

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
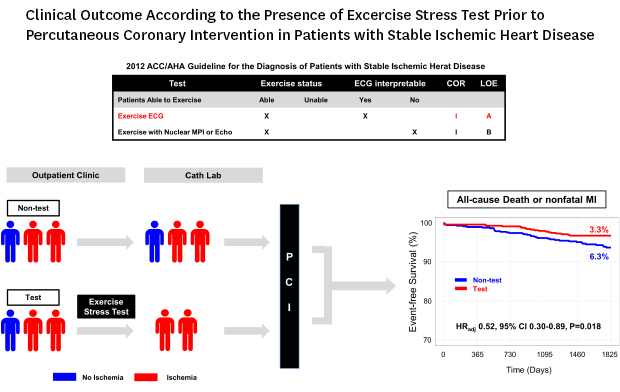
While percutaneous coronary intervention (PCI) has been an important treatment option in stable ischemic heart disease (SIHD), it has failed to reduce death or myocardial infarction (MI) compared with optimal medical therapy (OMT).1 One plausible explanation for this failure is inappropriate patient and lesion selection due to the limitations of PCI performed with angiographic guidance alone. Therefore, current guidelines recommend ischemia-guided PCI with fractional flow reserve (FFR) as well as noninvasive stress tests prior to elective PCI.2 However, noninvasive stress tests are performed in fewer than 50% of all patients prior to revascularization and limited data are available regarding the impact of noninvasive stress tests on long-term clinical outcomes after PCI.3
In one observational study, the pre-PCI stress test was associated with a lower mortality rate in patients undergoing elective PCI.4 However, clinical variables were limited, and angiographic and procedural data were not recorded in that study. Moreover, the results or types of the stress test were not clearly presented. It has also been reported that ischemia-guided revascularization with myocardial perfusion imaging decreased the risk of repeat revascularization for patients with multivessel disease in a single center observational study.5 However, current guidelines recommend exercise stress test (EST), which is the most physiologic and the most commonly performed noninvasive stress test, as the initial assessment. Despite this recommendation, the impact of antecedent ESTs on the long-term clinical outcomes after elective PCI has not been investigated. Therefore, we sought to investigate long-term outcomes in patients undergoing elective PCI for SIHD with or without EST.
METHODS
Study population
Between January 2003 and June 2011, a total of 5,929 consecutive patients underwent PCI with drug-eluting stent (DES) implantation for coronary artery disease at Samsung Medical Center. To select patients with SIHD undergoing elective PCI, we excluded 2,431 patients who had a diagnosis of acute coronary syndrome (unstable angina, non-ST-segment elevation or ST-segment elevation MI), and 279 patients who had undergone diagnostic work-up at other hospitals and were referred to our center for PCI. Among patients with SIHD, we also excluded 243 patients who had undergone pharmacologic stress tests, and 291 patients who had undergone ESTs without a positive result. In addition, we excluded 11 patients due to lack of follow-up information. Finally, we included 2,674 patients in the present analysis. Patients were classified into the 2 groups: those who underwent elective PCI with positive ESTs within 180 days prior to PCI (the test group), and those who did not undergo any noninvasive stress tests within 180 days prior to PCI (the non-test group) (Fig. 1).
 | Fig. 1Study population.DES = drug-eluting stent, PCI = percutaneous coronary intervention, EST = exercise stress test.
|
Clinical, angiographic and procedural data were recorded prospectively in our PCI registry by independent research personnel. Patients were routinely followed up at 1, 6, and 12 months after the index procedure and annually thereafter. Further information was collected by telephone contact and medical records if necessary. Follow-up was considered complete if the patient's death was confirmed by the National Population Registry of the Korea National Statistical Office using a unique personal identification number or if the patient was contacted at the planned follow-up interval.
PCI and angiographic analysis
PCI was performed according to the practice guidelines established by the Korean Society of Interventional Cardiology.6 All patients were given a loading dose of aspirin (300 mg) and clopidogrel (300 mg) before the coronary intervention unless they had previously been receiving these antiplatelet medications. Unfractionated heparin was administered to maintain an activated clotting time of 250 to 300 seconds during PCI. The choice of treatment strategy, access, stenting technique, type of DES, and use of adjunctive devices to facilitate optimal stenting was at the operator's discretion. The duration of dual antiplatelet therapy with aspirin and clopidogrel was determined by the attending physicians.
Pre- and postprocedural coronary angiograms were analyzed. The major epicardial coronary arteries were defined as diseased vessels if it exhibited ≥ 50% stenosis, and left main coronary artery stenosis was regarded as two-vessel disease. All cine coronary angiograms were reviewed and analyzed at the angiographic core laboratory (Heart Vascular Stroke Institute, Samsung Medical Center, Seoul, Korea). The Synergy Between PCI With Taxus and Cardiac Surgery (SYNTAX) score.7 and the residual SYNTAX score8 were calculated by independent experienced personnel.
EST
The primary noninvasive stress test for patients with coronary artery disease is EST in our institution. As current guidelines recommend, EST was generally indicated in patients with an intermediate pretest probability of ischemic heart disease, or in patients with a high pretest probability for risk stratification.29 EST was contraindicated in patients who had an uninterpretable electrocardiogram such as left bundle branch block or ventricular pacing rhythm, or those unable to exercise. For the purpose of risk stratification, however, poor functional status per se was not a contraindication of exercise stress testing.
The exercise treadmill test was performed according to the Bruce protocol.10 In brief, a 12-lead electrocardiogram was recorded and monitored continuously with a computerized system (Quinton Q-Stress) during exercise and rest. The electrocardiogram was then reviewed by cardiology fellows and senior cardiologists. The test was discontinued in the event of limiting symptoms including dyspnea, chest pain, fatigue, or significant abnormalities in rhythm or blood pressure. The target heart rate was determined as 85% of maximum predicted heart rate (220 minus age), but was not used as a predetermined end point for premature termination of the test. The positive result was defined as horizontal or downsloping ST depression ≥ 1 mm (0.1 mV) at 60 to 80 ms after the J point. The metabolic equivalents (METs) was estimated by the stage of the Bruce protocol according to the standard.11 The Duke treadmill score was calculated as follows:
Duration of exercise in minutes − (5 × the maximal ST-segment deviation from baseline during or after exercise in millimeters) − (4 × angina index).
The angina index was defined as 0 if the patient had no angina during exercise, 1 if the patient had non-limiting angina, and 2 if angina was the reason the patient stopped exercising.1213 For interpretation of EST, inter-observer agreement (Kappa = 0.84; 95% confidence interval [CI], 0.78–0.89) and intra-observer agreement (Kappa = 0.97; 95% CI, 0.95–0.98) were good.14
Outcomes
The primary outcome was a composite of all-cause death or nonfatal MI at 5 years from the index PCI. The secondary outcomes included all-cause death, cardiac death, nonfatal MI, any repeat revascularization, target vessel revascularization, and target lesion revascularization at 5 years from the index PCI.
All deaths without an undisputed non-cardiac cause were considered cardiac death. MI was defined as elevated cardiac enzyme levels, such as troponin I or myocardial band fraction of creatine kinase, greater than the upper limit of the normal range with either ischemic symptoms or electrocardiography changes indicating ischemia, which required subsequent hospitalization (defined as an emergency admission with a principal diagnosis of MI). Any repeat coronary revascularization included all target and non-target revascularizations with either PCI or coronary artery bypass graft surgery.
Statistical analysis
Continuous variables were presented as mean ± standard deviation and analyzed using Student's t-test or the Mann-Whitney U test as appropriate. Categorical variables were analyzed using the χ2 test. Event rates were calculated based on Kaplan-Meier censoring estimates. Clinical outcomes were compared between the test and non-test groups using multivariable Cox regression analysis with clinically relevant variables including age, gender, diabetes mellitus, extent of coronary artery disease, and types of stents used. Exploratory subgroup analysis using univariable Cox regression analysis was performed to estimate the effects of interaction terms between groups and test effects on clinical outcomes. In the subgroup analysis, each subgroup divided by exercise capacity or Duke treadmill score in the test group was compared with the entire non-test group because of unknown information on exercise capacity or Duke treadmill score in the non-test group.
To minimize selection bias and control potential confounding variables, an adjusted analysis was performed with propensity score matching.15 The propensity score was the probability that any patient would be selected for the test group and was estimated by multivariable logistic regression analysis using all baseline variables except procedural profiles (number of stents, stent diameter, total stent length, and pre- and post-diameter stenosis). For the propensity-score matching, a 1:1 matching process without replacements was performed by a greedy algorithm with nearest neighbor matching, yielding 668 patients in the test group matched with 668 controls in the non-test group. Variables were considered balanced between the test and non-test groups after propensity score matching if the absolute value of the standardized mean difference of each variable was less than ± 10%. As a sensitivity analysis to clarify the benefit of documenting positive EST prior to elective PCI, clinical outcomes were additionally compared among the groups including patients who underwent EST but had a negative result.
All probability values were two-sided and P values < 0.05 were considered statistically significant. R software version 3.4.0 (R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analyses.
RESULTS
Patients characteristics
Of 2,674 patients eligible for the present analysis, 668 patients (25.0%) underwent ESTs within 180 days prior to elective PCI, and 2,006 patients (75.0%) did not undergo any noninvasive stress tests (Fig. 1). Baseline characteristics are shown in Table 1. Patients in the test group were younger, had a higher prevalence of men, and had a lower risk profile with less comorbidities than those in the non-test group. Table 2 shows the procedural profiles. After propensity score matching (668 pairs) (Supplementary Fig. 1), all baseline characteristics were well-balanced between the 2 groups. In the matched population, angiographic and procedural profiles which included stent profiles (number and total length of stents) and residual disease (residual SYNTAX score and mean post-diameter stenosis) were similar between the 2 groups.
Table 1
Baseline characteristics according to the presence of EST prior to PCI
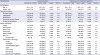
Values are mean ± standard deviation or number (%).
EST = exercise stress test, PCI = percutaneous coronary intervention, SMD = standardized mean difference, CVA = cerebrovascular accident, MI = myocardial infarction, CABG = coronary artery bypass surgery, LVEF = left ventricular ejection fraction, LV = left ventricle, ACEi = angiotensin-converting enzyme inhibitor, ARB = angiotensin II receptor blocker, DS = diameter stenosis.
aPropensity score matching was performed using entire variables except stent profiles (number, diameter, and total length of stent) and residual disease (pre- and post-DS); bLV dysfunction was defined as LVEF less than 30%. LVEF was measured in 2,321 of 2,674 patients (86.8%).
![]()
Table 2
Procedural profiles according to the presence of EST prior to PCI
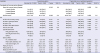
Values are mean ± standard deviation or number (%).
EST = exercise stress test, PCI = percutaneous coronary intervention, SMD = standardized mean difference, SYNTAX = Synergy Between PCI With Taxus and Cardiac Surgery, CTO = chronic total occlusion, IVUS = intravascular ultrasound, OCT = optical coherence tomography, DS = diameter stenosis.
aPropensity score matching was performed using entire variables except stent profiles (number, diameter, and total length of stent) and residual disease (pre- and post-DS); bSYNTAX score was measured in 2,245 of 2,674 patients (84.0%). Complete revascularization was defined as residual SYNTAX score = 0; cType of stent used included 1st generation (paclitaxel-eluting stent, sirolimus-eluting stent), 2nd generation (everolimus-eluting stent, zotarolimus-eluting stent, biolimus-eluting stent) and otherwise (simultaneous usage of 1st generation stent, 2nd generation stent or bare-metal stent).
![]()
The detailed results of EST in the test group were presented in Supplementary Table 1. Baseline mean exercise duration was 8.1 ± 2.2 minutes. Mean Duke treadmill score was −4.3 ± 5.0, which represented patients in the test group as a moderate-risk population.
Clinical outcomes for overall population
The median follow-up duration was 5.9 years (interquartile range, 3.8 to 7.9). The test group had a significantly lower incidence of all-cause death or nonfatal MI than the non-test group (3.3% vs. 10.9%; adjusted hazard ratio [HR], 0.34; 95% CI, 0.22–0.55; P < 0.001) (Fig. 2 and Table 3). The incidence of cardiac death or nonfatal MI was also significantly lower in the test group than in the non-test group (2.3% vs. 7.3%; adjusted HR, 0.36; 95% CI, 0.21–0.64; P < 0.001). However, the incidence of any revascularization was similar between the 2 groups (16.7% vs. 16.8%; adjusted HR, 0.99; 95% CI, 0.79–1.25; P = 0.962).
 | Fig. 2Clinical outcomes at 5 years according to the presence of EST prior to PCI in overall population of patients with SIHD. (A) All-cause death or nonfatal MI, (B) all-cause death, (C) nonfatal MI, (D) cardiac death or nonfatal MI, (E) cardiac death, and (F) any revascularization.Adjusted HR and its CI was calculated by multivariable Cox regression analysis using clinically relevant variables including age, gender, diabetes mellitus, extent of coronary artery disease, and types of stent used.
EST = exercise stress test, PCI = percutaneous coronary intervention, SIHD = stable ischemic heart disease, MI = myocardial infarction, HR = hazard ratio, CI = confidence interval.
|
Table 3
Clinical outcomes at 5 years according to the presence of EST prior to PCI
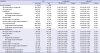
Values are presented as number (%) or HR (95% CI). The cumulative incidences of clinical outcome were presented as Kaplan-Meier estimates at 5 years. HR and its 95% CI was calculated by Cox regression analysis.
EST = exercise stress test, PCI = percutaneous coronary intervention, HR = hazard ratio, CI = confidence interval, MI = myocardial infarction, DS = diameter stenosis.
aPropensity score matching was performed using entire variables except stent profiles (number, diameter, and total length of stent) and residual disease (pre- and post-DS); bAdjusted HR was calculated by multivariable Cox regression analysis using clinically relevant variables including age, gender, diabetes mellitus, extent of coronary artery disease, and type of stent used.
![]()
Clinical outcomes for matched population
The test group had a significantly lower incidence of all-cause death or nonfatal MI than the non-test group over 5 years after PCI (3.3% vs. 6.3%; adjusted HR, 0.52; 95% CI, 0.30–0.89; P = 0.018), even after propensity score matching (Fig. 3 and Table 3). The incidence of cardiac death or nonfatal MI was also significantly lower in the test group than in the non-test group (2.3% vs. 4.8%; adjusted HR, 0.48; 95% CI, 0.25–0.92; P = 0.026). The incidence of any revascularization was not significantly different between the 2 groups (16.7% vs. 18.3%; adjusted HR, 0.91; 95% CI, 0.70–1.19; P = 0.509).
 | Fig. 3Clinical outcomes at 5 years according to the presence of EST prior to PCI in matched population of patients with SIHD. (A) All-cause death or nonfatal MI, (B) all-cause death, (C) nonfatal MI, (D) cardiac death or nonfatal MI, (E) cardiac death, and (F) any revascularization.Adjusted HR and its CI was calculated by multivariable Cox regression analysis using clinically relevant variables including age, gender, diabetes mellitus, extent of coronary artery disease, and types of stent used.
EST = exercise stress test, PCI = percutaneous coronary intervention, SIHD = stable ischemic heart disease, MI = myocardial infarction, HR = hazard ratio, CI = confidence interval.
|
Exploratory subgroup analysis
To confirm the association between the pre-PCI ESTs and improved clinical outcomes of all-cause death or nonfatal MI, a subgroup analysis was performed. The lower incidence of all-cause death or nonfatal MI in the test group was observed consistently across the various subgroups without significant interaction P values (Fig. 4), and among patients with left ventricular ejection fraction ≥ 50% (Supplementary Tables 2 and 3, and Supplementary Fig. 2).
 | Fig. 4All-cause death or nonfatal MI at 5 years according to the presence of EST prior to PCI in various subgroups.HR and its CI was calculated by univariable Cox regression analysis in the propensity score-matched population.
MI = myocardial infarction, EST = exercise stress test, PCI = percutaneous coronary intervention, METs = metabolic equivalents, NA = not available, HR = hazard ratio, CI = confidence interval.
aBecause of unknown exercise capacity or Duke treadmill score in the non-test group, each subgroup of the test group was compared with the entire non-test group.
|
In the sensitivity analysis, the test group also had a significantly lower risk of all-cause death or nonfatal MI than the patients with a negative result of EST prior to PCI (Supplementary Tables 4 and 5, and Supplementary Fig. 3).
DISCUSSION
Although PCI relieves angina and reduces the extent of myocardial ischemia, there has been no confirming evidence for PCI to reduce death or MI compared with OMT alone in SIHD.1 A lack in benefit regarding long-term clinical outcomes of PCI in SIHD may result from periprocedural complications and stent failure during follow-up, but inappropriate lesion and patient selection is considered to be one of the most important causes. In particular, treatment decision based on stenosis measured by coronary angiography alone can be misleading, because coronary angiography is associated with overestimation or underestimation of coronary lesions as well as significant interobserver variability.161718 To overcome these drawbacks, efforts have been made to identify lesions causing significant ischemia. PCI guided by FFR, which determines functionally significant coronary lesions, showed improved clinical outcomes compared to angiography-guided PCI and OMT.1920 However, this assessment is invasive, and its global adoption rate is still low in real world practice.21 Alternatively, noninvasive stress testing is an appropriate tool for detecting myocardial ischemia and has several strengths in managing coronary artery disease. For instance, it can predict downstream noninvasive imaging and invasive angiography results.22 and detect high-risk patients who require revascularization as well as provide prognostic information.23 Moreover, stress testing followed by selective angiography is more cost effective than direct catheterization.24 Despite these advantages of noninvasive stress testing, the majority of patients undergo elective PCI without stress tests,3 and a previous study reported that elective PCI without antecedent stress testing was associated with high mortality.4 However, this study was limited because patient characteristics differed greatly according to the presence of stress testing, and angiographic data were not collected. Moreover, the results or types of the stress test performed were not clearly described. Another observational study showed that PCI guided by myocardial perfusion imaging was associated with a decreased risk of major adverse cardiac and cerebrovascular events in patients with multivessel disease.5 However, the most commonly used stress test for ischemic heart disease is EST.2526 which assesses myocardial ischemia by giving a personalized physiologic load, and current guidelines recommend ESTs as a Class I indication in patient with SIHD.2 Nevertheless, the impact of ESTs on the outcomes of elective PCI has not been investigated yet. Therefore, we compared the clinical outcomes of PCI for patients who underwent pre-PCI ESTs with those who did not undergo any noninvasive stress tests.
We found that PCI with a positive antecedent EST was associated with a reduced risk of all-cause death or nonfatal MI. Patients undergoing PCI based on the EST would also have functionally significant coronary lesions and therefore receive more benefit from revascularization than those without a prior stress test. Even if the EST does not have excellent accuracy, patients with high risk requiring revascularization could be detected by the EST. Compared to OMT, revascularization has been shown to confer the survival benefit in patients with substantial myocardial ischemia,27 however, worse outcome in patients without myocardial ischemia,28 findings that are accordant with our results. During the study period, FFR was used rarely due to the lack of supporting data from large randomized trials and reimbursement issues in the Korean medical insurance system. Therefore, among patients without stress tests, PCI might have been unnecessarily performed in those with functionally insignificant lesions. In this population, procedure-related or stent-related complication potentially outweighed the benefit from revascularization, as shown that the patients without stress tests had an increased risk of target vessel MI but similar risk of non-target vessel MI, compared with those with stress tests. Taken together, these data indicate that selection of patients for elective PCI by ESTs may improve long-term clinical outcomes after revascularization. Although EST is not a treatment option and may not directly improve clinical outcomes, it is a proper diagnostic tool for detecting exercise-induced myocardial ischemia and therefore can aid appropriate patient selection for PCI by providing useful information about exercise capacity, hemodynamic response, symptoms, or electrocardiogram changes to individual physical loads. In the subgroup analysis, improved outcomes of PCI with pre-PCI ESTs were consistently observed in the various subgroups. There were no significant interactions between the EST and the extent of coronary artery disease, or between the EST and the stent generation.
Contrary to our expectations, any revascularization occurred at similar rates in patients who underwent ESTs prior to PCI and patients who did not. This finding could be related to the similar extents of residual coronary artery disease measured by the residual SYNTAX score, a known predictor of repeat revascularization.8 The risk of target vessel or target lesion revascularization was also similar between patients with and without exercise stress testing prior to PCI. Nevertheless, the similar risk of any revascularization did not necessarily mean the similar outcome related with PCI. Because the rates of restenosis and repeat revascularization have been lowered after the introduction of drug-eluting stent, unnecessary PCI could alter the risk of death or MI without change in the risk of target vessel or target lesion revascularization, as the 2-year outcome of Fractional Flow Reserve Versus Angiography for Multivessel Evaluation (FAME) trial.29
The current study has several limitations. First, it has the inherent limitations of a non-randomized study. Although the baseline variables were well-balanced between the test and non-test groups after adjustment using propensity score matching, unmeasured confounders should be considered. In addition, although there was a general indication of EST in our institution, the reason why EST had not been performed in the non-test group was not clearly identified. However, less than half of patients with SIHD undergo PCI with prior stress testing in real world practice.3 Future well-designed randomized studies are needed. In particular, ISCHEMIA trial (NCT01471522) is expected to provide evidence to inform ischemia-based PCI at the patient level. Second, adverse clinical events were not independently adjudicated in our registries. Considering the limitation of possible inaccuracy in determining cause of death, we chose all-cause mortality as the primary outcome instead of cardiac mortality. Third, there has been no recommended time interval between exercise stress testing and PCI. Although a previous study used 90 days to define antecedent stress testing,4 recommended outpatient follow-up interval by guideline is 4 to 6 months,2 and the rate of stress testing prior PCI at 180 days was not significantly different compared with that at 90 days in previous study.3 In our study, there was also similar rate of stress testing between 180 days (n = 668) and 90 days (n = 645) prior to PCI. Fourth, the practice pattern of PCI changed during the long enrollment period. DES safety has improved markedly and the use of physiologic assessment during coronary angiography or PCI gradually increased, which may hinder the full application of our results to current practice. Lastly, we did not collect detailed information on medical treatment during follow-up. However, we consider it unlikely that there were significant differences in medical treatment during follow-up between the test and non-test groups, considering that the groups were well-matched in clinical, angiographic, and procedural characteristics after propensity score matching.
In conclusion, patients who underwent elective PCI with antecedent ESTs had a reduced risk of all-cause death or nonfatal MI than those undergoing PCI without any noninvasive stress tests.
 XML Download
XML Download