

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Steatocystoma multiplex is a rare benign subcutaneous disease characterized by multiple dermal cyst-like lesions derived from the pilosebaceous glands. Its pathogenesis remains unclear, but it is predominantly referred to as a hamartomatous malformation of the pilosebaceous duct junction.1 Steatocystoma multiplex is most commonly diagnosed in adolescence or early adulthood;2 however, it has been reported as early as birth3 and in patients as old as 78 years old.4 The condition appears to lack any sex or race predilection.5 Although usually asymptomatic, it can cause patients social stress related to their appearance if the lesions are numerous or large, especially on the face and neck. Some cases are sporadic; however, an autosomal dominant inherited type associated with mutations of the gene coding for keratin 17 (KRT17) has also been described.6
Steatocystoma multiplex was first mentioned in a case report published by Jamieson in 1873 involving numerous cutaneous cysts scattered throughout the body.7 This condition has mainly been reported on the trunk and the proximal extremities, though it has been described as occurring on the oral mucosa8 as well. Few previous studies have reported lesions of the head and neck area concurrent with other characteristics resembling ectodermal dysplasia, especially with regard to their radiographic imaging features.
This report aimed to describe a case of steatocystoma multiplex on the cervical area concurrent with several dental anomalies, with a focus on its clinical, radiological, and histopathological characteristics, as well as the possibility that this condition was inherited.
Case Report
A 32-year-old man was referred to Seoul National University Dental Hospital for further evaluation and treatment of bilateral nodular lesions of the neck that had been present for several months. He had visited a local plastic surgery clinic with a chief complaint of a large lesion and pain in the right cervical area. Documentation from the clinic stated that he had only agreed to a drainage procedure and had refused surgery to remove the lesions. According to the patient, the pain and swelling had subsided as a result of the aspiration performed during his visit to the clinic. Additionally, while the patient had an operative history of cardiac septal defect repair performed when he was 10 months old, he gave no family history associated with skin lesions like those that he exhibited.
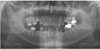
Panoramic radiography showed abnormal dentition. First, the deciduous second molars were in a state of prolonged retention and submergence on both sides of the maxilla and the right side of the mandible. Second, multiple permanent teeth were missing, including the maxillary second premolars on both sides and 2 mandibular incisors on both sides and 1 mandibular molar on the right side. Finally, microdontia of 2 maxillary lateral incisors (peg lateral incisors) and 2 mandibular premolars was observed (Fig. 1).
To accurately evaluate the soft-tissue lesions, contrast-enhanced computed tomography (CECT) was performed. The images revealed multiple well-defined round to ovoid, smooth or scalloped, nodular lesions with diameters ranging from 2 to 20 mm in the subcutaneous layer on both sides of the cervical region. The internal structure showed fat attenuation on the level of −110 to −100 Hounsfield units (HU) and some lobulation. Additionally, the large lesion of the right upper neck, where the patient experienced the pain, displayed peripheral enhancement with mild swelling, suggesting that it was accompanied by inflammation. The epidermis of that lesion was elevated, and the adjacent platysma muscle and external jugular vein were displaced medially (Fig. 2). In other words, the benign lesion exerted a pushing force on adjacent structures. Based on these radiographic findings, the initial diagnosis was lipomatosis.
For microscopic examination, excisional biopsy was performed on a lesion (7×5×4 mm) on the right side of the neck, and hematoxylin and eosin staining was used. The histological finding was a subcutaneous cystic lesion containing sebum-like material. At the lowest magnification (×12.5), a cavity surrounded by a thin epithelial lining that formed part of the cyst wall was observed. The middle magnification settings (×40 and ×100) showed the specimen to have a wall lined by 3 to 5 layers of keratinized stratified squamous epithelium lacking a granular layer, and many sebaceous lobules were located very close to, as well as within, the cyst wall. In addition, a wavy luminal surface and sebum-like material or keratin debris were detected. The highest magnification (×400) showed numerous lobules of pilosebaceous glands on the cyst wall. The granular layer was completely absent (Fig. 3). Accordingly, the analysis resulted in a diagnosis of steatocystoma multiplex.
The patient revisited with bleeding of the above-mentioned large lesion of the right neck 6 months after the biopsy. The aspiration contained serous fluid, blood, and sebum-like material. His discomfort was relieved with medication a few days later, and he required no further visits.
Discussion
Steatocystoma multiplex consists of benign cystic lesions derived from the sebaceous glands. The lesions are macroscopically smooth and uniform with a size of a few millimeters to centimeters along the long axis. Their color is usually whitish or yellowish, which likely reflects sebum-like material in the cystic cavity. Therefore, small lesions can be clinically confused with acne conglobata or milia. Furthermore, it is difficult to differentiate steatocystoma multiplex from some dermal cystic lesions of different origin, such as dermoid/epidermoid cysts, multiple lipomas, and xanthomatosis, on the basis of CECT imaging findings, as these types of lesions are also characterized by low internal attenuation.9
Histopathologically, steatocystoma is defined as a dermal cystic lesion containing sebum or sebum-like material and keratin debris, characterized by lobules originating from sebaceous glands, and lacking a granular layer. These features are critical to distinguish steatocystoma from eruptive vellus hair cysts, which have a similar appearance, age of onset, and distribution pattern. An eruptive vellus hair cyst is formed by several layers of squamous cells, with vellus hairs as well as keratinous material in the cavity.1011
As mentioned, the familial form of steatocystoma multiplex has been described as a phenotypic variant of an autosomal dominant inherited disease associated with mutations of KRT17. Mutations of these genes have also been identified in patients with pachyonychia congenita type 2 (PC-2).12 Pachyonychia congenita (PC) has 2 main types, PC-1 (the Jadassohn-Lewandowsky form) and PC-2 (the Jackson-Lawler form). Common clinical features of PC-2 include hypertrophic nail dystrophy, natal teeth, and hair abnormalities.13 Individuals with PC-2 may also develop dermal cysts, including steatocystoma multiplex.14
In PC-2 patients, various dental anomalies - for instance, early primary tooth loss,13 natal or neonatal teeth,15 Hutchinson-like teeth,16 and friable adult teeth17 - are also commonly recognized. The congenital absence of secondary dentition with persistent partial primary dentition, which was exhibited by our patient, was first described by Gass et al.18 They reported the identification via DNA analysis of a missense mutation in KRT17 in the described patient and his sister. Gass et al. showed that the amino acid substitution was located in the 2B domain, not in the 1A domain, which is the typical site of the mutations involved in steatocystoma multiplex and PC-2. That report can be said to extend the range of dental anomalies recognized in cases of PC-2.
Taken together, the features of our case were sufficient to suggest ectodermal dysplasia. Among them, association with KRT17 mutations or PC-2 have been established for steatocystoma multiplex and the dental anomalies described above, while no such association has been established for cardiac septal defect. Unfortunately, in our case, the patient's family history was not obtained, and a genetic analysis was not conducted. Therefore, we cannot be certain that this case reflects a genetic condition; however, it certainly represents steatocystoma multiplex with dental anomalies.
Steatocystoma multiplex is a benign disease that typically does not cause any symptoms or discomfort. Therefore, it can be overlooked or excised simply for aesthetic reasons. It is likely that the pain that spurred the patient described herein to seek treatment stemmed from a secondary infection. However, since the possibility of a KRT17 mutation cannot be excluded in cases presenting with multiple cysts consistent with steatocystoma multiplex, patients should be carefully examined with regard to family history and the presence of other ectodermal abnormalities, and a histological assessment should be performed as needed.
In conclusion, steatocystoma multiplex is an uncommon benign skin disease that is particularly rare in the head and neck region. Due to the high potential of association with a KRT17 mutation, a biopsy is recommended. CECT is useful for defining the locations, shapes, internal structures, and effects on surrounding structures of these cyst-like lesions.


 XML Download
XML Download