

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Glycogen storage disease (GSD) is an inherited metabolic disease caused by deficiency in various enzymes that are related to glycogenolysis and gluconeogenesis. The most common type, GSD Ia, is an autosomal recessive disorder that leads to abnormal glucose metabolism and glycogen accumulation induced by the defect of glucose-6-phosphatase.12 This condition is associated with various complications such as hyperuricemia, hyperlipidemia, hypoglycemia, and failure to thrive. Among the long-term complications, hepatocellular carcinoma (HCC) is the most severe and fatal.12345
To date, there are few cohort studies on GSD with long-term follow-up, especially concerning the development of GSD adenoma and HCC. The pathogenesis of hepatic adenoma and HCC in patients with GSD has not yet been clearly identified.2345678 It has been well known that good metabolic control in patients with GSD results in lower chance of development of hepatic adenoma. Other studies, however, reported that there is a clear risk of hepatic adenoma in patients with GSD even under good metabolic control.345678 Then a question can arise what possible risk factors would work in the development of hepatic adenoma and/or its malignant transformation. The question could be related with a possible pathophysiology of adenoma and HCC in GSD.
This retrospective cohort study focused on the risk factors and the natural course of hepatic adenoma and HCC formation in patients with GSD.
METHODS
A total of 72 patients were enrolled from March 1982 to September 2013 at Seoul National University Children's Hospital and were reviewed retrospectively. The follow-up period was a median of 19.2 years (range, 9.7–27.2 years).
The diagnosis of GSD was based on symptoms and signs consistent with the disease, as well as with compatible pathologic findings both on light microscopy and electron microscopy. Liver biopsy was performed in all patients for pathologic diagnosis. An increased amount of glycogen in the liver parenchyma was considered to be the positive pathologic finding. Molecular genetic testing was conducted in 62 patients (86.1%) to confirm the GSD type.
For the diagnosis of hepatic adenoma and HCC, we followed up all patients with abdominal radiologic evaluation through ultrasonography, computed tomography (CT), or magnetic resonance imaging (MRI). Routine radiologic examination was usually done with ultrasonography on a regular interval of 6–12 months. For hepatic adenoma, regular imaging follow-up was usually done with ultrasonography; if the number or size of adenoma increased, CT or MRI was done. Even before the development of hepatic adenoma, we checked for the patients with ultrasonography at least once a year. After the development of hepatic adenoma, we followed-up hepatic adenoma for any change with 6- or even shorter interval if needed. Liver biopsy for adenoma was performed in 15 patients (46.8%), and 8 of 15 patients (53.3%) underwent surgical biopsy and pathologic evaluation at the time of liver transplantation.
We evaluated the biochemical profiles of all patients, including complete blood count; liver function; blood sugar level; uric acid level; and lipid profiles including triglycerides, cholesterol, high-density lipoprotein, and low-density lipoprotein. Considering that hepatic adenoma and HCC are long-term complications of hepatic glycogenosis, alpha-fetoprotein (aFP) levels were assessed regularly in all patients. We checked for AFP regularly like 2 to 3 months interval with other biochemical markers through blood sampling prior to HCA and the interval was adjusted shorter after the development of hepatic adenoma. To rule out viral infection of the liver, hepatotropic viral markers for hepatitis A, B, C, and D and for cytomegalovirus were screened in all patients at the time of investigation before the initial diagnosis of GSD to screen out the possibility of infection as the cause of the elevation of transaminase or of hepatomegaly.
We also checked for the patient's growth at the diagnosis and regularly thereafter, and the short stature meant that the height standardized for age and sex was less than 3 percentile.
Statistical analysis was conducted using SPSS Statistics 21.0 (SPSS Inc., Chicago, IL, USA). Descriptive results were reported as either mean ± standard deviation, or median with range. To analyze the hazard ratio for risk factors of adenoma and HCC, a Cox proportional hazards model with stepwise selection was used. Log-rank analysis of Kaplan-Meier survival curves was performed to determine the HCC-free survival rate, and statistical significance was accepted for P values < 0.05.
RESULTS
Patient characteristics
Among the total of 72 patients with a diagnosis of hepatic GSD, 51 patients had GSD type I (50 type Ia and 1 type Ib). Of the total patients, 8 had GSD type III, 1 had GSD type IV, 2 had unknown type, and 10 did not underwent the molecular genetic testing (Fig. 1). A male predominance was observed, with 55 (76.4%) men and 17 (23.6%) women. The mean age at the initial diagnosis was 2.2 years (range, 0.3–13.5 years).
 | Fig. 1Flowchart for GSD patients with specific types. It shows the distribution of specific types of GSD in total patients. Among the total of 72 patients with GSD, 62 patients underwent the molecular genetic testing; 51 showed type I (50 type Ia and 1 type Ib), 8 type III, 1 type IV, and 2 unknown type.GSD = glycogen storage disease.
|
The age at initial symptom presentation was 1.6 ± 2.1 years. The initial symptoms and signs were abdominal distension along with hepatomegaly, which was observed in all patients, followed by abnormal aminotransferase in 80%, diarrhea in 60%, and epistaxis in 38%.
Portacaval shunt operation was done in 20 of 72 patients (27.8%), mainly for short stature, which was persistent despite the administration of cornstarch therapy. The failure of cornstarch therapy was considered when the patient's biochemical markers did not improve for more than one-year despite of optimal diet treatment. The portacaval shunt operation in the patients with GSD in our study was done by the method of end to side. The portacaval shunt operation was mostly done before 1990s since the liver transplantation was established in Seoul National University Hospital in 1990s.
We have looked in for the blood level of uric acid, cholesterol, triglyceride, and transaminases at the time of diagnosis of hepatic adenoma and HCC. In hepatic adenoma patients with GSD, the uric acid level was 8.78 ± 1.75 mg/dL, the cholesterol level was 239.1 ± 83.91 mg/dL, and the triglyceride level was 650.6 ± 442.78 mg/dL. The elevation of transaminases were found in 26 (81.3%) of hepatic adenoma patients with GSD, and the normal range of transaminases in 6 (18.8%). More specifically, the aspartate aminotransferase showed 197.4 ± 211.86 U/L and the alanine aminotransferase 135.2 ± 135.03 U/L in hepatic adenoma patients with GSD, respectively.
In HCC patients with GSD, which were total of four patients, hyperuricemia was found in all of the four patients (100%), and the level was 10.08 ± 2.20 mg/dL; the hypercholesterolemia was found in half of the HCC patients, and the level was 206.0 ± 63.39 mg/dL; the hypertriglyceridemia was found in half of the HCC patients, and the level was 355.0 ± 259.90 mg/dL; the hypertransaminasemia was found in half of the HCC patients, and the level was 161.0 ± 171.08 U/L for aspartate aminotransferase, 77.75 ± 77.40 U/L for alanine aminotransferase, respectively.
Risk factors for adenoma development
Hepatic adenoma developed in 32 patients (44.4%) at a median age of 14.3 years (range, 7.9–26.3 years). The results of the univariate analysis on the risk factors for adenoma development are shown in Table 1. In univariate analysis, GSD type (P = 0.043) and portacaval shunt operation (P = 0.001) were shown to be statistically significant factors in adenoma development.
Table 1
Unadjusted and adjusted HR and CI for risk factors of hepatic adenoma
Data are presented as number (%).
HR = hazard ratio, CI = confidence interval, GSD = glycogen storage disease.
![]()
In multivariate analysis, GSD type and portacaval shunt operation were observed to be statistically significant risk factors in adenoma development (Table 1). When the other types were compared with GSD type I for the hazard ratio of adenoma development, GSD type I showed a significantly higher rate (P = 0.006). When controlling for GSD type, the group with portacaval shunt operation had a 3 fold greater risk for adenoma development than the group without this operation (P = 0.003).
Other factors such as sex difference, cornstarch treatment, metabolic derangement, elevation of liver function parameters, and short stature were not statistically related to the development of adenoma. The results showed no significant relation between adenoma development and diet therapy or metabolic control.
Risk factors and outcomes of HCC
HCC developed in 4 of 32 patients with adenoma (12.5%) at a median age of 26.8 years (range, 13.5–34.1 years). The interval from the diagnosis of adenoma to the diagnosis of HCC was a median of 6.7 years (range, 3–14 years).
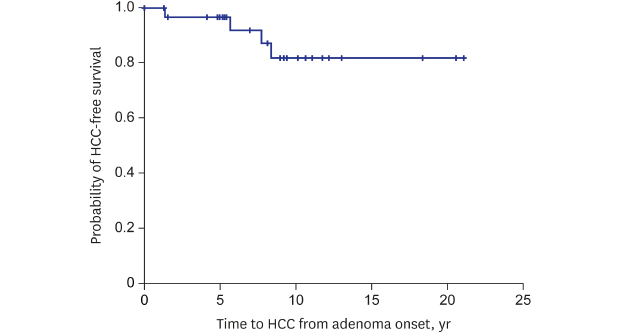
Factors such as sex, cornstarch treatment, GSD type, portacaval shunt operation, metabolic derangement, liver function test abnormality, short stature, and radiologic findings were analyzed. For the metabolic control or derangement, we investigated the level of cholesterol, triglyceride, and uric acid. The results showed that none of the factors had a statistical significance (P > 0.05). We analyzed the HCC-free survival rate at 5 and 10 years from the development of adenoma, and obtained values of 96.6% (range, 77.9%–99.5%) and 82.0% (range, 58.4%–92.9%), respectively (Fig. 2).
 | Fig. 2HCC-free survival at 5 years from the development of adenoma. The vertical axis of the graph shows the probability of HCC-free survival. The horizontal axis indicates time to HCC from adenoma onset.HCC = hepatocellular carcinoma.
|
There were 4 HCC cases in our study during the follow-up period (Table 2), which were diagnosed on the basis of radiologic findings in 1 patient, liver biopsy findings in another patient, and surgical biopsy findings at liver transplantation in the other 2 patients. All 4 cases of HCC were patients with GSD Ia, which accounted for 13.8% (4 of 29) of patients with adenoma in the GSD type I group. HCC developed in 8% of the total patients with GSD type I (4 of 50). Portacaval shunt operation was done in 3 of 4patients with HCC, and each of these patients developed HCC at 14, 9, and 3 years, respectively, after the initial diagnosis of adenoma. One patient who did not undergo shunt operation developed HCC 6 years later. The average time interval between portacaval shunt operation and adenoma is 5.1 years (0.8 to 16.8 years), and the one between portacaval shunt operation and HCC is 15.3 years (3.0 to 23.6 years).
Table 2
Patient characteristics, interval from adenoma to HCC, management, and outcomes of the 4 HCC cases

![]()
Liver transplantation was performed in 2 patients at the age of 13.4 and 30.6 years, respectively. In 1 patient, liver transplantation was performed because of the rapid growth of adenomatous lesions. This patient was found to have HCC based on the pathologic findings of the surgical specimen. He developed multiple metastases despite undergoing chemotherapy after liver transplantation. The other patient who had undergone liver transplantation also showed the increase of adenomas in numbers and sizes in the follow-up imaging of liver MRI. The patient was found to have HCC, which was diagnosed from the surgical biopsy.
Notably, all patients with GSD HCC showed a normal range of aFP levels. aFP elevation was observed in 2 of 32 patients with adenoma, and neither of them had HCC. Specifically, the normal range for aFP was considered to be lower than 20 ng/dL, and the one GSD patient with adenoma showed 78.3 ng/dL, and the other showed 80.5 ng/dL.
One patient with HCC did not receive cornstarch therapy because of poor compliance. The other 3 patients with HCC all received cornstarch therapy at a median age of 4.1 years (range, 1.5–16.7 years). Cornstarch therapy was started in 2 of 3 patients within a short time because the initial diagnosis of GSD because of parent's refusal of receiving dietary treatment at first, and 1 patient started the therapy at 3 years after the diagnosis also because of poor compliance to the medical treatment.
Concerning the change of adenoma on radiologic evaluation, 2 of 4 patients with HCC (50%) showed an increase either in the number or size of adenomas; in the other 2 patients (50%), there was an increase in both size and number. Hemorrhagic change of adenoma was observed in 1 patient with HCC, and no necrotic change was observed in all patients with HCC. As for the radiologic change, of the 32 adenoma patients with GSD, 10 patients showed the increase in size (31.3%), 8 the increase in number (25.0%), 6 the increase of both in size and number (18.8%), 1 hemorrhage within adenoma (3.1%), and 7 showed no change of adenoma (21.9%). In patients with GSD adenoma, multiple adenomas were diagnosed in 20 of 32 patients (62.5%), of whom 3 were found to have HCC. Moreover, 1 patient was found to have only 1 adenoma, the size of which increased on follow-up. Liver biopsy revealed HCC, which reflected the need to perform a biopsy although only 1 adenoma appeared and grew rapidly.
DISCUSSION
HCC is one of the most fatal long-term complications of GSD.12345678 Investigations about the pathophysiology of GSD had helped improve the overall survival rate, however, the morbidity and mortality from malignant transformation of adenoma has not changed yet.1235 As the survival rate is increasing, long-term complications such as hepatic adenoma and HCC are also increasingly observed.12345
According to a European GSD type I study, adenoma developed in up to 75% of adolescent or adult patients, although no malignant transformation was observed.2 Other studies, however, reported that there is a clear risk of malignant transformation in GSD adenoma, even when metabolic derangements are under control.345678 This suggests that the pathophysiology of GSD adenoma and/or its malignant transformation could have an independent pathway from the development of metabolic derangement in GSD.9101112 Di Rocco et al.3 observed that there was no significant difference in metabolic balance between patients with GSD type I who developed adenomas and those who did not, which is consistent with our findings. On the other hand, Weinstein and Wolfsdorf9 showed a significantly higher mean 24-hour blood lactate concentration in the adenoma group than in the non-adenoma group.
GSD I is the most common type, accounting for 90% of all GSD cases, and hepatic adenoma also mostly occurs in GSD type I, with a reported incidence of 22%–57%.2 This is in line with our result that GSD type I is one of the risk factors for hepatic adenoma development. Portacaval shunt operation has been recommended in patients with GSD who are experiencing growth retardation, uncontrolled metabolic derangement, or severe respiratory insufficiency. The operation makes glucose more readily available to peripheral tissues, which relieves hypoglycemia, induces deglycogenation of the liver, and improves other metabolic abnormalities. These metabolic improvements have been suggested to result in a growth spurt in patients with GSD with a short stature. Despite those benefits, however, portacaval shunt operation is reportedly related to hepatic adenoma formation. Although the pathogenesis of hepatic adenoma after portacaval shunt operation remains unclear, it seems to be similar to that of regenerative nodular changes and hepatic tumors caused by hyperarterialization of the liver combined with uneven portal perfusion or outflow disturbance.1314 For those reasons, portacaval shunt operation is no longer performed as often as before.
Although we failed to prove any significant factors for HCC development, one notable observation was that the aFP level was normal in all of our cases during the follow-up. One patient with adenoma showed an elevated level of aFP, and we conducted a liver biopsy, which did not show a malignant change. We are cautiously following up the patient for any change in imaging findings that would suggest malignant transformation of adenoma. In our study, we did not check for protein induced by vitamin K absence or antagonist II (PIVKA-II), although it was reported that elevation of PIVKA-II is observed in patients with GSD with HCC.15
There has been no clear conclusion about the imaging characteristics of patients with GSD adenoma, especially one that could suggest malignant transformation.151617 Nodules could be other lesions such as focal nodular hyperplasia, focal fatty infiltration, focal fatty sparing, hepatoblastoma, or peliosis hepatis, and it is difficult to differentiate these lesions from hepatic adenoma.151617 At present, it is suggested that if there is a rapid increase of either the number or size of adenoma, or both, malignant transformation should be considered.1516 In our study, those radiologic changes did not show statistical significance in relation to malignant transformation of adenoma, which might be caused by the small number of patients with HCC. Besides the increase in the size and number of adenomas, hemorrhagic and necrotic changes of the nodules were observed, and those lesions were finally confirmed as HCC in another study.17 In our study, 1 patient with HCC showed hemorrhagic change of hepatic adenoma, which was finally confirmed as HCC based on biopsy findings. Considering the premalignant nature of hepatic adenoma, biopsy or surgical resection should be considered in patients with GSD who present with hemorrhagic or necrotic hepatic nodules. Furthermore, to differentiate the nature of focal liver lesions, especially whether they are benign or malignant, contrast-enhanced ultrasonography has been recognized as a valuable method in the evaluation of these lesions in patients with GSD, instead of CT or MRI.18
One of the characteristics of GSD adenoma is that hepatic adenoma in GSD usually develops in pubertal age and increases in size and/or number with aging.1516171819 Lee reported that hepatic adenomas in patients with GSD type I are considered to share many of the features of estrogen-induced tumors.16 On the other hand, many researchers have observed that GSD type I hepatic adenoma is clearly different from sex-hormone-induced adenoma in that GSD type I adenoma tends to present as multiple tumors at the initial finding, and is increasingly being detected as a premalignant lesion.21719 In our study, 20 of 32 patients, comprising 62.5% of the total patients with adenoma, developed multiple hepatic nodules at the initial finding. Our study also showed that the most common age of adenoma development was the pubertal age (mean, 14.3 years; range, 7.9–26.3 years). We have not checked for sex hormone levels, especially estrogen, in patients during follow-up. The level of sex hormones might provide a clue about the pathogenesis of GSD adenoma or HCC.
An important characteristic feature of HCC in patients with GSD is that it tends to grow and metastasizerapidly.1219 This can be one of the challenges in deciding the proper timing of surgical intervention (e.g., partial hepatectomy or liver transplantation). For hepatectomy, it was observed that GSD tumors can easily recur after surgicalexcision.1619 Those characteristic of GSD adenoma suggests that orthotopic liver transplantation should be the treatment of choice.1619 There are different point of views about the surgical treatment for hepatic glycogenosis, taking into consideration both benefits and complications.202122 And nowadays, gene therapy for GSD is studied more and more in animal models, and it shows the possibility to figure out the pathophysiology of hepatic adenoma and HCC development in GSD and also the possibility of important role for the treatment of GSD.23
Little is known about HCC occurrence in patients with GSD, and, to our knowledge, there has been no cohort study about the incidence rate of HCC from hepatic adenoma in patients with GSD, except for a few case series. One case series study reported an incidence of HCC from hepatic adenoma of 11% (4 of 36).24 The incidence rate of HCC from hepatic adenoma in our study was 12.5% (4 of 32) in overall patients with adenoma and 13.8% (4 of 29) in patients with adenoma of GSD Ia. All of the cases in our study involved hepatic adenoma-to-carcinoma transformation, not de novo malignancy. The incidence rate of HCC in the total patients with GSD type I in our study was 8.0% (4 of 50), whereas Nakamura et al.25 reported an incidence of 16.0% (3 of 19) in their study of adult patients with GSD Ia.26 To our knowledge, this is the first large cohort study to report about the HCC-free survival rates in patients with GSD with adenoma, which were 96.6% and 82.0% at 5 and 10 years, respectively, from adenoma development.
This long-term follow-up cohort study shows that there is a high incidence of adenoma development in patients with GSD, especially in those with GSD type I. Our study shows that GSD type I and portacaval shunt operation are the risk factors for hepatic adenoma development. The hepatic adenoma in GSD patients have a potential of malignant transformation, which should be keep in mind in follow-up process of the disease.
 XML Download
XML Download