

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Osteomyelitis (OM) is an inflammatory condition of the bone, beginning in the medullary cavity and Haversian system and extending to involve the cortex and periosteum of the affected area.1 OM of the jaw is a fairly common disease of the oral and maxillofacial area, and extensive research has investigated the pathophysiology, diagnosis, treatment, and prognosis of OM. The large number of bacteria harbored in the oral cavity, as well as the high frequency and severity of odontogenic infections in daily dental practice, have been thought to be reasons why OM of the jaw is relatively more common than OM of other skeletal bones.1 The overall incidence of OM has decreased due to the development of antibiotics and improvements in dental and medical care; however, OM of the jaw has become more prevalent in recent years. The growth of the aged population, along with the increased use of antiresorptive medications such as bisphosphonates, has resulted in an increased rate of complications, including jaw necrosis,2 and this increased complication rate could be a predisposing factor for the increased rate of OM.34
Medication-related osteonecrosis of the jaw (MRONJ) is an osteonecrotic condition of the jawbone that is associated with antiresorptive (e.g., bisphosphonate and denosumab) and antiangiogenic agents. MRONJ has been described as necrosis resulting from non-inflammatory drug toxicity;5 however, some reports have posited that MRONJ may be an infectious disease or triggered by exposed bone and subsequent infection.678 In addition, infection of the jaw can occur without bone exposure. For these reasons, MRONJ is currently understood to include not only necrosis but also the entire associated inflammatory condition due to the increased probability of. Multiple symptoms, signs, and radiographic changes caused by OM and MRONJ appear similar, and the differentiation of MRONJ from OM using clinical symptoms and radiographic images may be difficult in patients without a history of medication use or bone exposure.
This study defined OM as the entirety of inflammatory conditions of the jaw, including MRONJ. The aim of this study was to analyze the clinical features of contemporary OM and to investigate imaging differences on panoramic radiographs according to patients' history of use of medications that impact bone metabolism.
Materials and Methods
Subjects
A retrospective study was conducted that involved reviewing the electronic records and images of 364 patients diagnosed with osteomyelitis via clinical, radiological, and histopathological examinations at Seoul National University Dental Hospital between January 1, 2014 and December 31, 2015. Patients' records, including medical and dental records and panoramic radiographs, were selected for the study. The exclusion criteria were recurrent OM and OM occurring adjacent to sites of previous operations to treat cancer. The current study was exempted from review by the Seoul National University Hospital Institutional Review Board (IRB066/05-19).
Analysis of clinical records
General demographic information was gathered using electronic dental records. The clinical symptoms exhibited, duration of symptoms, and previous medical history – including a specific history of antiresorptive medication use, previous dental history, and treatment history – were also recorded. The presumed causes of OM were categorized by the consensus of 2 examiners as antiresorptive medication use, odontogenic origin, radiation therapy, infection of a fibro-osseous lesion, orthognathic surgery, trauma, and unknown cause.
Analysis of images
The panoramic imaging features of the scans of the 340 patients were analyzed, excluding 24 patients who had site-specific causes, such as osteoradionecrosis, orthognathic surgery, and trauma. Most panoramic images were taken with an OP100 device (Instrumentarium Dental, Tuusula, Finland). All panoramic images were reviewed by 2 oral and maxillofacial radiologists each with more than 15 years of experience. The image findings were analyzed in a picture archiving and communication system (PACS; INFINITT Healthcare, Seoul, Korea).
The pattern of each lesion was classified as osteolytic, sclerotic, or mixed (Fig. 1). The presence of sequestrum, periosteal new bone formation, extraction sockets, and cortical bone involvement via osteolysis or sclerosis of the lesion were evaluated (Fig. 2). Additional radiomorphometric analyses were performed to evaluate the following parameters: mandibular canal wall change (categorized as lysis, thickening, adjacent sclerosis, or no change), the mandibular cortical index (MCI; categorized as C1, C2, or C3), and the extent of the lesion (categorized as alveolar cortex, above the mandibular canal, between the mandibular canal and the mandibular cortex, or mandibular cortex).
Statistical analysis
The authors compared the differences in clinical and imaging features between patients with antiresorptive medication-related OM (m-OM) and those with conventional, medication-unrelated OM (c-OM), with patients classified according to their history of antiresorptive medication use. Twenty-four patients with site-specific causes such as osteoradionecrosis, orthognathic surgery, and trauma were excluded in order to facilitate a pure comparison of panoramic imaging features. Statistical analysis was performed using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). Values for all parameters were expressed as percentages. The Pearson chi-square test and the Student t-test were used to compare groups. A P value less than 0.05 was considered to indicate statistical significance.
Results
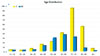
A total of 364 patients (241 female [66.2%] and 123 male [33.8%]) were included in this study. Their average was 66.8±14.9 years (for the female patients, 69.6±14.7 years; for the male patients: 61.5±14.0 years; range, 10–91 years). The age of onset of OM tended to be high and was most frequently observed in patients in their 70s (Fig. 3). The most common clinical findings of the patients with OM are shown in Table 1. Pain and swelling were the most frequent symptoms, and the average duration of symptoms was 4.7±8.1 months (range, 2 days to 5 years). Most patients (83.8%) had underlying diseases such as hypertension, osteoporosis, or diabetes, and 161 patients (44.2%) had a history of antiresorptive medication (mostly bisphosphonate) use; of these, 133 patients (82.6%) had been given oral medication, while 28 (17.4%) patients had been given intravenous medication. The average period of antiresorptive medication use was 4.5 years. The most frequent presumed causes of active OM were antiresorptive medication use and odontogenic origin (Table 1).
Most lesions occurred in the mandible (maxilla : mandible ratio=68 : 303 lesions; 7 patients had both mandibular and maxillary lesions). The most common finding on the panoramic radiographs was a mixed pattern of osteolysis and sclerosis, and the second most common finding was an osteolytic bone pattern. Sequestra were observed in 143 cases (42.1%), and periosteal new bone was found in 24 cases (7.1%) (Table 2).
To compare the imaging features, 340 patients (female : male=232 : 108) were divided into 2 groups (m-OM and c-OM). There was little difference between the groups with regard to the distribution of maxillary and mandibular lesions. In the m-OM group, the patients were older on average, and the group contained a higher proportion of female patients (female : male=153 : 9, Table 3). On the panoramic radiographs, sequestrum and extraction sockets were more frequently observed in the m-OM patients than in the c-OM patients. In contrast, periosteal new bone formation was more frequently observed in the c-OM group. The MCI was significantly higher in m-OM patients than in c-OM patients (Fig. 4A). The changes in the wall of the mandibular canal and the extent of the lesion did not differ significantly between the groups (Figs. 4B and C).
Discussion
In the present study, the features of contemporary OM of the jaw were assessed using a large number of patients to determine the differences in panoramic image findings between antiresorptive m-OM and c-OM, given their concordant clinical features. The most common age of onset of OM was in the patients' 70s. A mixture of osteolysis and sclerosis was the most frequent imaging feature observed (68.6%), while sequestrum, extraction socket, and periosteal new bone formation were found in fewer than half of the patients. When comparing patients according to their history of antiresorptive medication use, sequestrum and extraction socket were more frequently observed in patients with medication-related OM. The MCI was significantly higher in m-OM patients than in c-OM patients.
Some previous studies have examined the clinical and imaging features of OM. The average age of onset and the rate of occurrence in female patients were higher in the present study than in previous reports (Table 4).91011 The more recent the study, the more the age of onset and predominance in female patients were found to increase. In addition, in this study, the most common presumed cause was antiresorptive medication use; however, most previous studies have reported that the most frequent cause was odontogenic infection.911 Approximately half of our OM patients had a history of antiresorptive medication use, and the sex distribution was significantly different between the 2 groups (Table 3). This may be due to the fact that the number of elderly people taking antiresorptive medication has increased significantly over time. Although the incidence of OM has decreased and the rate of MRONJ as an adverse effect of antiresorptive medicine use remains relatively low, millions of elderly people are currently being treated with these medications. The use of antiresorptive drugs has been popularized in the last few decades for the treatment and prevention of bone diseases such as osteoporosis, Paget's disease, hypercalcemia of malignancy, and bone metastasis, all of which are common conditions in an aging society.12 This fact may well explain our results regarding why the age of onset and the relative frequency of OM in women has increased in present society.
As MRONJ becomes more common as a side effect of antiresorptive medication use, our overall understanding of inflammation of the jaw is changing. When MRONJ involves osteonecrosis or bone exposure, the lesion can easily become infected by oral microbes or pathogens and has a high chance of becoming inflamed. Long-term jaw-bone exposure and the presence of intraoral or extraoral fistulas in MRONJ patients are causes of infection that can induce osteomyelitic lesions,13 and infected osteonecrosis is the most serious form of OM.14 Moreover, infection of the jaw can occur even without bone exposure or fistula opening.15 Therefore, MRONJ should be no longer be understood as simply necrosis itself, but rather as the entire related process of inflammation.
Although the occurrence of MRONJ has increased with the increased use of antiresorptive medications, it has not been clear how to differentiate between OM and MRONJ. Previous studies have reported that a history of antiresorptive medication use and a clinical finding of bone exposure are keys for the diagnosis of MRONJ.13 However, MRONJ can develop and progress without bone exposure, and using bone exposure and medication history as criteria for the diagnosis of MRONJ leads to delayed diagnoses and a poor response to treatment.16 Several previous studies have attempted to identify pathognomonic imaging features of MRONJ; however, most of those studies used 3-dimensional (3D) imaging modalities.151718 As panoramic radiography is typically used as part of the basic examination performed in dental clinics, we hypothesized that the early detection of signs of MRONJ using panoramic radiography, along with medication history, could be extremely helpful in diagnosing MRONJ. In the present study, sequestrum and extraction socket were observed significantly more frequently in the medication-related group. Although features such as sequestrum and extraction socket can also be found in cases of OM, these findings suggest that MRONJ is a possibility when no apparent cause of infection is visible on panoramic radiography. Although periosteal new bone formation was more frequent in the c-OM group than in the m-OM group, we believe that this feature is difficult to use to differentiate between OM and MRONJ because periosteal new bone can only be detected on a panoramic radiograph when it is located in the mandibular cortex and because the frequency of periosteal new bone formation is too low to function as a clinically useful parameter. With regard to MCI, C1 was more frequently found in the c-OM group, while C3 was more often observed in the m-OM group. However, it was difficult to interpret whether this was due to the alteration of bone metabolism, as in osteoporosis, or whether it was an effect of the antiresorptive medication.
The present study had some limitations, the most noteworthy of which was that imaging analysis was conducted using only panoramic radiography. Considering the fact that most patients undergo 3D imaging – such as computed tomography or magnetic resonance imaging – for the planning of surgery, a more accurate comparison could be drawn by using these 3D imaging modalities, especially with regard to certain imaging features, such as periosteal new bone or sequestrum. Second, this study had a retrospective design, so it was insufficient for gathering detailed information such as the specific type of medication used, the exact staging of MRONJ as determined by objective clinical signs, and treatment and prognosis. Further investigations of the predictive imaging factors that can be observed before the occurrence of MRONJ are needed. By comparing the serial panoramic radiographs of asymptomatic patients who take antiresorptive medication as part of their routine follow-up in future studies, we may be able to understand the entire process of MRONJ development.
This study evaluated the clinical and panoramic features of infected jawbones in a large number of patients by comparing patients with antiresorptive medication-related OM to those with OM unrelated to medication use. It may be useful as a basic study for understanding the imaging features that can predict MRONJ onset.







 XML Download
XML Download