

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
There are approximately seven million elderly people age 65 or older in Korea. The number of dementia patients is estimated at 705,473 (10%), which is expected to rise to more than one million by 2025. In particular, the number of elderly people with mild cognitive impairment (MCI), which can be transferred to dementia, is rapidly increasing. In 2018, 22.5% of elderly people age 65 or older are estimated to have MCI.1 In advanced studies, 10%–12% of the MCI reported migrating to dementia within a year.2 Thus, it can be observed that the cognitive improvement of the MCI is critical in preventing dementia. However, there are some pharmacological therapies associated with cognitive impairment, but it is difficult to expect fundamental treatment with this. Thus, it is effective to combine non-pharmacological therapies with pharmacological therapies.3
Recently, a variety of non-pharmacotherapies has been proposed. Among them, non-pharmacotherapy comprising physical activity, cognitive training, and social interaction activities.4 These interventions strengthen the cognitive reserve of the elderly with dementia and MCI. Cognitive reserve is a driving force in maintaining cognitive function against neurological brain injury such as dementia as well as atrophy of the brain due to aging, which also means the potential to strengthen the existing neural pathways of the brain and enlarge the new neural pathways.5 Especially, physical activity including exercise, is facilitates the strengthening of cognitive reserve.6 Various previous studies have shown muscle and aerobic exercise can delay cognitive decline such as memory and concentration in dementia patients.7 The meta-analysis of physical activity program for dementia patients also showed significant improvement in cognitive function.8 Physical activity has a positive impact on cognitive function. However, in a recent meta-analysis of the MCI population, 92% of the elderly with MCI who engaged in single exercise reported that the impact was unclear.9 Conversely, multi-tasking exercise rather than single exercise is effective in increasing brain function10 and because the dual task or multiple task exercise method with exercise and cognitive task rather than just one exercise method is more effective in improving cognitive function, It can be predicted that it also impacts the brain's cognitive reserve. However, there is a lack of research on cognitive function improvement of programs that combine exercise and cognitive tasks of the MCI subject. The purpose of this study was to investigate the impact of multi-tasking exercise on the cognitive and motor functions of the Cognitive Normal Elderly (CNE) and MCI.
METHODS
Study design and participants
In this study, 144 MCI and CNE registered in 16 regional dementia centers in Busan metropolitan city were recruited. Among them, a total of 67 subjects participated, except for 77 subjects, diagnosed with dementia or who refused to participate in the study. Each regional dementia center used promotional posters, homepage advertisements, and local newspapers for recruitment of participants. The contents of the advertisement described the multi-tasking exercise and guided local residents to visit the regional dementia center. MCI subjects in this study were diagnosed by neurologists and psychiatrists based on the results of Mini-Mental State Examination-Dementia Screening (MMSE-DS), Seoul Neuropsychological Screening Battery (SNSB), and Korean Version of the Consortium to Establish a Registry for Alzheimer Disease (CERAD-K). The diagnosis of MCI was made according to Petersen's criteria.11 The subjects of the CNE were assigned to the study according to the value of normative of MMSE-DS.12 The final selected 67 subjects (MCI group=33, CNE group=32) participated in the intervention program for approximately six months (May-October), 2018 at 14 regional dementia centers in Busan metropolitan city. Each institution conducted an intervention program of a total of eight sessions (eight weeks) once weekly for six months. The start of the program was different for each institution, but the total sessions and operating periods were identical. Additionally, pre-assessments were performed within one week before the start of the program, and post-assessments were performed within one week after the end of the program. During the intervention, two subjects withdrew from participation with musculoskeletal disorders, and a total of 65 subjects were tested for cognitive and motor functions (Fig. 1).

Multi-tasking exercise intervention
The intervention program consisted of eight sessions 60–80 minutes per session and subjects participated in this study for a total of eight weeks once weekly. Before the start of the main exercise, the preparation exercise was conducted for approximately 20 minutes. It was designed to perform stretching and strength training at home. This main exercise consisted of stretching, muscle strengthening, balance exercise, aerobic exercise, double task, and multi-tasking exercise for 60 minutes. The multi-tasking exercise was designed to exercise as well as improve attention, performance, and memory by introducing the dual task. It has the characteristic to conduct tasks such as conversation, thinking, and calculation simultaneously while exercising. The program was operated directly by practitioners (occupational therapist, registered nurse, social worker) who completed training on multi-tasking exercise at the Busan Metropolitan Dementia Center. Before starting the exercise, the condition of the subject was checked and all the subjects checked and signed the agreement of the emergency situations response guide of the dementia center. The manual for the multi-tasking exercise is shown in Table 1.
Table 1
Manual of the multi-tasking exercise

The program takes 80 minutes per session and consist of eight sessions in total. Each session includes “Preparatory and finishing exercise” that takes 20 minutes, and “Main exercise” consisting of one exercise or multi-tasking exercise, which takes 60 minutes.
![]()
Neuropsychological and motor function assessment
Three assessment tools were used to analyze the subjects' cognitive ability and depression. And MMSE-DS was used to measure overall cognitive change. The Short-Form Geriatric Depression Scale (SGDS-K) was used to assess the change of depressive mood status.13-15 Also, the Subject Memory Complain Questionnaire (SMCQ) was used to assess subjective memory decline.16 The subjects' motor ability status and changes were measured by 5-chair sit to stand and 5-meter walking speed. The “5-chair sit to stand” is a tool used for evaluating leg strength and coordination, which measures the time spent by the subject sitting and standing in a chair five times. The “5-meter walking speed” measures the time that passes a 5 m walking section by setting acceleration and deceleration sections of 1.5 m at the starting and ending points of a total of 8 m of walking length. The measurements were performed for four times in total, and the normal walking speed was measured three times and the average speed was measured accordingly and measured once the maximum walking speed without running.
Statistical analyses
The data collected in this study were analyzed using SPSS version 21 (IBM Corp., Armonk, NY, USA). The descriptive statistics were used to analyze the general characteristics of the subjects and the paired t-test was used to analyze pre-post intervention changes in cognitive and motor function. The p-values less than 0.05 were statistically significant.
RESULTS
Characteristics of participants
A total of 65 subjects (MCI group=33, CNE group=32) were assigned to this study. The mean age of subjects in MCI group was age 73.88±7.46, 12 males and 21 females. The CNE group was age 76.50±5.60, 8 males and 24 females. The education level was 8.03±3.46 for the MCI group and 7.69±4.83 for the CNE group. The MCI group showed a higher education level than the CNE group. Additionally, subjects diagnosed with hypertension were identified as the MCI group 9 (27.3%) and the CNE group 5 (15.6%), and in the question of if they are currently smoking, 5 (15.2%) in the MCI group and 7 in the CNE group (21.9%) of the subjects responded yes. The respondents who answered ‘yes’ to the question if they are currently drinking alcohol were 6 (18.2%) in the MCI group and 9 (28.2%) in the CNE group (Table 2).
Table 2
Characteristics of participants (n=65)

Data are shown as mean±standard deviation or number (%).
MCI: mild cognitive impairment, CNE: cognitive normal elderly, SD: standard deviation.
![]()
Comparison of the Pre-Post in the MCI Group
The results of MCI group showed statistically significant improvement in cognitive and motor function evaluation items (p<0.05). The MMSE-DS (score) improved by 2.24 (p=0.006) from 21.12±4.30 before intervention to 23.36±3.32 after intervention and the SMCQ (score) improved by 1.33 (p=0.000) from 6.60±3.62 before intervention to 5.27±3.19 after intervention. The SGDS-K (score) improved by 1.3 (p=0.000) from 4.93±3.62 to 3.63±2.76. The “5-chair sit to stand (sec)” was shortened by 1.72 (p=0.000) from 13.55±4.26 before intervention to 11.83±3.89 after intervention and the normal speed of the “5-meter walking speed (sec)” was shortened by 0.47 (p=0.004) from 6.39±3.31 before intervention to 5.92±3.33 after intervention and the maximal speed was shortened by 0.41 (p=0.002) from 5.38±3.40 before intervention to 4.97±3.41 after intervention (Table 3).
Table 3
Comparison of the pre-post in the MCI group (n=33)
MCI: mild cognitive impairment, SD: standard deviation, MMSE-DS: Mini-Mental State Examination-Dementia Screening, SMCQ: Subject Memory Complain Questionnaire, SGDS-K: Short-Form Geriatric Depression Scale-Korean version.
*p<0.05; †p<0.005.
![]()
Comparison of the pre-post in the CNE group
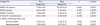
The results of the cognitive and motor function evaluation of the CNE subjects showed statistically significant improvement in all items except MMSE-DS and SGDS-K (p<0.05). The SMCQ (score) improved by 1.5 (p=0.002) from 7.12±3.44 before intervention to 5.62±3.01 after intervention and the “5-chair sit to stand (sec)” was shortened by 2.46 (p=0.002) from 14.59±5.65 before intervention to 12.13±3.89 after intervention and the normal speed of the “5-meter walking speed (sec)” was shortened by 0.24 (p=0.013) from 5.61±2.54 before intervention to 5.37±2.46 after intervention and the maximal speed was shortened by 0.26 (p=0.007) from 4.91±2.66 before intervention to 4.65±2.40 after intervention (Table 4).
Table 4
Comparison of the pre-post in the CNE group (n=32)

CNE: cognitive normal elderly, SD: standard deviation, MMSE-DS: Mini-Mental State Examination-Dementia Screening, SMCQ: Subject Memory Complain Questionnaire, SGDS-K: Short-Form Geriatric Depression Scale-Korean version.
*p<0.005; †p<0.05.
![]()
DISCUSSION
In this study, multi-tasking exercise was provided to the MCI and CNE groups to analyze their impact. As a result, statistically significant improvement on cognitive functions with psychological symptom was observed in both groups for pre-post intervention comparison. In the case of the MCI group, the MMSE-DS score improved by 2.2 points compared to before the intervention and the CNE group improved by 0.7 points, and the score of the SMCQ decreased by 1.3 points in the MCI group and 1.5 points in the CNE group, and the degree of subjective memory decline improved. The SGDS-K score decreased by 1.3 points in the MCI group and by 0.6 points in the CNE group, and it was confirmed that the degree of depression improved. Especially in this study, we examined the change in improving cognitive function as well as motor function. In the case of the 5-chair sit to stand, compared with that before intervention, 1.7 seconds in the MCI group, CNE group it was shortened to 2.5 seconds. In the 5-meter walking speed, the normal speed of the MCI group was shortened by 0.5 seconds, the maximum speed was shortened by 0.4 seconds, the normal speed of the CNE group was shortened by 0.2 seconds, and the maximum speed was shortened by 0.3 seconds. These results suggest that multi-tasking exercise can have a positive impact on the MCI and CNE groups. In this study, we applied the program to the MCI group and CNE group respectively, and compared if it is more effective in improvement cognition in which group, and selected a group suitable for the program. However, this study did not measure cognitive and motor function changes between groups, since the ceiling effects of the CNE groups are not considered, there is a limit to comparing the differences in the impact between the two groups. Since the baseline cognitive function was lower in the MCI group compared to the CNE group, the change in cognitive function may be better represented in the MCI group. The MCI group is characterized by marked memory impairment, and characterized in that general cognitive impairments such as language ability, frontal lobe function, and visual-spatial ability are displayed, but the activities of daily living is maintained to some extent.17 In particular, more than 40% of MCI patients are reported to recover to normal status18 and this can be viewed as critical to intervention before progressing to dementia.
As a result of analyzing advanced research, it is obvious that physical activity positively impacts cognitive function,19 but when exercise or cognitive therapy is applied in a task, the impact is insufficient.20 In this program, the subject has to make a more extensive mental effort by solving the problems of aerobic exercise, stretching, strength training, and cognitive activities. In particular, when performing multiple tasks, it has been reported that the blood flow in the brain rises,21 activates a wide area of the brain, and positively impacts cognitive functions22 and in the future, there may be many changes in applying the intervention model of the MCI patients. Additionally, the MCI group are accompanied by behavioral and emotional symptoms with cognitive decline, and in particular, the proportion of suffering from depression is seen most frequently in 20.1%–44.3%,23 and various advanced studies It has been reported that depression causes damage to overall cognitive function. This can be viewed as an alleviation of depressive symptoms in MCI patients that impacts cognitive function improvement. In this study, it was confirmed that the MCI group significantly alleviated depressive symptoms after intervention compared to before intervention (p<0.005). This demonstrates that multi-tasking exercise can facilitate in alleviating general cognitive and mental symptoms observed in MCI patients. In considering the impact of this study, it is considered to be an effective program for improving MCI cognitive functions, alleviating depression, and improving physical activity.
Our study has shortcomings. We did not include the control group who did not conduct the intervention and the number of subjects was relatively small, the arbitration period was short, and it was difficult to fully observe the impact. Also, the usual exercise and living habits of each individual would have impacted the result, and the neurocognitive tests and brain imaging were not performed, so we could not confirm the impact of specific cognitive area and neurological brain changes in detail. It is necessary to recruit homogeneous groups in the future and to conduct research on a large number of patients. Additionally, there is a need for clinical intervention research that can cognitively improve through multicenters, randomized controlled trial research, and necessitate further studies on the impact of preventing dementia.
 XML Download
XML Download