

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A durable vascular access is an integral component of hemodialysis treatment for end-stage renal disease (ESRD). Currently, the type of vascular access that has the longest duration of function is the native arteriovenous fistula (AVF) [123]. Nevertheless, failure of AVF may occur at any time after its creation [45]. Although several authors have claimed that AVF has a lower failure rate once matured [6], the reported rate of AVF loss in the first year after maturation remained high at 29% [7]. Hence, it is important to closely monitor the AVF during the first year of use. Earlier studies have suggested several prognostic factors associated with 1-year AVF survival, such as prior central venous catheter (CVC) use, interventions used to promote AVF maturation, peripheral vascular disease, and female sex [8910111213]. However, the results of these studies were inconsistent.
Given the growing global incidence of ESRD, the demand for AVF creation is also increasing. Data on prognostic factors predicting the success rate and survival of AVFs are crucial for patients, physicians, hospital administrators and policy makers to estimate personal and national budgets and manpower.
To date, few studies have incorporated the clinical features of patients into a prediction model for AVF nonmaturation or AVF failure after creation [1415161718]. Additionally, no study has developed a scoring system to predict the survival of AVF after maturation. This study aimed to develop a simple score based on clinical data for predicting AVF survival at 1 year after initial use in a group of ESRD patients who underwent AVF creation for the first time. The score was also tested in another group of patients to validate its clinical application.
METHODS
Study design and patient selection
This retrospective study was performed using data from the electronic records of patients with ESRD who underwent first-time autogenous AVF creation at the author's institution during the period from January 2009 to December 2017 and who had successful cannulation. The AVF created included radiocephalic and brachiocephalic types. Each patient was required to have had a minimum follow-up period of 12 months after the first cannulation. The study was approved by the Institutional Review Board (approval number 023/2562) and was conducted in accordance with the Declaration of Helsinki.
Fistula creation and follow-up assessment
In the author's institution, first-time AVF was performed by one of the vascular surgeons. As a routine practice in the vascular unit, the patients had to have a vascular anatomy suitable for AVF formation. This was assessed preoperatively by physical examination. Anatomical suitability for AVF placement were as follows: (1) easily palpable pulse; (2) no pressure gradient between arms; (3) adequate diameter (≥2 mm) and length (at least 5 cm) of superficial vein with easy compressibility; (4) absence of venous collateral circulation in the shoulder region; and (5) absence of edema. Duplex ultrasound assessment was selectively performed before AVF formation at the discretion of the surgeon [6].
The AVF could be an anastomosis between the end of the cephalic vein to the side of radial (radiocephalic anastomosis) or brachial (brachiocephalic anastomosis) arteries based on the surgeon's discretion and the feasibility of vessels. All arterial and venous anastomoses were created with continuous 6/0 or 7/0 polypropylene monofilament sutures under local anesthesia. After surgery, patients were scheduled for follow-up visits at 2 weeks and then at monthly intervals for 3–6 months. Longer follow-up visits were determined at the discretion of an attending surgeon.
First cannulation of the AVF was generally performed 6 weeks after the procedure. AVF maturation was defined as when the fistula could be used for dialysis for at least 6 consecutive sessions [19]. If an AVF failed to attain adequate flow for dialysis, an additional intervention would be performed to promote fistula maturation or patency. An AVF that functioned well at 1 year, regardless of whether it required intervention(s) before or after successful use, was defined as AVF survival, whereas an AVF that failed to function despite additional intervention was defined as AVF loss.
Development of the clinical score
To develop a clinical scoring model, data on ESRD patients who received a new AVF between January 2009 and June 2013, referred to as the “development cohort,” were extracted from the hospital electronic database. The data that were collected were age, sex, body mass index, comorbid conditions, current medications, a history of prior CVC insertion, presence or absence of intervention(s) performed to achieve AVF maturation, and functional status of the AVF 1 year after the first use. Comorbid conditions consisted of diabetes mellitus (DM), hypertension, ischemic heart disease, and cerebrovascular disease. Current medications included antithrombotic agents, statins, calcium channel blockers, angiotensin converting enzyme inhibitors/angiotensin II receptor blockers, and beta blockers. The interventions performed to achieve AVF maturation included surgical and endovascular procedures.
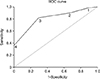
The clinical features that were significantly associated with 1-year AVF survival in the univariate analysis were entered into a multivariate analysis. A clinical scoring system was then developed using the methods described in a previous report [20]. Specifically, the author calculated the number of points assigned to each significant variable by dividing its regression coefficient by the lowest coefficient in the model then rounded this quotient to the nearest integer. These score points were summed to derive a total clinical score. A receiver operating characteristic (ROC) curve was constructed, and the area under the curve (AUC) was calculated to determine the optimal score and its sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) with the associated 95% confidence interval (CI) to predict AVF survival at 1 year.
Validation of the clinical score
The validity of the clinical score was assessed in ESRD patients receiving a primary AVF between July 2013 and December 2017 who were referred to as the “validation cohort.” The patient selection, data collection, and clinical scoring system for this cohort were the same as those for the development cohort. The performance of the clinical score was evaluated according to the AUC, sensitivity, specificity, PPV, and NPV with their 95% CIs.
Statistical analysis
Data were analyzed with IBM SPSS Statistics version 22.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as the means with standard deviations, and categorical variables are expressed as numbers with percentages. Student's t-test was used to compare continuous variables. Categorical variables were compared by chi-square test or Fisher exact test as appropriate. A value of P < 0.05 was considered statistically significant.
This study has been reported in line with the STARD (Standards for the Reporting of Diagnostic Accuracy) criteria.
RESULTS
Among the 195 patients included in the development cohort (Fig. 1), 168 (86.2%) had a well-functioning AVF at 1 year. Patients whose AVFs remained patent had significantly lower rates of DM, prior CVC insertion, and intervention(s) performed to achieve AVF maturation than patients with AVF loss. Other characteristic features of the 2 groups were not significantly different (Table 1).
Clinical score development
The 3 significant clinical features of DM, prior CVC insertion, and intervention(s) performed to achieve AVF maturation in the development cohort were entered into a multivariate analysis. These 3 features retained their significance as independent predictors of AVF survival. The regression coefficient values were 1.066 for DM, 1.406 for prior CVC insertion, and 1.735 for intervention(s) performed. These figures were rounded to the nearest integer by dividing each by 1.066 (the lowest value among the three). The corresponding integer score assignments are presented in Table 2. The total score of each patient varied from 0 to 4 points.
Clinical score validation
Among the 204 patients in the validation cohort, 159 (77.9%) had a well-functioning AVF at 1 year (Fig. 1). Associations between variables and AVF survival in this cohort resembled those in the development cohort (Table 1). The clinical score had acceptable predictive performance for 1-year AVF survival, with an AUC of 0.755 (95% CI, 0.677–0.834). Similar to the findings in the development cohort, the optimal score cutoff with the highest AUC value was ≥3. This cutoff point yielded sensitivity, specificity, PPV, and NPV values of 76.1%, 64.4%, 88.3%, and 43.3%, respectively (Table 3).
DISCUSSION
AVF failure after maturation remains a problem for patients with ESRD. Hence, close postoperative monitoring of these patients is important, especially during the first year of AVF use when access failure occurs most often [7]. From a practical viewpoint, the ability to identify patients who are prone to AVF loss would serve as a surrogate indicator to alert clinicians to the possibility of abandonment of a primary AVF, which consequently results in the creation of a secondary fistula or arteriovenous graft. On the other hand, those who are identified as having little chance of access abandonment would be good candidates for salvage intervention if their AVFs fail to function properly.
To date, only a few studies have investigated the role of clinical scores as predictive indicators for long-term AVF failure after creation [161718]. Twine et al. [16] constructed the DISTAL scoring model using 6 preoperative clinical features for the prediction of 2-month, 6-month, 1-year, and 2-year primary patency of snuffbox AVFs. Their study revealed a trend toward decreased primary patency as the DISTAL score increased. Another study by Bosanquet et al. [17], who created the CAVeA2T2 score based on 5 preoperative and intraoperative clinical parameters to predict the patency of radiocephalic AVFs, found that fistulas with scores ≥2 were significantly associated with reduced 6-week and 1-year patency rates. The predictive ability of this CAVeA2T2 score was further validated in the study by Martinez et al. [18], who observed a good predictive ability of the score among patients undergoing creation of radiocephalic AVFs. The DISTAL and CAVeA2T2 scores were constructed using only preoperative and/or intraoperative parameters to predict both early AVF failure (before fistula maturation) and late failure (after fistula maturation). Therefore, a history of intervention(s) performed to promote AVF maturation, which has been reported to be associated with late AVF failure by some authors [9], was not included as part of either scoring system. The exclusion of this postoperative parameter might affect the ability to predict late AVF loss. In addition, the DISTAL and CAVeA2T2 scores focused only on the snuffbox and radiocephalic AVFs and might not be applied to patients undergoing brachiocephalic AVF, which is another common type of AVF in current practice [2122].
Unlike prior studies, the present study developed and validated a scoring model for the prediction of either radiocephalic or brachiocephalic AVF survival 1 year after cannulation for dialysis use. This clinical score used only 3 readily available clinical variables, so it was simple to calculate. Its AUC values from ROC curves in the development and validation cohorts were quite high at 0.810 and 0.755, respectively, suggesting that the model had high predictive validity. Moreover, analysis of the clinical score in an independent validation cohort revealed similar performance to that in the development cohort, although with a lower AUC, sensitivity, and specificity. These concordant results indicated the reliability of the scoring model for AVF survival prediction.
The clinical score presented herein yielded a high sensitivity of 81.5% for the prediction of AVF survival at 1 year in the development cohort. Hence, it is useful for identifying patients with a score less than 3 who have a high probability of 1-year AVF loss. Furthermore, its high PPV of 94.5% strengthens its role as a predictor of good AVF function at 1 year. Based on these findings, the author suggests that proactive surveillance, including routine clinical monitoring and/or duplex ultrasound [23], should be applied to individuals with a score lower than 3 at regular intervals throughout the first year of AVF use to identify access-related problems early. In the event that an AVF fails to maintain adequate flow on dialysis, these patients should be offered other treatment options, including a secondary AVF or arteriovenous graft, if an initial salvage intervention is unable to reestablish the patency of a primary AVF. On the other hand, repeat salvage interventions of the nonfunctioning AVF should be attempted in individuals with a score of ≥3 because these patients have a better AVF prognosis.
One may question whether this clinical score would yield benefits, because the 3 parameters in the model are already known as predictive factors of AVF survival. Upon further analysis of the data of the patients in the development cohort, the author found that the AUCs of DM, prior CVC insertion, and history of intervention(s) performed to achieve AVF maturation for the prediction of AVF survival were 0.605, 0.646, and 0.675, respectively. These AUC values were much lower than the AUC of 0.810 obtained from the combination of the 3 clinical features. Such findings signified that incorporating multiple parameters into a prediction model would produce a better predictive performance than the use of only a single parameter. In addition, this clinical score can predict the chance that a patient with a given set of clinical risk factors will encounter AVF loss. Hence, it is useful in making clinical decisions and helping patients make an informed choice regarding their treatment.
This study was limited by utilizing a retrospective design. Therefore, data on duplex ultrasound imaging were not available for most patients. Nevertheless, all patients were determined to have vascular anatomy suitable for AVF formation based on preoperative physical examination. Thus, vessel characteristics were not incorporated into the scoring system. Another limitation was that it was conducted in a single center. Therefore, external validation in other settings is needed to confirm its findings. Additionally, this study included only the number of patients with successful cannulation for dialysis use but not the total number of patients who underwent AVF creation. Hence, data on primary failure rate, and 1-year primary and secondary patency rates were unavailable. Furthermore, the scores for each variable were transformed from the original regression coefficients to rounded numbers. This could lead to some loss in predictive accuracy. Nevertheless, upon further analysis of the data of the patients in the development cohort, the author found that the AUC of the model with the original (untransformed) regression coefficients was 0.813 (95% CI, 0.739–0.887). This figure was only slightly higher than the AUC of 0.810 obtained from the proposed scoring model. Thus, the loss in precision of this scoring system was minimal and should not affect clinical relevance.
There were some strengths in the study. First, this was the first study to establish and validate a clinical tool to predict the 1-year survival of radiocephalic or brachiocephalic AVFs, which are the 2 most common types of AVFs performed in current practice. Second, the simple dichotomous no/yes variables in this clinical model were easy to use and did not require a calculator or computer. Lastly, the prediction model included only simple clinical data that can be obtained from a patient's medical history. Hence, utilizing the model is free of charge and can be applied to any patient.
In the present study, a scoring model based on 3 clinical features that predict 1-year AVF survival was developed and validated. This clinical model may guide clinicians in providing personally tailored treatment for patients with a failing primary AVF. As the present study focused only on the survival of a primary AVF at 1 year, the clinical utility of this scoring model for the prediction of AVF survival over longer periods or in patients who undergo repeated AVF creation requires further evaluation.




 XML Download
XML Download