

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Nonsteroidal anti-inflammatory drugs (NSAIDs) are one of the most commonly used drugs worldwide, as either prescriptions or over-the-counter medications.1 Adverse drug reactions (ADRs) of NSAIDs account for 12% to 29.6% of all ADRs in hospital admissions.2 Most ADRs of NSAIDs belong to type A,3 which are dose-dependent and predictable from pharmacological actions of the drugs. Common type A reactions include gastrointestinal bleeding and acute kidney injury.4 Type B reactions, also known as NSAID hypersensitivity reactions, account for 8.4% to 18.3% of total ADRs of NSAID.56 They are idiosyncratic and pharmacologically unpredictable. NSAID hypersensitivity reactions pose classification as well as diagnostic and management challenges in clinical practice. The aim of this review is to provide the latest update on the classification of NSAID hypersensitivity and practical approaches to the diagnosis and management of NSAID hypersensitivity, according to the current systematic classification system.
The articles were retrieved via PubMed using the following keywords: nonsteroidal anti-inflammatory agents, hypersensitivity reactions, asthma, chronic urticaria, and angioedema. Only studies published in English were evaluated.
PATHOPHYSIOLOGY AND CLASSIFICATION OF NSAID HYPERSENSITIVITY
NSAIDs consist of drugs with diverse chemical structures and anti-inflammatory properties. Most NSAIDs have nonselective inhibitions of COX-1 enzymes. They interfere with arachidonic acid metabolism, leading to blockage of prostaglandin synthesis and up-regulation of the leukotriene pathway that contributes to various presentations of NSAID hypersensitivity reactions.7 NSAIDs that possess predominant inhibition of COX-1 enzymes, such as indomethacin, naproxen, and diclofenac, have higher rates of hypersensitivity reactions, while weak COX-1 inhibitors and selective COX-2 inhibitors are often better tolerated with a lower probability of hypersensitivity reactions.
Hypersensitivity response to paracetamol is also regarded as a type of NSAID hypersensitivity reaction, as one-third of the patients with history of NSAID hypersensitivity reactions also suffer from cross-reactions with high-dose paracetamol.8
The current classification of NSAID hypersensitivity is based on the time of symptom onset, underlying pathophysiology, clinical symptoms, and the presence of cross-reactivity with other NSAIDs, as summarized in Fig. 1.
Acute or immediate hypersensitivity reactions refer to reactions with clinical symptoms starting within 1 hour after intake of the culprit drug.9 Both IgE-mediated and non-immunological hypersensitivity reactions can lead to acute onset of symptoms. The onset time of delayed hypersensitivity reactions is more variable, ranging from 24 to 72 hours after administration of the drug. Delayed hypersensitivity reactions are usually mediated by T cells.
According to the European Network of Drug Allergy, NSAID hypersensitivity reactions can be divided into non-immunologically and immunologically mediated subgroups, in which specific IgE or T cells are involved.10
Non-immunologically mediated NSAID hypersensitivity reactions are caused by disturbance of arachidonic acid metabolism, dysfunction of 5-lipoxygenase leukotriene C4 synthase (LTC4S), reduction in prostaglandin (PG) E2, and increased production of cysteinyl leukotrienes (CysLTs), hence triggering systemic inflammation and hypersensitivity symptoms.11 Cross-reactivity is found among NSAIDs with different chemical structures. Major clinical phenotypes of NSAID hypersensitivity reactions induced by non-immunological mechanisms include NSAID-exacerbated respiratory disease (NERD), NSAID-induced urticaria/angioedema (NIUA), and NSAID-exacerbated cutaneous disease (NECD).
In NERD, the role of CysLTs has been illustrated by increased levels of urinary CysLT before and after aspirin challenges compared to aspirin-tolerant asthma.1213 Decreased levels of PGE2 enhance LTC4S pathway, which accelerates CysLT production.14 Overproduction of CysLT leads to vascular leak, bronchoconstriction, and excess mucus secretion, as well as activation of mast cells and eosinophils. Stimulated mast cells and eosinophils release chemical mediators and cytokines, which further increase systemic inflammation. Furthermore, aspirin/NSAID can directly promote the activation of eosinophils and mast cells.15 Stimulated innate immune responses with up-regulated IL-33/thymic stromal lymphopoietin (TSLP) can induce eosinophil activation and facilitate production of cytokines, such as IL-5, IL-9, and IL-13, in patients with NERD.16 Activated eosinophils release extracellular vesicles that promote asthma exacerbation. They also secret extracellular traps, which contribute to reactive oxygen species production and thereby induce airway inflammation. 17 Genetic and epigenetic variance in NERD patients and aspirin-tolerant asthmatic patients provide insights into the mechanism of NERD predisposition. Single nucleotide polymorphisms (SNPs) related to NERD cause dysregulation of CysLTs/PG production. Epigenetic studies have shown that reduction in PGE production is due to hypomethylation of PGE receptors by SNP, while overproduction of CysLT is caused by hypermethylation of CysLT receptor 1 and 2 by SNP. SNPs on HLA-DPB1 increases susceptibility of NERD. SNPs that regulate the number of CpG sites are less frequently seen in NERD patients compared to aspirin-tolerant asthma patients.18 The complex interplay among SNP, PG, CysLTs, and inflammatory cells makes NERD patients suffer from more severe type 2 airway inflammation.
There are two cutaneous phenotypes of NSAID hypersensitivity reactions: NECD and NIUA. In NECD, patients have a history of chronic urticaria, which can be exacerbated by aspirin/NSAID exposure.19 On the other hand, patients with NIUA do not suffer from chronic urticaria but develop urticaria, angioedema, and/or anaphylaxis only after the exposure to at least two NSAIDs with distinct chemical structures.20 The underlying pathophysiology of NECD and NIUA is not completely recognized; however, it is believed to have overlapping features in the defects in arachidonic acid metabolism. This can be illustrated by the increase in urinary CysLT levels and depletion of PGE2 in patients with NECD and NIUA after aspirin challenges.2122 However, there are some distinctive pathophysiological features in NECD. Degranulation of basophils is more severe in patients with NECD.23 Genetic polymorphisms of alpha-chain of the high-affinity IgE receptor and HLA allele markers, such as DRB11302 and DQB10609, were more frequently detected in patients with NECD/NIUA,2425 suggesting that mechanisms related to mast cell activation should be further investigated.
Single NSAID-induced urticaria/angioedema or anaphylaxis (SNIUAA) is the only IgE-mediated type among NSAID hypersensitivity reactions. SNIUAA is defined as the presence of urticaria, angioedema, and/or anaphylaxis caused by the production of IgE antibodies to a single NSAID or NSAIDs with similar chemical structures. Aspirin or NSAID-specific IgE antibodies bind to high-affinity IgE receptors on the surface of mast cells and basophils, hence triggering massive production of chemical mediators (e.g., histamine and platelet activating factors) and causing urticaria, angioedema, and even anaphylaxis. Among different types of NSAID, pyrazolone is the most common culprit drug class responsible for IgE-mediated NSAID hypersensitivity reactions.26
T cell-mediated NSAID hypersensitivity reactions are the only delayed-type hypersensitivity reactions. Dendritic cells recognize NSAID antigens and present them to naïve T cells, leading to the production of activated antigen-specific T cells. Antigenspecific T cells release cytokines and cytotoxins, which further provoke systemic inflammation.27 There is a wide range of clinical manifestations including fixed drug eruption, erythema multiforme, and life-threatening conditions, such as drug reaction with eosinophilia and systemic symptoms (DRESS), Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN).28
There are various predisposing factors for NSAID-induced hypersensitivity reactions. They are either related to the chemical structures of NSAID or the characteristics of individual patients. There is a higher risk of anaphylaxis in the propionic acid group of NSAIDs and pyrazolones. Also, patients are more likely to develop delayed hypersensitivity reactions of severe cutaneous adverse reactions when taking propionic acids.29 On the other hand, selective COX-2 inhibitors have much lower risks of hypersensitivity reactions compared to non-selective COX inhibitors.3031 Regarding patient characteristics, female sex, history of autoimmune diseases, and prior history of hypersensitivity reactions to other drugs have been shown to be risk factors for NSAID hypersensitivity reactions.5 Patients with history of atopy are also predisposed to NECD or NIUA.3233
DIAGNOSTIC APPROACH FOR PATIENTS WITH NSAID HYPERSENSITIVITY
Although NSAID hypersensitivity reactions are commonly seen, the correct diagnosis and classification of NSAID hypersensitivity is not straight forward. A comprehensive diagnostic algorithm is necessary for categorizing clinical phenotypes of NSAID hypersensitivity reaction, so that the management plan and prognosis of individual patients can be ascertained and safe alternatives can be identified. The diagnostic algorithm should include clinical history, physical examination, and specific provocation tests. Currently, there is no fully validated in vitro testing.34 The diagnostic algorithm is summarized in Fig. 2.
Clinical history and physical examination
A detailed history is extremely important for the identification of clinical phenotype of NSAID hypersensitivity that patients suffer from. It should include the time of symptom onset, details of the symptoms experienced, correlation between symptoms and ingestion of the culprit drug(s), concomitant medications, personal history of atopy, and the names of tolerated NSAIDs that patients are aware of.
In NERD, patients are commonly middle-aged women who are suffering from both upper (severe recurrent chronic rhinosinusitis and/or nasal polyps) and lower respiratory symptoms (mainly moderate to severe asthma).35 These symptoms arise within 30 to 120 minutes after exposure to at least two different chemical classes of NSAID. NERD patients may have coexisting ocular, urticaria, and gastrointestinal symptoms, with respiratory symptoms predominant. Lee, et al.36 stratified four sub-phenotypes of NERD, based on the combination of NERD with chronic rhinosinusitis (CRS), atopy, and urticaria. These included subtype 1 (NERD with CRS and atopy), subtype 2 (NERD with CRS), subtype 3 (only NERD), and subtype 4 (NERD with urticaria). Patients with subtype 1 suffered from more frequent asthma exacerbations, requiring more prevalent use of a combination of medium-to-high-dose of inhaled corticosteroids (ICS)/long-acting beta-agonist (LABA) as well as systemic corticosteroids due to asthma exacerbation. Both subtypes 1 and 2 had higher levels of serum/sputum eosinophilia. Classification of NERD subtypes has enabled better understanding of the pathophysiology of NERD.
All patients with NECD, NIUA, and SNUIAA suffered from urticaria, angioedema, and/or anaphylaxis. They developed wheals, angioedema, or both within 1 to 6 hours after aspirin and/or NSAID exposures. Anaphylaxis was more commonly observed in patients with SNIUAA.37 NECD patients had a history of chronic urticaria, while NIUA patients did not. There was a discrete phenotype of NIUA, with predominant facial angioedema and minimal urticaria. This was associated with hypersensitivity reactions to two house dust mites (Dermatophagoides farinae and Dermatophagoides pteronyssinus).38 Patients with NECD and NIUA had cross-reactivity to NSAIDs with various chemical structures. Patients with SNIUAA suffered from cutaneous symptoms, only after ingestion of a single NSAID or NSAID sharing similar chemical structures.39 In conclusion, a precise history of the types of intolerable NSAIDs is fundamental for an appropriate diagnosis.
Delayed NSAID hypersensitivity reactions were rarely noted, and symptom onset varied from 2 days to 6 weeks after NSAID administration. Diffuse maculopapular eruption, erythroderma, and skin desquamation were observed in DRESS, SJS, and TEN, while mucosal erosions were only relevant in TEN and SJS patients. On the other hand, eosinophilia and liver function derangement were typical features of DRESS.40 Physical examination is essential, particularly for cutaneous subtypes of NSAID hypersensitivity reactions. Pattern recognition of skin lesions, evaluation of mucosal involvement, and assessment of the extent of skin involvement facilitate a correct classification, prognostic estimation, and appropriate management.
Diagnostic tests
The investigation and management strategy of NSAID hypersensitivity reactions is summarized in Fig. 3. Intradermal skin test and skin prick test are only useful for picking up patients with IgE-mediated NSAID hypersensitivity reactions, which is SNIUAA. Previous studies have documented the reliability of skin tests with pyrazolones, but few have suggested satisfactory correlations with other NSAIDs.41 Delayed skin patch test may be useful for delayed NSAID hypersensitivity reactions. The positivity rate of skin tests decreases with time; therefore, it is better to perform skin tests once after the resolution of drug rash. However, standardized protocols for skin tests are lacking, with variable sensitivity and specificities among different centers. Skin tests are not useful as they are not officially validated for the diagnosis of non-immunological NSAID hypersensitivity reactions.42
Aspirin provocation test is considered to be the gold standard investigation for NSAID hypersensitivity reactions. Aspirin can be administered in oral, nasal, bronchial, or intravenous forms; nonetheless, oral and bronchial challenge tests are more commonly performed. Aspirin oral provocation test (OPT) is more sensitive and convenient compared to other aspirin tests. The sensitivity and specificity of aspirin OPT were reported to be 89% and 93%, respectively.43 Aspirin bronchial challenge has a lower sensitivity, but a similar specificity compared to aspirin OPT. It is considered to be a safer and easier approach for assessing patients with suspected NERD. Intranasal provocation with ketorolac had a low sensitivity, and hence was abandoned in the routine evaluation of NERD. In all cases, supervision by an experienced physician, along with a well-equipped resuscitation trolley, are required to ensure a safe and controlled environment to avoid NSAID-induced anaphylaxis during provocation tests.
The EAACI/GA2LEN (European Academy of Allergy and Clinical Immunology/Global Allergy and Asthma European Network) 2011 guideline provides the most comprehensive reference for aspirin provocation, and thereby has been the most frequently cited protocol in the literature.44 It recommends a placebo on day 1, followed by genuine aspirin provocation on the next day. Baseline pulmonary function test is performed to exclude unstable asthma states, which are defined as forced expiratory volume in 1 second (FEV1) less than 70% predicted or 1.5 L. A four-step approach to consecutive aspirin administration (71, 117, 312, and 500 mg) is performed every 1.5 to 2 hours. An ultimately high dose of aspirin challenge (650 mg) can be given to patients who are highly suspected of having multiple NSAID hypersensitivity, but with an unexpectedly negative aspirin OPT result. FEV1 is measured every 30 minutes after intake of each aspirin dose. Presence of respiratory symptoms or over 20% decline in FEV1 from baseline are noted as positive responses in aspirin OPT.
For aspirin bronchial challenge test, a mixture of lypophilized lysine-aspirin and 0.9% saline (up to 300 mg/mL) is delivered via a nebulizer. The concentration of aspirin obtained is determined by the concentration of lysine aspirin mixture and the total number of inhalations. FEV1 is measured as baseline, 10, 20, and 30 minutes after each dose. A decline in over 20% of baseline FEV1 after the administration of lysine aspirin supports the diagnosis of NERD.
Either oral or bronchial aspirin provocation test can be performed in patients with suspected NERD. Aspirin OPT can be repeated when patients show negative results in bronchial aspirin challenge. However, the time-consuming, long and tedious procedure of EAACI/GA2LEN 2011 protocol restricts its use in clinical practice. Regimens with shorter dosage intervals (1 to 1.5 hours), a larger starting dose of aspirin (40 mg), and a higher rate of dose escalation have been used for the procedure. They were shown to have similar safety and tolerance profiles; therefore, they can be readily applied in clinical settings.4546 On the other hand, only aspirin OPT can be performed in patients with aspirin/NSAID-induced cutaneous manifestations.
OPT is a key to determining appropriate phenotypes of cutaneous NSAID hypersensitivity reactions.47 It is considered positive when urticaria and/or angioedema are induced within 6 hours of drug exposure.48 If patients suffer from acute and chronic urticaria associated with NSAID hypersensitivity, aspirin OPT is recommended to confirm the sensitivity. A positive OPT result signifies cross-reactivity of NSAIDs, and a diagnosis of either NECD or NIUA can be made based on the history of chronic urticaria. On the other hand, OPT negativity equates with single NSAID hypersensitivity cases, and hence confirms SNIUAA.49 If aspirin is the suspected culprit drug, a strong COX-1 inhibitor can be chosen for OPT instead. There is no consensus on whether to perform OPT for the culprit NSAID(s), and it is contraindicated in patients with prior anaphylaxis to the offending drug. Since there is no standardized protocol for aspirin/culprit NSAID OPT for delayed NSAID hypersensitivity reactions, it is not generally not recommended.50 Aspirin/culprit NSAID OPT may help confirm a diagnosis of fixed drug eruption and maculopapular drug eruption. On the other hand, OPT is contraindicated in patients with prior severe cutaneous adverse reactions to aspirin and/or NSAID, as they are potentially life-threatening conditions. If aspirin/culprit NSAID OPT is positive, COX-2 inhibitor and paracetamol OPT should be performed to look for safe alternatives. High-dose paracetamol OPT (1000 mg) should be used, as most positive oral challenges are seen only in high-dose paracetamol.
In vitro tests have been studied regarding their effectiveness in identifying NSAID hypersensitivity, including basophils activation test (BAT), serum periostin, surfactant protein D (SPD)/folliculin concentration, urine leukotriene E4 (LTE4) level, and lymphocyte transformation test (LTT). In BAT, increased expressions of CD63 and CD203c markers after in vitro stimulation with allergens were observed by using flow cytometry in patients with allergen-specific hypersensitivity.51 BAT with a combination of aspirin and diclofenac had a sensitivity of 58.3% and a specificity of 93.3%.52 The role of BAT was emphasized when aspirin provocation test was contraindicated; however, technical and analytical difficulties restrict BAT in clinical use.53 Urine LTE4 level is a potential biomarker for NSAID hypersensitivity reactions, especially in NERD, as it is much higher in NERD patients;54 however, studies concerning the relationship between urinary LTE4 level and NECD or NIUA are scarce, with only one small-scale clinical study suggesting elevation of urinary LTE4 levels in NECD/NIUA patients after aspirin challenge.22 SPD, a lipid and protein complex produced by airway epithelium, is responsible for eosinophil and mast cell suppression as well as phagocytosis induction for pathogen clearance. SPD initiates a protective mechanism against airway epithelial damage. Decreased serum or bronchoalveolar lavage SPD levels are associated with a higher severity of type 2 inflammation, especially in NERD patients, which was confirmed by an in vitro study.55 However, application of serum SPD in NERD is still preliminary and largely experimental. Folliculin, an intracellular protein expressed by multiple inflammatory cells, disrupts the integrity of airway epithelial cells. Serum folliculin is significantly higher in NERD patients compared to patients with aspirin-tolerant asthma, but further clinical studies are required to standardize the cut-off value.56 Periostin, an extracellular matrix protein produced by lung fibroblasts and epithelial cells under IL-4 and IL-13 stimulation, has recently been found to be the predictor of type 2 airway inflammation and a key factor for airway remodeling and permanent airway damage. There are significantly high periostin concentrations in both serum and exhaled breath condensate during asthma exacerbations.57 LTT detects T-cell proliferation after drug exposure in an in vitro setting. It is important to confirm causative drugs in patients with delayed NSAID hypersensitivity reactions;58 however, its low sensitivity and technical issues limit the use of these tests in clinical practice. Moreover, validation of potential biomarkers and qualification of in vitro tests help identify phenotypes and endotypes of NERD patients; therefore, precise management decisions can be made with better treatment efficacy.59
TREATMENT
NSAID avoidance
Strict NSAID avoidance is essential for the prevention of acute exacerbation of allergic conditions related to NSAID hypersensitivity. Cross-reactivity of NSAID occurs in patients with NERD, NECD, and NIUA; therefore, all COX-1 inhibitors should be avoided. Tolerance tests of COX-2 and paracetamol should be performed due to potential cross-reactivity. For patients with SNIUAA and NSAID-induced delayed hypersensitivity reactions (NIDHR), culprit NSAID avoidance is required. Clear drug labeling, use of drug allergy passport, and comprehensive patient-education ensure that both healthcare providers and patients know about NSAID hypersensitivity status and safe alternatives. The management strategies of NSAID hypersensitivity reactions can be classified according to the sub-phenotypes reported.
Pharmacological management of NERD
The treatment goals of NERD include prevention of further triggering of NSAID hypersensitivity, satisfactory control of asthma and CRS, and prevention of disease complications, especially recurrence of nasal polyps and lung function decline. The latest EAACI guideline for the management of NERD offers a comprehensive and precise treatment approach in NERD patients.60 The Global Initiative for Asthma (GINA) guideline 2019 provides insights into disease control and management of acute exacerbations in asthmatic patients, whether they have NERD or aspirin-tolerant asthma. Control strategy comprises a stepwise approach, starting from the use of low dose inhaled ICS, followed by a ICS-LABA combination, and then an add-on therapy with low-dose systemic steroids, tiotropium, anti-IgE (omalizumab), three anti-IL5 antibodies (reslizumab, mepolizumab, and benralizumab), or anti-IL4 receptor alpha antagonist (dupilumab) in severe refractory asthma.61 In addition, as the major pathophysiology of NERD is dysregulation of arachidonic acid metabolism, early introduction of leukotriene modifiers, including CysLT receptor 1 antagonists and 5-lipoxygenase inhibitors, is more preferable in patients with NERD to potentially improve their disease outcomes.6263 However, in a clinical trial, a leukotriene modifier failed to have advantages in treatment efficacy in NERD patients compared to aspirin-tolerant asthmatics.64
Severe asthma is more prevalent in NERD patients than in those with aspirin-tolerant asthma, especially in subtype 1/2 of NERD patients, who have higher blood/sputum eosinophilia and require higher doses of ICS and systemic steroids, resulting in more prevalent use of biologics. Omalizumab, a humanized monoclonal antibody, neutralizes IgE by binding to its high-affinity receptors on the surface of mast cells and basophils. It is approved as an add-on therapy to control patients with severe allergic asthma.6566 Clinical parameters, including the number of asthma exacerbations and hospitalizations, as well as the molecular markers of urinary LTE4 and blood eosinophils, were reduced after treatment of omalizumab.67 There have been several reports on the efficacy omalizumab, especially in NERD patients. A reduced use of steroids and short-acting bronchodilators was noted after 12 months of omalizumab treatment;68 asthma symptom score, number of asthma exacerbations, hospitalization, and urinary LTE4 were significantly reduced.67 A retrospective study of 19 Korean patients with NERD showed reduction in asthma exacerbation, hospitalization, blood eosinophil count, and systemic steroid use after omalizumab treatment. Therefore, the efficacy of omalizumab could also be reproducible in the Asian population.69 So far, there have been no clinical trials on the efficacy of omalizumab use among different NERD subtypes; however, there have been a few cases of patients with NERD subtype 1 who had more favorable responses to omalizumab, with improvement of asthma and urticaria control.7071 Omalizumab can increase the success rate of aspirin desensitization if regular NSAID use is required in cardiovascular or rheumatological conditions. Omalizumab is well tolerated with few adverse effects. Most of the dropouts in previous studies were due to medical costs or non-adherence.72 Large-scale, double-blind, and randomized controlled studies are needed in NERD patients.
Mepolizumab, an anti-IL5 monoclonal antibody, provides an add-on option in eosinophilic asthma refractory to a combination of medium-to-high dose ICS and LABA. IL-5 is essential for survival, proliferation, and maturation of eosinophils.73 Neutralization of circulating IL-5 by mepolizumab reduces blood and sputum eosinophil counts as well as asthma exacerbation in patients with severe eosinophilic asthma.74 A retrospective study of 14 NERD patients receiving mepolizumab showed a significant reduction in absolute eosinophil count and improved asthma control.75 An in vitro study suggested that reslizumab, another anti-IL5 monoclonal antibody, had a higher binding affinity to IL-5 and a greater potency to inhibit IL-5-dependent cells proliferation compared to mepolizumab.76 Dupilumab is known to reduce asthma exacerbations in moderate and severe cases of eosinophilic asthma, and a small-scale randomized controlled study showed improvement in FEV1 in NERD patients after 16 weeks of dupilumab use.77 Further clinical randomized controlled studies are required to determine the efficacy of other type 2 biologics (reslizumab, benralizumab, and dupilumab) in NERD patients.
With increasing importance of epithelial cells interacting with immune cells, epithelial cell-targeting biologics, such as anti-TSLP/IL-33 antibodies, are potential agents for the relief of bronchoconstriction and airway inflammation. A small-scale, double-blind, randomized controlled study illustrated efficacy of anti-TSLP in terms of lung function improvement as well as post-treatment reduction in serum/sputum eosinophil counts,78 although further randomized controlled trials are needed.
To conclude, head-to-head comparisons of treatment efficacies of different biologics among specific NERD phenotypes and endotypes with applying potential biomarkers are necessary in future studies to define the best personalized treatment modality.
Management of NSAID-exacerbated chronic rhinosinusitis and/or nasal polyps
According to the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2012, CRS is subdivided into CRS without nasal polyposis (CRSsNP) and with nasal polyposis (CRSwNP), based on nasal endoscopic findings.79 Initial treatments for both CRSsNP and CRSwNP include regular nasal saline lavage and intranasal corticosteroids. Systemic steroids and prolonged antibiotics can be considered in those with moderate and severe CRS symptoms. For CRSwNP patients, there is a higher level of evidence to support the use of oral corticosteroids.80 Surgical options, including polypectomy, ethmoidectomy, functional endoscopic sinus surgery, and the endoscopic modified Lothrop procedure, are reserved for difficult-to-treat cases. Optimal control of concomitant allergic rhinitis is critical for preventing progression of CRS.81
In NERD patients, occurrence of CRSwNP is attributed to upregulation of type 2 inflammatory pathway, leading to the proliferation and activation of eosinophils and mast cells as well as the release of cytokines, especially IL-5. Eosinophilic inflammation is a common finding in NP tissues of NERD patients; therefore, NERD patients with CRSwNP tend to be more refractory, with higher probability of NP recurrence.82 NERD patients had higher prevalence of CRSwNP, as illustrated by a higher Lund-Mackay NP score of 3–4 in CT.83 Increase in activated eosinophils and Th2 cytokines was found in the nasal polyp tissue of non-eosinophilic CRSsNP patients after a long duration, suggesting a possible endotype spectrum of CRS from non-eosinophilic CRSsNP to eosinophilic CRSsNP, and then eventually to eosinophilic CRSwNP.84 The endoscopic modified Lothrop procedure, together with continual medical treatment for the secondary prevention of NP recurrence, is an optimal treatment for patients with CRSwNP.8586 Leukotriene modifiers did not show additional benefit in the prevention of disease progression in CRSwNP.87 Omalizumab has been shown to be effective in both CRSwNP and CRSsNP patients. There was a significant decrease in dosages of regular steroids and antibiotics in CRS patients with and without NP, although this study did not specifically target NERD patients.88 A small-scale randomized controlled study showed a significant reduction in the total endoscopic NP score in NERD patients who received four injections of omalizumab, and that baseline tissue IgE levels were more correlated with the severity of NP than with serum IgE level in CRSwNP patients.89 Recent data have demonstrated that type 2 biologics, mepolizumab, and dupilumab are useful for secondary prevention of NP, especially in patients with NERD. A meta-analysis illustrated a statistically significant reduction in NP scores of CNSwNP patients using mepolizumab compared to the placebo group.90 However, there are no biomarkers to predict potential responders to mepolizumab before use. Dupilumab reduces both endoscopic and CT scores of NP as well as symptoms, and improved the quality of life in patients with CRSwNP, especially those with concomitant asthma. Serum IgE, thymus, and activation regulated chemokine, and eotaxin-3 were decreased from baseline after dupilumab use; such results imply that they could be potential biomarkers to assess dupilumab response.91
Aspirin desensitization
Aspirin treatment after desensitization (ATAD) is another treatment option for patients suffering from moderate to severe asthma and CRS. The underlying mechanism for aspirin desensitization is not fully understood. Down-regulation of cysteinyl leukotriene receptors, decrease in the production of LTE4, and reduction in airway hyper-responsiveness to LTE4 may be possible pathways,92 while inhibition of IL-4 shows conflicting results and requires further validation.9394
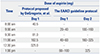
Various protocols for ATAD have been developed, and they are usually the extension of aspirin challenge test.95 Similar to aspirin OPT, expertise and well-equipped tertiary centers are necessary to ensure the safety of ATAD. A modified protocol for aspirin challenge and desensitization was suggested by the EAACI 2019 guideline, consisting of 2 days of ATAD.46 The 1-day ATAD protocol proposed by DeGregorio, et al.45 provides a quick alternative for busy patients. Details and time schedules of the two protocols are shown in Table 1. No matter which protocol has been accomplished, the compliance of aspirin after ATAD is of utmost importance, as aspirin tolerance is lost if aspirin is not taken within 48 hours.
Previous studies have shown convincing results for the efficacy of ATAD in controlling symptoms, deterrence of NP relapse, and reducing the chance of reoperation. According to Berges-Gimeno, et al.,96 87% of NERD patients showed improvement in terms of better symptom control scores, fewer sinusitis, and lower daily dose of systemic steroid. Walters, et al.97 demonstrated persistent benefits of ATAD beyond 10 years of daily aspirin therapy. In clinical practice, however, a significant dropout rate of ATAD has been observed, due to gastrointestinal intolerance or need for elective surgery. Patient education and prescription of proton pump inhibitors may improve drug compliance.
NECD
Patients with NECD suffer from exacerbation of urticaria or angioedema, and even anaphylaxis, immediately after NSAID ingestion. The exacerbation becomes more severe when patients have a suboptimal control of chronic urticaria, or are exposed to high doses of NSAID. As a result, NSAID avoidance, along with optimal control of chronic urticaria, is essential. Chronic urticaria should be managed according to the EAACI/GA2LEN/EDF/WAO 2017 guideline,19 which starts with the regular use of standard dose of second generation H1-antihistamines, followed by a top-up of 4-fold dose of antihistamines when the standard dose fails. Omalizumab is reserved for patients who are not responsive to antihistamines. It prevents urticaria exacerbation, and thus leads to a better quality of life in patients with severe uncontrolled chronic urticaria.98 An emergency kit with adrenaline auto-injector should be given to patients with prior anaphylaxis to NSAID.99
NIUA, SNIUAA, and delayed NSAID hypersensitivity reactions
In NIUA and SNIUAA, patients develop urticaria only after intake of NSAID. Culprit NSAID avoidance is enough to prevent exacerbation. Acute urticaria exacerbation can be controlled by a short-term use of antihistamines with or without steroids.
In delayed NSAID hypersensitivity reactions, NSAID avoidance can prevent the recurrence of skin manifestations. Desensitization should be considered only when the use of aspirin is irreplaceable (e.g., acute myocardial infarction) and the delayed hypersensitivity reaction is mild (e.g., uncomplicated exanthems and fixed drug eruptions).100
CONCLUSION
Advances in diagnostic tests as well as the development of new pharmacological and surgical interventions provide an optimistic outlook for better management of NSAID hypersensitivity reactions. Identification of phenotypes and endotypes of NSAID hypersensitivity allows for management on an individual basis. Further studies are needed to establish the relationship between sub-classification of NSAID hypersensitivity reactions and novel in vitro biomarkers.



 XML Download
XML Download