ≥ 50% of patients revealed that incidence of hypotension was not significantly different between two groups (36.5% vs.49.0%; RR, 0.41; 95% CI, 0.14–1.13; P = 0.085; I2 = 88.6%) (Fig. 3).
Secondary outcome
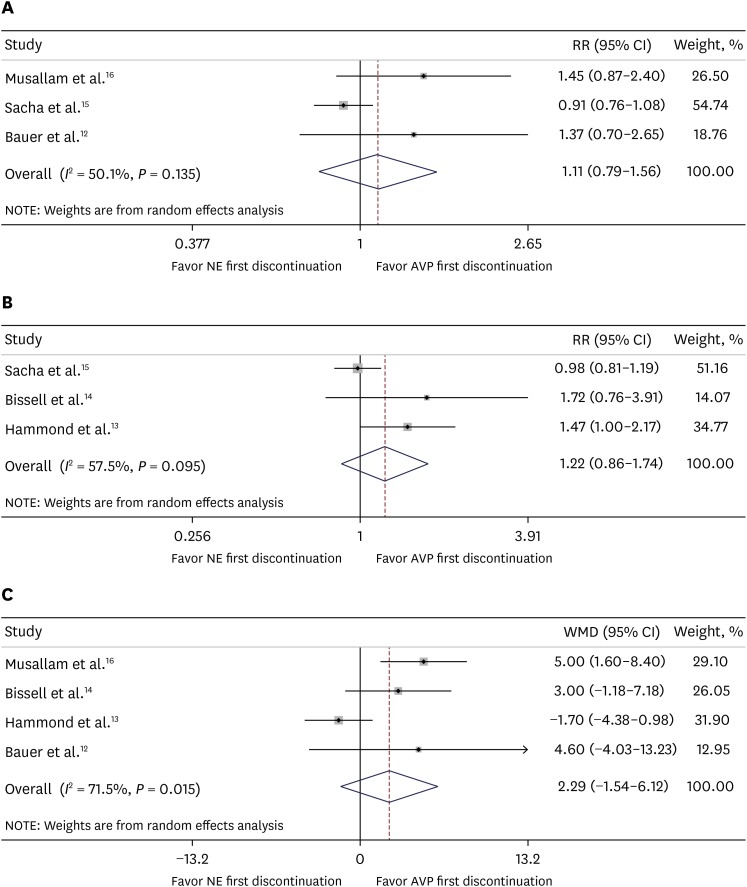
Three trials with a total of 715 patients compared ICU mortality between NE first and AVP first discontinuation group in patients with septic shock.121516 In pooled estimates, ICU mortality was 50.1% and 49.5% in the NE-first and the AVP-first groups, respectively. The pooled estimates using a random effect model demonstrated that ICU mortality was not significantly different between the two groups (RR, 1.11; 95% CI, 0.79–1.56; P = 0.555; I2 = 50.1%) (Fig. 4A). Also, no significant difference was found between the NE first and the AVP first group in in-hospital mortality (48.0% vs. 43.2%; RR, 1.22; 95% CI, 0.86–1.74; P = 0.266; I2 = 57.5%) (Fig. 4B).131415 We retrieved data concerning ICU length-of-stay according to two strategies from four studies,12131416 and there was no significant difference in ICU length-of-stay between the NE-first group and the AVP-first group (mean difference, 2.29 days; 95% CI, −1.54–6.12; P = 0.241; I2 = 71.5%) (Fig. 4C).
Fig. 4
Paired forest plots of RRs for clinical outcomes according to vasoactive agent discontinuation in patients with septic shock; (A) ICU mortality, (B) in-hospital mortality, and (C) the mean difference (day) in ICU length of stay.
RR = risk ratio, CI = confidence interval, NE = norepinephrine, AVP = arginine vasopressin, WMD = weighted mean difference, ICU = intensive care unit.
DISCUSSION
In the present study, we found that discontinuing NE before AVP led to a lower incidence of hypotension in patients recovering from septic shock on concomitant NE and AVP. However, a substantial degree of heterogeneity existed among the trials. Although we conducted a meta-regression to explore heterogeneity, we did not observe any specific significant factors of bias.
Possible explanations for potential sources of bias may be considered, such as the following. The first is the timing to discontinuation of vasopressors considering the onset of an AVP deficiency. Patients who were included in a retrospective large cohort experienced a shorter time to discontinuation of vasopressors compared to other studies.15 That study reported no significant difference in the incidence of hypotension based on discontinuation order of vasopressors.15 In contrast, the remaining four retrospective studies demonstrated that discontinuing AVP first led to a higher incidence of hypotension.12131416 These conflicting results could be explained by the onset time of the AVP deficiency in septic shock. An AVP deficiency contributes to a decreased response to hypotension and enhanced sensitivity to infused AVP.1025 These characteristics of AVP in septic shock may be more beneficial than NE for hemodynamic stabilization, especially in patients with AVP deficiencies. Theoretically, during AVP deficiency, endogenous AVP production and function are muted. Before AVP deficiency is restored, discontinuation of exogenous AVP may result in hypotension.2627 However, the exact onset time of AVP deficiency has not been clearly determined.2728 According to previous studies, plasma AVP levels was increased during the first 24–36 hours of septic shock,82728 and most patients exhibit a relative AVP deficiency after 36 hours following onset of shock.27 In this regard, discontinuation of AVP first could be associated with an increased risk of hypotension with a time-varying effect that decreases over time.1415 Therefore, AVP discontinuation after 36 hours of septic shock onset could be extremely sensitive to the development of hypotension.
In subgroup analysis for the use of systemic steroid treatment ≥ 50% of the patients, the effect of the discontinuation order of NE and AVP were suppressed. Corticosteroids increase AVP messenger RNA29 and plasma level of AVP.23 This might be associated with the primary outcome between the two groups, especially in the NE discontinuation first group. Therefore, interaction of AVP and corticosteroid treatment should be considered.232429
Finally, there is the speed of discontinuation of vasopressors. Discontinuation practice in which vasopressors are titrated or ceased was inconsistent between study institutions. Although the practice for discontinuation of vasopressors was difficult to elucidate, AVP is most frequently ceased without tapering and is sometimes decreased to half of the dose for a short period of time and then discontinued, as opposed to NE, which is gradually reduced. This potentially dramatic adjustment in AVP may have led to a higher incidence of hypotension after discontinuation of AVP, despite the longer effective half-life of AVP (10–20 minutes) compared to NE (2–2.5 minutes).30 Moreover, in the five retrospective studies, the incidence of hypotension was markedly different in patients who discontinued NE first (11%–50%) than in those who discontinued AVP first (55%–74%).1213141516 This difference was likely caused by center-specific variations in the rate of NE titration. This could also affect the difference in the primary outcome between studies. Therefore, we believe that these center-specific practice variations with vasopressors could be one of the reasons why the incidence of hypotension after discontinuation was different among studies. Considering the variations in discontinuing method of vasopressors, we suggest a future randomized controlled trial on the incidence of hypotension with vasopressor discontinuation.
In contrast to the findings from these observational studies, a recent prospective randomized controlled study (DOVSS) on the incidence of hypotension during vasopressor tapering showed that NE tapering more likely led to hypotension than did AVP tapering.31 However, the primary endpoint of the DOVSS study was the incidence of hypotension within one hour of tapering the first vasopressor from the predefined dose of both NE (0.3 mcg/kg/min) and AVP (0.03 U/min). As the study protocol, NE was titrated first to 0.3 mcg/kg/min in all participants. In addition, hypotension developed during vasopressor tapering was included in the study. Therefore, we did not include the DOVSS study in our meta-analysis on the incidence of hypotension within 24 hours after discontinuation of NE or AVP.
Our results add useful information regarding discontinuation of vasopressors in the recovery phase of septic shock. However, the potential limitations of our study should be considered. First, our meta-analysis was performed with a small number of trials, which limits the generalizations of our findings. Therefore, current results should be interpreted with caution, and further large-scale randomized controlled trials should be conducted to substantiate our findings. Second, there was statistically significant heterogeneity in the selected studies. Although we explored the heterogeneity using stratified meta-regression, we failed to identify the source of bias. Third, although our literature search procedures were extensive, other trials may have appeared or may not have been published, which could have affected the findings. Finally, myocardial dysfunction was not considered in our study. Because myocardial dysfunction is a very common and severe complication of septic shock, this factor may influence our results.32 Therefore, further studies using advanced monitoring for cardiac function are needed.
In conclusion, our study demonstrated that discontinuing NE before AVP led to a lower incidence of hypotension within 24 hours in patients recovering from septic shock, although between-study heterogeneity was high in the current study. In addition, there were no differences in ICU mortality, in-hospital mortality, and ICU length-of-stay between the two groups.
 XML Download
XML Download