

 PDF
PDF ePub
ePub Citation
Citation Print
Print



1. Cholera Outbreaks and Epidemics
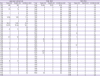
In Korea, cholera outbreaks usually begin following the introduction of cholera from other countries. The first cholera epidemic after the country's liberation occurred in 1946. From 1821 to 1946, there were 28 classical cholera epidemics. From 1946 to 2016, there were 11 cholera epidemics caused by El Tor strains (Table 1).
Table 1
Number of cholera reports by year (cases/deaths/incidence rate)
The cholera outbreak that occurred in 1946 had three distinct characteristics: (1) It was the last classical cholera outbreak that occurred in Korea; (2) It broke out at a time of major social upheaval following the country's liberation from Japan; and (3) It occurred immediately after the discontinuation of the Japanese health administration system, before the United States Army Military Government (USAMGIK) public health system was established.
1) Cholera epidemics during the late Joseon dynasty period and Japanese colonial rule
The first recorded cholera epidemic in Korea, which occurred in 1821, was introduced from trade with China [1]. There were more than 10 subsequent epidemics between 1821 and 1910, when Japanese colonial rule began [2]. As the country opened to the rest of the world, the concept of cholera, which used to be regarded as an infectious folk illness, has become more scientific. From the opening of the country in 1876 to the start of colonization in 1910, infection control programs were implemented as directed by the Japanese government [3].
There were several subsequent cholera outbreaks during the period of Japanese colonial rule. The incidence of cholera peaked in 1919 and 1920 in the aftermath of the Independence Movement Day (March 1st) [4]. During the period of Japanese colonial rule, the incidence of cholera and cholera-related deaths decreased as a result of quarantine procedures [5]. However, given that the incidence of other infectious diseases did not decline or increased, public health projects under Japanese colonial rule were largely ineffective [6].
2) The 1946 classical cholera epidemic
Two million out of 5 million Koreans living overseas returned to the country after it was liberated from Japan. As many people migrated to large cities, hygiene deteriorated greatly. The USAMGIK restructured the Korean Governor-General's administration and established the Ministry of Health and Welfare. After the discontinuation of the Japanese health administration system, the Ministry of Health and Welfare established by the USAMGIK did not function very well due to a lack of human resources. Various infectious diseases epidemics broke out under the circumstances of the unclear roles of the police in containing infectious diseases outbreaks [7].
In May 1946, cholera was introduced to the country by a ship returning from Guangdong, China. An epidemic started in Busan, then soon spread nationwide. There were 15,644 cases of cholera, and 10,181 cholera-related deaths [8]. People with cholera experienced severe dehydration as a result of profuse vomiting and diarrhea, and it was difficult to obtain sufficient fluids, which were essential for treatment.
The following passage describes the situation at that time [9]:
The USAMGIK's poor infection control policy made it impossible to stop the epidemic from spreading. The US Army threw bodies into the sea near Yeongdo, which resulted in the spread of cholera to nearby villages. Many skirmishes occurred in Busan amid worsening public sentiment. Soldiers annihilated an entire village because the villagers had hidden a person with cholera in a wardrobe, and they destroyed a crematorium because of the smoke that it produced. In addition, they pointed a gun at a driver who refused to move bodies.
3) El Tor cholera epidemics
In the 1960s, El Tor cholera replaced classical cholera. El Tor became established during the 7th pandemic of cholera, which began in Sulawesi, Indonesia. El Tor cholera [10] is characterized by lower volumes of and less frequent diarrhea, a lower case fatality rate, and a higher percentage of people who carry cholera without symptoms.
There were 11 cholera epidemics in Korea between 1963 and 2001 [11]. They generally occurred in summer and fall from August to October, and they may have been associated with environmental factors such as seawater temperature. The duration of the epidemics ranged from 11 days in 1999 to 77 days in in 1970 [12]. Most of the epidemics began in coastal areas or ports such as Incheon, Busan, Gunsan, Masan, and Sinan (Table 2) [11].
Table 2
The epidemic year, epidemic period, initial outbreak area, and major epidemic areas of El Tor cholera epidemics in Korea from 1963 to 2001

(1) The 1963 cholera epidemic
The first case of El Tor cholera occurred in a day laborer in September 1963. This cholera epidemic spread to coastal areas in South and North Gyeongsang Provinces and Gangwon Province. No source of infection was identified. There were cases of cholera in neighboring countries, including China, Japan, Taiwan, Hong Kong, and Macau [13].
(2) The 1969 cholera epidemic
The 1969 cholera epidemic began in Okgu-gun, North Jeolla Province in August 1969 and spread across the country [13]. Early in the epidemic, there was confusion about the cause. It was initially managed as food poisoning, then diagnosed as intestinal Vibrio infection, and subsequently confirmed to be El Tor cholera. Epidemiological investigations did not make much progress [14]. Epidemiologically and clinically, this outbreak showed differences to El Tor cholera, and various other intestinal pathogens were identified among patients quarantined in the clinic. Furthermore, considering that the route of infection into Korea was unclear and that there were multiple sources of the epidemic, some researchers in Korea suspected that pathogens may have been spread intentionally [13]. After Dr. Yen from the World Health Organization (WHO) Western Pacific Region visited the country and to investigate the outbreak, it was concluded that there was no clear evidence to suggest that the 1970 cholera in Korea was caused by pathogens that had been intentionally spread [15].
(3) The 1980 cholera epidemic
In September 1980, there was an outbreak of diarrhea among a group of mourners who had visited a funeral parlor in Du-ri, Anjwa-myeon, Sinan-gun, in South Jeolla Province. This outbreak was followed by a nationwide epidemic. Epidemiological investigations were delayed, which made it difficult to ensure the accuracy of the results. During the outbreak investigation and disease prevention process, disinterest and fear among local residents, which were attributable to previous indiscriminate investigations, posed an obstacle to ascertaining the facts. Given the similarities to previous epidemics, it is probable that the source of this cholera outbreak was someone who had traveled to Korea by ship or plane from one of the neighboring affected countries [1617].
(4) The 1991 cholera epidemic
In August 1991, a cholera outbreak occurred among mourners who had attended a funeral in Duwang-ri, Seocheon-gun, South Chungcheong Province. A notable feature of this outbreak was that it did not spread, although sporadic cases of cholera occurred across the country. Although Vibrio cholerae was isolated from sewage and seawater in Gunsan, and marine organisms in some other areas, the epidemic was small, and the epidemic period was short [18].
(5) The 1995 cholera epidemic
In 1995, an epidemic occurred over a period of 19 days from August 26. It originated in Pohang, in North Gyeongsang Province, and spread to Incheon, South Chungcheong Province, Gangwon Province and Gyeonggi Province.
(6) The 2001 cholera epidemic
After an index case was reported on August 29, a total of 139 confirmed cases of cholera subsequently occurred across the country. Of these, 105 cases were associated with a taxi-drivers' restaurant in Yeongcheon in North Gyeongsang Province. A further 33 cases had different sources of infection, and there was one unrelated case of cholera in an individual who had contracted the infection while traveling outside the country. A cook who worked in the taxi-drivers' restaurant was found to be the source of the epidemic associated with the restaurant in Yeongcheon [19].
(7) Cholera outbreaks after 2001
After the nationwide cholera epidemic in 2001, cholera outbreaks showed the following patterns: Except for 2 patients in 2002, all cases originated from, or were associated with, other countries until 2016. In 2016, cholera was transmitted to three individuals within Korea. This was the first time the domestic transmission had occurred within Korea since 2002, One additional case of foreign origin was reported. Most of the cases of foreign origin occurred among Koreans who returned to Korea after taking a vacation in Southeast Asian countries, including the Philippines, Thailand, Vietnam, India, Indonesia, China, and Cambodia.
2. Characteristics of Cholera
1) Characteristics of the classical cholera epidemic in 1946
When the last classical cholera epidemic occurred in 1946, there were 15,644 cases, and 10,181 deaths with a case fatality rate of 65%.
Hee-Myoung Park, who has served as President of Kyungpook National University Hospital and Dean of the College of Medicine, Kyungpook National University, was dispatched to Daegu Burip Hwaeseng Hospital (currently, Daegu Medical Center) to treat patients during the cholera epidemic. He described those days as follows [20]:
I realized that cholera patients could lose 15 to 20 kg due to dehydration in just 3 or 4 days. Their excreta looked like rice water, and although the excreta did not have much odor, they had sufficient volume to flood the floor of the hospital room and corridor. We had to wear rainboots. The patients were all skin and bones due to severe dehydration, and they looked like old men and women as they had wrinkles all over their bodies. We relied on fluids, which were rarely provided by the army.
2) Characteristics of El Tor cholera
(1) Incidence rate, and case fatality rate
The number of cases, the number of deaths, and the case fatality rate decreased markedly after the 1946 cholera epidemic. The highest case fatality rate since 1946 was 9% in 1969, and there have been no deaths due to cholera since 1995. These improvements were thought to be attributed to better nutrition, public health programs, hygiene, and improved access to health care, as well as the less virulent characteristics of the V. cholerae El Tor variant compared to those of the original V. cholerae.
(2) Distribution patterns
In the early stage, cholera epidemics showed an exponential increase in the number of cases, resembling the pattern of collective food poisoning outbreaks, and then cases became sporadic due to gradual spread by individuals with subclinical infection [21].
(3) Clinical characteristics
Regarding sex, the incidence of cholera was greater in women than in men. In adults, the incidence rate increased with age, and was highest incidence among individuals in their 50s and 60s [12] The latent period of cholera was only 1 to 3 days after exposure to a source of infection. In the 1969 and 1970 epidemics, 68% of cases had an onset within 6 hours of exposure [12]. The 11 cholera epidemics that occurred from 1963 to 2001 showed no differences in the clinical symptoms of the patients. Diarrhea and vomiting were common in all of the epidemics, and abdominal pain and fever occurred less frequently [12].
(4) Sources of infection
Introduction of infection from outside the country, infection by V. cholerae carrier-residents within the country, and intentional spread are all considered to be possible sources of the initial infection that triggered the epidemics. When a cholera epidemic occurred after several years without an outbreak, it is probable that the infection in the initial case (s) was introduced from outside the country by an infected traveler or contaminated foods or fluids. When epidemics occurred in two consecutive years, it is likely that individuals infected in the first year had persistent infection and spread cholera locally resulting in an outbreak the following summer, which then spread further and became a more generalized epidemic [1121].
Environmental pathogens are also a possible source of cholera infection [22]. When an environment favorable for the growth of zooplankton such as copepods is established by conditions such as flooding, cholera bacteria which exist in small quantities in natural conditions may rapidly proliferate in copepods, leading to infection of marine organisms in the next tier of the food chain, with zooplankton becoming a reservoir of infection [2324].
3. Cholera Prevention and Control
1) Prevention and control of the classical cholera epidemic in 1946
Professor Yong-Suk Ki at Gyungsung college of medicine, the only surviving person with first-hand experience in cholera prevention during the 1946 outbreak, trained faculty members, staffs, and students of the college of medicine at the request of the USAMGIK, organized cholera prevention teams, and sent them to key areas [25]. Cholera prevention teams from Gyungsung college of medicine submitted the Incheon Marine Quarantine Project Report, which is regarded as the first academic article on cholera epidemics in Korea after liberation.
Here is an account of Professor Jong-Hui Jeon, who experienced several cholera outbreaks, remembered the experience [26]:
I experienced two classical cholera outbreaks and seven El Tor cholera outbreaks. After cholera treatment was shifted to rehydration, people recognized that cholera was no longer a terrifying disease, and that it was is important to provide water as soon as possible to treat the disease. As a result, we were able to reduce the case fatality rate of the 1963 epidemic to 5.1%. When a cholera epidemic occurs, we should abstain from the idea of identifying cholera carriers as we did in the past, and quarantine patients in diarrhea centers for treatment. Then, you will reach a simple conclusion that ordinary hygiene measures, including a general hygiene knowledge and the use of disinfectants, would be sufficient to stop the spread of cholera.
2) El Tor cholera prevention and control in 2001
In 2001, the Central Epidemiological Investigation Team and the Epidemiological Investigation Team of North Gyeongsang Province established the prevention task force within public health centers in Yeongcheon and Gyeongju; strengthened monitoring of patients with diarrhea; and visited households in person, conducting a questionnaire survey and collecting stool samples to identify individuals who had eaten food at a restaurant for taxi drivers. To stop further spread from the restaurant, a microbiological screening was conducted of employees who worked with food in the risk areas (the areas with confirmed cases where there was a risk of further spread). To supplement the questionnaire survey, members of the investigation team reviewed medical records and interviewed healthcare professionals. To identify the source of infection, the Local Quarantine Center and the Department of Intestinal Pathogens at the Korea National Institute of Health conducted microbiological screening and a polymerase chain reaction (PCR) test of samples of marine organisms, seawater, and plankton in order to identify possible reservoirs of infection [19].
3) Cholera control
As cholera is mediated by water and food and multiple individuals can become infected from a single source, it is imperative to seek a prevention response immediately after an outbreak is identified. All cases should be reported without delay when an infected patient, physician, or anyone carrying cholera is diagnosed, an infected individual's dead body is examined, or when a case fatality occurs. The case should be reported by fax to the head of the responsible health center or through the Integrated Disease and Health Control System (http://is.cdc.go.kr).
Since 2002, WHO has selected the pathogens that are expected to increase in as a result of climate change, and have evaluated correlations between these pathogens and the environment. The WHO selected 11 pathogens, which require an early warning system to prevent their outbreak and spread, and cholera was the only intestinal pathogen included. Since 2005, Korea has operated Vibrio Net, a project investigating pathogenic Vibrio in the marine environment, and has performed monitoring on coastal seawater in Korea [27].
In the event of a cholera outbreak, a prevention task force has been established within the government to perform cholera prevention activities with the assistance of expert consultants. In cooperation with professional organizations such as the Korean Society of Infectious Diseases, the Korean Medical Association, and the Korean Hospital Association, cholera information and precautions are informed across the country.
 XML Download
XML Download