

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Incidence and Outbreaks in Korea
1. 1945 – 1959: A disease that can ruin a country
The liberation from Japanese occupation in 1945 was a momentous event, but the political chaos and Korean War that followed brought substantial hardship to the lives of Koreans, especially in the area of healthcare. Tuberculosis (TB), which had already been recognized as a major infectious disease from the late Joseon dynasty through the Japanese colonial period, spread rapidly because of poor living conditions, low healthcare accessibility, lack of diagnostic and treatment technologies, and lack of proper management systems. Although the exact incidence of TB during this period is unknown owing to the lack of systematic surveys, rough estimates can be made through small-scale surveys and records from that time. In April 1946, the United States Army Military Government in Korea restructured the Health and Welfare Department to establish plans for disease prevention and welfare programs. Among these programs, the development of the National Tuberculosis Hospital in Masan city was selected as the top priority. An article that reported on this program stated that its goal was to “prevent TB and infectious diseases that are rapidly spreading after the war,” [1] which indicates that TB was one of the most prevalent infectious diseases during that time. A media report in 1948 cited health authorities reporting that up to 400,000 people were infected with TB, representing a two-fold increase compared to figures before the liberation [2]. In the same year, the Seoul Health and Welfare Department conducted tuberculin skin tests among approximately 100,000 students from roughly 70 primary schools in Seoul; approximately 47% tested positive and the positivity rate among children aged 16 years was 62% [3].
“Tubercle bacilli, which cause a disease that can ruin a nation, dwell in the bodies of young citizens who bear paramount responsibilities and the promise of great achievements for a new nation, and yet do administrators and parents not recognize the severity of this issue? If that is the case, it is a very dangerous situation. The disease will most definitely affect these children in the future when they become tired from work or do not consume enough nutrients in their daily lives.”
- Lee KH. Foremost Mission for Nation's Public Health: Proper Nutrition and Physical Fitness (國民保健의第一課題 榮養攝取와體力向上). Kyunghyang Shinmun, September 19, 1948.
During the 6-month period from November 1948 to April 1949, tuberculin skin tests were conducted among 119,609 people living in group facilities, such as factories, schools, mines, and prisons. The results showed a very high positivity rate of 69% among people aged 15–20 years and 80 – 92% among people aged >20 years. Among 23,345 people who underwent chest X-ray imaging, the proportion of patients with active TB was 6.08%. Based on these records, the number of patients with active TB in Korea at the time was estimated to be approximately 120,000 [4]. The high prevalence of TB and lack of healthcare resources inevitably led to a high TB-associated mortality rate, with an estimated 50,000 people dying each year because of TB during this period (equivalent to 250 per 100,000 population) [5]. Whenever lung disease was mentioned during that period, it commonly referred to TB. Moreover, TB was referred to as a disease that could ruin a country and there were certainly enough reasons justifying this.
The Korean War added fuel to an already volatile situation. Considering the poor nutritional status of individuals, group living because of mass evacuation, and poor access to healthcare, such an increase in the infection rate and prevalence of TB would be expected. Due to weakened government function during this period, there is little epidemiological data available. However, considering that an article had reported that approximately 25% of patients who required medical treatment in refugee camps had pulmonary TB (PTB), it is clear that there was an increasing trend in the number of TB patients [6]. In addition, the TB-associated mortality rate also increased significantly, with 10,000 PTB patients dying each month in 1954, equivalent to roughly 300 patients per day [7]. According to an estimate for the same year, among 20 million Koreans, 1.3 million had active TB, and the TB-associated mortality rate had reached 300 – 400 per 100,000 population [8]. However, the number of people who received inpatient treatment at government-operated medical institutions was about 2,000, while the number of outpatients receiving treatment amounted to only 30,000.
To accurately assess the disease burden of TB in Korea, the first National Tuberculosis Prevalence Survey was conducted over a 3-year period, starting from 1957. In this survey, the prevalence of TB (including latent TB infection) was 72% among individuals of all ages and the prevalence of active PTB based on chest X-ray imaging was 4.4% [9]. Although this survey was limited, it was significant in that it provided nationwide data on the prevalence of TB.
2. 1960 – 1999: National Tuberculosis Prevalence Survey
In 1965, a National Tuberculosis Prevalence Survey that included sputum stain examination for mycobacteria was conducted; since then, the survey was repeated every five years until 1995 (Table 1). It became possible to use the survey results to obtain major TB-related indicators via a systematic and consistent method, which enabled observation of temporal changes in the disease burden of TB and effective assessment of TB control policies. Indicators that are important for understanding the epidemiology of TB include the prevalence of TB infection (including latent TB infection), the prevalence of smear-positive PTB, and annual risk of infection (annual infection rate). The prevalence refers to the proportion of people infected with TB at a certain time point, which is typically measured by the positivity rate observed with the tuberculin skin test among different age groups. Therefore, it does not only refer to active TB that can be transmitted, but also includes latent TB infection in which Mycobacterium tuberculosis (MTB) is dormant in the body and has not yet triggered the disease. The prevalence of smear-positive PTB refers to the proportion of patients within a population group who have smear-positive PTB confirmed by sputum microscopy. It represents the proportion of people with confirmed presence of MTB in the sputum among those within the survey population who underwent a sputum test after abnormal findings on chest X-ray imaging. The annual risk of infection represents the proportion of people newly infected or re-infected with TB over a 1-year period. This is calculated on the basis of the prevalence among children aged 5–9 years in Korea.
Table 1
National Tuberculosis Prevalence Survey results

The results from the survey conducted in 1965 revealed that the TB prevalence among those aged <30 years was 44.5% and the annual risk of infection was 5.3%. This indicated that approximately half of the young people in Korea were infected with TB and 5.3% were newly infected with TB each year. Owing to the effects of various TB control policies, which will be discussed later, the prevalence increased slightly to 46.9% in 1970 and 1975, but steadily decreased thereafter to 15.5% in 1995. The risk of infection also continued to decrease with each survey, going down to 0.5% in the final survey in 1995.
As the prevalence of TB decreased, the prevalence of active PTB also decreased steadily. The proportion of patients showing findings of active TB on chest X-ray imaging, the number of PTB patients with positive culture findings, and the number of PTB patients with positive smear findings who had higher infectivity all decreased steadily over 30 years, resulting in a 5- to 7-fold decrease. However, the prevalence of active TB is highly dependent on the duration of the disease; thus, even if the incidence remains constant, the prevalence of active TB may appear higher when the duration of the disease is longer. Owing to advances in the treatment of TB, the duration of the disease has been shortened to 1/4th of that observed 40 years earlier. Thus, as it is difficult to assume that the incidence has decreased to a similar extent as the prevalence has, attention should be paid to the change in the incidence of TB [9].
As TB often shows slow progression, it is very difficult to investigate its incidence. When the number of people who developed active PTB within a year of being determined as healthy in the 1970 National Tuberculosis Prevalence Survey was investigated, the annual incidence was estimated to be 410 per 100,000 population; however, this study was limited by a small sample size [10]. Another large-scale study used data from biennial civil servant health checkups to assess the incidence among 800,000 people for two sets of years. The results showed that the annual incidence per 100,000 population for active PTB on X-ray imaging, positive culture, and positive smear was 393, 84, and 53, respectively, for 1988 – 1990 [11], and 202, 81, and 54, respectively, for 1992 – 1994, showing no distinct changes between the two surveys [12]. The World Health Organization (WHO) estimated the incidence in Korea to be 108 and 80 per 100,000 population in 2012 and 2016, respectively [13]. Since 2000, an internet-based surveillance system has been operated to strengthen the surveillance of notifiable infectious diseases, which has enabled the prediction of trends in TB incidence based on changes in the number of new TB cases reported.
3. Since 2000
With a continued decrease in the prevalence of TB, the sample size required to obtain meaningful data increased. Accordingly, the National Tuberculosis Prevalence Survey was discontinued from 2000. Other surveys using different methods have since been conducted in its place, the results of which could be used to determine the recent prevalence of TB. Among recent large-scale surveys, a survey of 2,051 members of selected households within the sample population of the 2016 Korea National Health and Nutrition Examination Survey showed a TB prevalence of 33.2% [14]. With regard to age groups, the prevalence was 6.5%, 10.9%, 36.4%, 46.1%, 48.7%, and 45.0% among those aged 10 – 19, 20 – 29, 30 – 39, 40 – 49, 50 – 59, and 60 – 69 years, respectively. In place of the National Tuberculosis Prevalence Survey that was conducted periodically, changes in the epidemiology of TB could now be identified through the internet-based reporting and surveillance system operated by the Korea Centers for Disease Control and Prevention (KCDC) as this strengthened the reporting of notifiable infectious diseases (Fig. 1).
Figure 1
Age-standardized distribution of the proportion of tuberculosis patients reported by year (relative to the population in 2005).
Source: Korea Centers for Disease Control and Prevention. 2016 Annual Report on Notified Tuberculosis in Korea.
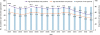
In 2001, the total number of TB patients was 46,082 (96.3 per 100,000 population), of which the number of new patients was 34,123 (71.3 per 100,000 population). In 2016, the number of total and new TB patients was 39,245 (76.8 per 100,000 population) and 30,892 (60.4 per 100,000 population), respectively, showing decreases of 20.2% and 15.3% in the prevalence and incidence, respectively, over those 15 years. The proportion of new patients increased from 73.5% to 79.5% and the number of people being re-treated decreased to approximately half. The increase in the proportion of new patients and the decrease in the number of people being re-treated could be viewed as a positive change as it implies that discontinuation or failure of treatment decreased because of improved TB treatment and care. With respect to age groups, the incidence among those aged 10–19 years was more than 2-fold lower than that among those aged ≥60 years, which indicates that the risk of infection had reduced. However, there was a small peak in the rate of new patients among those in their late 20s, indicating that the spread of TB is continuing (Fig. 2).
Figure 2
Distribution of new tuberculosis patients by sex/age.
Source: Korea Centers for Disease Control and Prevention. 2016 Annual Report on Notified Tuberculosis in Korea.

Regarding institutions reporting TB cases, in 2001, 46.1% of cases were reported by public health centers and 53.9% were reported by private healthcare institutions. In 2016, however, the proportion of cases reported by public health centers decreased significantly, with the majority of cases (92.2%) being reported by private healthcare institutions. This demonstrates that the reporting rates in private healthcare institutions have improved, and the role of these private healthcare institutions in TB treatment has increased as well. The number of new patients who were foreigners residing in Korea also increased steadily each year, from 126 in 2001 to 2,136 in 2016. While it is difficult to claim that the incidence among foreigners is higher than that among Korean nationals, there is an increasing inflow of people from countries with a high prevalence of TB and foreigners may show low diagnosis rates because of low accessibility to healthcare. Thus, greater effort is needed for TB control among foreigners. Considering the incidence of TB cases up to 2012, there was a pattern of a slight increase followed by plateauing at close to 70 per 100,000 population. The reason for the plateau in the incidence could be the decrease in the number of actual new patients and an increase in reporting. The number of patients who received TB-related insurance benefits from the National Health Insurance Service continued to decrease from 169,938 in 2004 to 83,149 in 2015, supporting this hypothesis [15]. Moreover, during the 4-year period after 2013, the number of new patients decreased steadily to 60.4 per 100,000 population in 2016, which also suggests a continued decrease in the incidence of TB.
Disease Characteristics in Korea
1. Diagnosis of TB
For the radiographic diagnosis of TB, mass screening via miniature chest radiograph was carried out for the first time in Korea in 1942. After liberation from Japanese occupation, mass screenings were carried out mostly in schools or large businesses. In particular, a large-scale mass screening, covering approximately 70,000 high school and university students from 300 schools throughout Korea, took place in 1953. Mass screening programs went into full gear after the war; however, because of a lack of mobile screening vehicles, X-ray imaging equipment and generators donated by other countries were hauled in delivery trucks and oxcarts to perform the required screening. Starting from the late 1950s, screening vehicles with X-ray imaging equipment loaded on buses manufactured in Korea were introduced. Regarding the X-ray imaging equipment, 35-mm cameras were used initially, but starting from 1960, 70-mm cameras with lower radiation exposure were introduced. With respect to medical institutions, a total of 1,458 institutions, including 980 private clinics and 189 public health centers, had X-ray imaging equipment available in 1969. As access to X-ray imaging devices was limited, TB was diagnosed by sputum tests in many areas. Subsequently, X-ray imaging equipment became more widely available, and the introduction of computed tomography scans began in the late 1970s.
For the bacteriological diagnosis of TB, the National Central Tuberculosis Center established in 1954 functioned as a testing facility, and testing was subsequently transferred to the Korean National Tuberculosis Association in 1958. For the management of TB patients registered with public health centers, a technical training program for effective performance of sputum tests at public health centers was started in 1962, and this was the first government-led microbiological testing program. Based on such effort, microbiological laboratories for MTB were set up in all cities and provinces in 1964, and subsequently, a system was established in which smear tests were performed in laboratories at public health centers and cultures were performed in city or provincial laboratories or sent to the central laboratory. In addition to training of testing personnel and equipment support for quality control, the Central Tuberculosis Laboratory re-evaluated smear slides examined by public health centers, while also manufacturing and supplying test agents. Subsequently, fluorescence microscopy was used for smear tests and an automated culture system was developed, enabling private healthcare institutions and commercial laboratories to perform mycobacterial cultures in-house. With the introduction of the polymerase chain reaction in the early 1990s and rapid susceptibility test in the mid-2000s, the time required for diagnosis and confirmation of susceptibility was shortened significantly.
2. Treatment of TB
Before effective drug therapy for MTB was developed, most PTB patients were isolated in sanatoriums located in areas with clean air. In some cases, surgical interventions, such as artificial pneumothorax, artificial pneumoperitoneum, or thoracoplasty were performed. In Korea, public and private TB hospitals, including Masan National Tuberculosis Hospital, began providing care and surgical treatment for TB after liberation from Japanese occupation. However, such methods had limited efficacy and were difficult to use universally.
Streptomycin (STR), the first drug effective against MTB, was developed in 1944. It was introduced to Korea in the late 1940s through foreign aid and was used to treat TB patients on a limited basis. Isonicotinic acid hydrazide (isoniazid, INH) was developed in 1952 and was imported to Korea from the following year onwards. The introduction of new drugs for TB was reported several times in newspapers and was even advertised; hence, it appears that it gained much attention from the general public. In 1951, Masan National Tuberculosis Hospital received an allotment of 40 bottles of STR from the government, and starting from 1953, it received STR, INH, and para-aminosalicylic acid (PAS) as relief medicine and freely prescribed them [8]. After the Korean War Armistice, in addition to those donated in humanitarian aid packages, anti-TB drugs began to be imported through official channels. In the late 1950s and 1960s, pyrazinamide (PZA) and ethambutol (ETB) were developed and introduced for widespread use. The standard treatment for TB at the time involved administration of INH, STR, and PAS or ETB in the early intensive care period and administration of INH and PAS or ETB in the follow-up maintenance period lasting 18 – 24 months. Although this treatment approach was effective, the duration of treatment was long, and the drugs had many adverse effects, which resulted in high treatment failure rates because of treatment discontinuation or irregular drug administration. In 1967, the use of rifampicin (RIF) was started, and this revolutionized the treatment of TB. Short-course therapy that included RIF spanned only 9 months; thus, the development of RIF shortened the duration of treatment by more than half as compared to the previous standard therapy. Such short-course therapy increased the treatment success rate, as fewer people dropped out during the treatment period, which also contributed significantly toward improving TB control. When RIF was introduced in Korea for the first time, it was mostly used for re-treatment of patients in whom initial treatment had failed. Song et al. reported on the outcomes of RIF use in initial treatments in 1972, and a clinical trial in Africa reported the successful outcome of short-course therapy. As a result, the full use of RIF in Korea began from 1980 following discussions about its use in short-course therapy since 1977 [16].
One significant change brought on by advances in TB treatment is the decrease in the TB-associated mortality rate. During the 1950s, TB was the most common cause of death, but the TB-associated mortality rate had decreased to 22.3 per 100,000 population by 1981 [17] and to 19.7 per 100,000 population by 1983, making it the sixth most common cause of death. The TB-associated mortality rate continued to decrease to 9.9 per 100,000 population by 1990 and 4.8 per 100,000 population by 2007, with similar levels being maintained since. Although the TB-associated mortality rate was no longer a useful indicator because of the introduction of effective treatment, the annual number of deaths associated with TB was still 2,209 in 2015 [18].
Due to advancements in TB treatment and improvement in TB control, resistance to anti-TB drugs also decreased gradually. In the National Tuberculosis Prevalence Survey conducted in 1965, the proportion of patients infected with MTB showing some drug resistance at the first treatment (initial drug resistance) was 26.2%, while the resistance rate during treatment or recurrence (acquired drug resistance) was 55.2%. The drug resistance rate reached a peak in 1980 (initial drug resistance rate, 30.6%; acquired drug resistance rate, 75.4%), but gradually decreased thereafter to reach a rate of only 5.8% in the final survey conducted in 1995. However, multidrug-resistant TB (MDR-TB) with resistance to both INH and RIF, which are key drugs in the treatment of TB, emerged as an important threat. According to TB notification statistics, the annual number of reported MDR-TB patients has been 800 – 1,200 since 2011, with extensively drug-resistant TB cases being reported at a rate of over 50 per year. According to data from the Korean Institute of Tuberculosis, which has been conducting a large proportion of drug resistance tests in Korea, the multidrug resistance rate among new patients was 1.9 – 2.9% [19]. Thus, special attention is needed for MDR-TB patients because they show lower treatment efficacy, require longer treatment periods, and often become chronic carriers of MTB.
Tuberculosis Control in Korea
1. 1945 – 1960
As government function was transferred from Japan to the US Army Military Government in Korea after the liberation, major changes in health administration also took place. During the Japanese colonial era, health policies were implemented by the sanitary police and showed strong military characteristics. Their main focus was on preventing the outbreak of acute infectious diseases that could cause a decline in productivity, rather than truly improving the quality of life of the population. On September 24th, 1945, the US Army Military Government declared “Establishment of Sanitary Bureau” as Ordinance No. 1, whereby the Sanitary Division within the Police Bureau was disbanded, and an independent Sanitary Bureau was established. The Sanitary Bureau was renamed as the Health and Welfare Bureau in October of the same year and became the Ministry of Health and Welfare in March 1946. The Ministry of Health and Welfare took over a facility the Japanese had used as a sanitarium for disabled veterans, and the facility was renovated and reopened as the Masan National Tuberculosis Hospital on June 1, 1946 [20]. Dr. In-Sung Kwak from Severance Medical School was appointed the first director and Dr. Roy K. Smith, an American doctor, was appointed as an advisor. Subsequently, the hospital began performing various procedures, such as interventions for phrenic nerve paralysis, pleural adhesiolysis, and artificial pneumoperitoneum. Subsequently, the Incheon Red Cross Sanitorium opened in 1948 and the Transportation Ministry's Sanatorium in Masan opened in 1949. In Masan in particular, various TB hospitals/centers - including the 36th Army Hospital, National New Tuberculosis Sanitorium, and the TB ward at Jinhae Naval Hospital - came together to provide treatment with antibiotics and surgical interventions.
In early 1948, the Ministry of Health and Welfare decided to conduct the tuberculin skin test among primary school students and conducted the first round of tests among 3,000 students from Maedong Elementary School. In addition, the Ministry of Transportation conducted screening among workers of factories located in the Yongsan industrial zone, found that 5% of the people screened had TB, and advised those who required treatment to take a leave of absence. Furthermore, newspaper articles also reported that Gyeonggi-do Health Department conducted TB screening in group institutions, such as factories and schools, which indicated that workplace screening targeting large businesses was also conducted [21]. In the following year, the Health Bureau allocated a budget of 21.54 million won and planned to perform chest X-ray imaging among students, factory workers, and farmers in an effort to diagnose TB patients and assess the nationwide prevalence of TB [22]. In February 1950, the WHO and the United Nations Children's Fund (UNICEF) committed $900,000 to support public health projects in Korea and dispatched a delegation to Korea for 1 year. Of the amount committed, it was planned that 1/3rd would be used for TB-related programs. In March of the same year, Bacillus Calmette–Guérin (BCG) cultured by the National Institute of Health and Masan National Tuberculosis Hospital was to be used to vaccinate children and adolescents. However, because of the Korean War that followed, such efforts were faced with many difficulties.
As mentioned in the chapter on disease characteristics in Korea, TB became an even bigger problem during the Korean War, and implementation of healthcare policies also became very difficult. Despite this, group vaccinations with BCG for students and civil servants were carried out from 1952 onwards, which suggests that even in the chaos of war, healthcare programs for TB were a relatively high priority. Medical technologies from advanced countries, such as the US, were introduced to Korea during the war. This led to advances in the treatment of TB and a full-fledged framework for TB control was established after the war. A key event in relation to this was the founding of the Korean National Tuberculosis Association. Four existing entities (Joseon Tuberculosis Prevention Association, Korean Tuberculosis Association, Christian Medical Association, and Tuberculosis Prevention Committee of the Health Ministry) came together to form a single entity in order to make efforts towards eradicating TB, and as a result, the Korean National Tuberculosis Association was founded in November 1953. In September of the following year, Korea became a regular member at the Fifth International Union Against Tuberculosis.
With respect to TB awareness campaigns that target the general public, the first thing that comes to mind is the Christmas seal. The first Christmas seal in Korea was issued in 1932 by Dr. Sherwood Hall, a Canadian doctor who was a pioneer in the anti-TB movement in Korea. After liberation from Japanese occupation, the Korean National Tuberculosis Association issued these seals starting 1953 onwards, and on December 1, it held the first TB Prevention Week in conjunction with the Ministry of Health. Subsequently, the Christmas seals were issued every year; not only did this provide financial support for TB eradication programs, but the seal also became a symbol of the anti-TB movement.
In 1954, the Ministry of Health established a 5-year plan for TB control in response to the problem that worsened because of the Korean War. Major programs included dissemination of TB-related knowledge, training of specialists, BCG vaccination, and establishment of outpatient treatment services. In August of the same year, the National Central Tuberculosis Center was established to provide technical support for TB control. Moreover, chest clinics, sponsored by the Church World Service and led by Dr. E. B. Struthers, a Canadian doctor, were established within various hospitals throughout Korea, providing free outpatient treatment to TB patients. Owing to the success of these clinics, the Ministry of Health expanded the outpatient treatment of TB patients to public healthcare centers throughout Korea in April 1955. Through such efforts, TB treatment in Korea transitioned from sanitoriums to outpatient clinics.
The identification of undiagnosed TB patients is just as important as successfully treating TB patients. Starting from 1954, the National Central Tuberculosis Center used five X-ray imaging machines to conduct screening in schools. Starting from 1956, the Korean National Tuberculosis Association conducted group X-ray imaging screenings with foreign aid. Subsequently, X-ray imaging screenings were expanded to target not only schools, but also the general public, whereby 100,000 to 200,000 people were screened every year.
2. 1960 – 1999
Along with revolutionary changes in national healthcare policies, major advances in TB control took place during the 1960s. In 1961, the Public Health Center Act was enacted, and starting from the following year, TB control programs, such as BCG vaccination and registration and treatment of TB patients, were handled through public health centers. For this, TB control personnel were assigned to 182 public health centers throughout Korea starting from 1963, and in 1964, microbiologic laboratories for TB diagnosis were established in 9 cities and provinces. By the end of 1964, over 100,000 TB patients were registered with public health centers, and as a result, public health centers took the lead in TB control. Moreover, existing TB sanitoriums were expanded to become TB hospitals, and new medical institutions specializing in TB were also established. According to the Health and Social Affairs Statistical Yearbook, such efforts led to an increase in the number of hospital beds for TB patients - from 1,537 beds in 1962 to 2,501 beds in 1970. In 1966, to address the improper prescription of anti-TB drugs by private healthcare institutions, guidelines for PTB chemotherapy were prepared and published in the journal “Tuberculosis and Respiratory Diseases” and were distributed to private clinics.
In January 1967, the Tuberculosis Prevention Act was announced and enacted. This act contained a total of 45 articles that regulated regular health screening for businesses and schools, temporary health screening for those who come in contact with TB patients, BCG vaccination, obligation of medical personnel to report TB patients, hospitalization orders, and responsibilities of the government. Consequently, enforcement decrees and rules were enacted, and the Division of TB Control was newly established within the Health Bureau of the Ministry of Health and Social Affairs. The Tuberculosis Prevention Act has been amended 14 times and is still effective today. In addition, a TB specialist certification was implemented in 1969 for the training of doctors specializing in the treatment of TB.
Collection of basic epidemiological data, such as TB infection rate, prevalence, and number of patients with positive smear findings, is needed foremost for TB control. In this regard, the Korean National Tuberculosis Association conducted the National Tuberculosis Prevalence Survey for the first time in 1965 with support from the WHO and UNICEF. Through this survey, reliable data on the epidemiology of TB in Korea were obtained for the first time. The National Tuberculosis Prevalence Survey was conducted every five years but was discontinued in 1995 because of a decrease in the prevalence of TB, with the reporting and surveillance system operated by the KCDC performing its role instead.
Another key strategy for infectious disease control is vaccination. The BCG vaccine, which was produced by Albert Calmette and Camille Guérin from France by sub-culturing Mycobacterium bovis 239 times, is an important vaccine that helps in reducing the risk of latent and active TB, as well as the risk of severe TB, such as tuberculous meningitis. Accordingly, the Korean government placed a high priority on BCG vaccination programs early on and began producing BCG in Korea. Initially, infants were vaccinated before the age of 1 year, but the vaccination program was expanded to include children up to the age of 5 years if they did not have a vaccination scar, while first graders who tested negative for the tuberculin skin test were also vaccinated [23]. Starting from 1973, tuberculin skin tests were performed among sixth graders and those who tested negative were re-vaccinated with BCG. However, based on the recommendation of the WHO to discontinue the practice of re-vaccination with BCG, this practice was discontinued in 1997. Through such efforts, the BCG vaccination rate among children under 4 years of age increased drastically from 6.1% in 1965 to 85.0% in 1995 [24].
TB control policies, the framework for which was established during the 1960s, were gradually expanded and upgraded during 1970 – 1989, and included TB patient registration and treatment through public health centers, mass screening, BCG vaccination, and regular surveys. In particular, a standard regimen was formulated, focusing on public health centers, to enhance therapeutic efficacy and prevent drug resistance, and programs for improving the appropriateness of prescriptions were also implemented. During the 1960s, ideal anti-TB drug therapy could not be administered because of the lack of medical supplies and government budget constraints. Moreover, the standard regimen - such as the use of thioacetazone, which has many adverse effects, or the use of semi-weekly intermittent therapy - changed frequently. In 1973, TB treatment guidelines were distributed to public health centers throughout Korea, whereby the standard regimen was established as mentioned in the previous chapter. Along with this, the late 1970s saw the start of re-treatment programs for patients who had previously experienced failed TB treatment. In addition, domestic production of anti-TB drugs, expansion of public and private TB hospitals, and expansion of medical insurance coverage also took place.
3. Since 2000
In 1999, the Korean government established the “Comprehensive Plan for Healthcare Development in the 21st Century” and selected TB as one of five major diseases targeted for focused management, while also setting goals to be achieved by 2010. One of the goals set at the time was to reduce the incidence of PTB to 60 per 100,000 population by 2010.
Until the 1970s, most TB patients were treated at public health centers. However, with expansion of medical insurance coverage for all Korean citizens in 1989, the number of patients being treated at private healthcare institutions increased owing to improved access to such institutions. Starting from 2000, TB case reporting was computerized, thereby establishing a system that allowed management of patients being treated at private healthcare institutions. However, unlike public health centers that had dedicated themselves to TB control for a long time, private healthcare institutions could not systematically manage TB patients, which resulted in a lower cure and a higher treatment drop-out rate [25]. With respect to treatment, as of 2005, only 80% of new patients being treated at private healthcare institutions were being prescribed the standard regimen [26]. Thus, to overcome such limitations, the need for a private-public mix (PPM) in which the government would dispatch personnel to private healthcare institutions to support patient management, such as management of compliance and prevention of drop-out during treatment, emerged. In 2007, the KCDC implemented a pilot program that provided dedicated nurses to support university and general hospitals, and starting from 2009, the program was fully implemented. As of 2016, 193 dedicated TB control nurses had been dispatched to 120 medical institutions and were managing 63.5% of all new TB patients.
One of the key policies for eradicating TB is identifying people who have come in close contact with patients with active TB in order to prevent those people from becoming infected or providing early treatment to those who become infected. From 1995 onwards, public health centers have performed tuberculin skin tests on children younger than 6 years who have family members newly diagnosed with TB to provide treatment for latent TB infection, but such efforts have not been very active. To improve the investigation of close contact, contact investigation programs in group facility settings were started in 2005 and were expanded to close contacts of all TB patients in 2011. In addition, treatment for people with latent TB infection, which could advance to active TB in the future, has been strengthened. This is because medical insurance coverage for contacts of TB patients, people infected with human immunodeficiency virus, and children younger than 5 years was started in 2012 and was subsequently expanded to all Korean citizens by 2015. Furthermore, the Tuberculosis Prevention Act and the enforcement decrees were amended in 2016, making TB and latent TB screening mandatory for workers in group facilities, such as medical institutions and schools.
In March 2016, the Korean government announced the “Second National TB Control Plan,” the goal of which was to reduce the incidence of TB to less than 12 per 100,000 population by 2025. For this, TB control policies that focused on early diagnosis and appropriate treatment of patients with active TB were converted to policies that preemptively control TB before onset. Thus, latent TB infection screening and treatment were expanded as implementation strategies, setting plans to provide the necessary human, financial, and institutional support.
Owing to improved living standards, advances in diagnostic and treatment techniques, and governmental and social efforts to control TB, TB incidence has steadily decreased in Korea over the past 70 years. Moving forward, the incidence of TB is expected to continue to decrease owing to improved diagnosis and treatment, treatment of latent TB infection, survey of contacts, and PPM programs. Despite this, the prevalence of TB in Korea is still relatively higher than that in other countries with similar economic power, with Korea being ranked first among all Organisation for Economic Co-operation and Development countries. Moreover, with population aging, the incidence of active TB may increase among older individuals, who may have been infected with TB in the past. Additionally, efforts are needed for high-risk groups, such as the low-income group, foreigners residing in Korea, and North Korean defectors. As the prevalence of latent TB infection among younger people has decreased, mass outbreaks in schools or hospitals could increase. Mass outbreaks in such groups could have a significant social impact, and thus, active control measures are necessary. The WHO is running an “End TB Campaign” to eradicate TB around the world, with the goal of reducing its incidence by 90% to 10 per 100,000 population by 2035. Continued efforts are also needed in Korea to eradicate TB, which still presents a major disease burden.
 XML Download
XML Download