

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Some strains of methicillin-susceptible Staphylococcus aureus (MSSA) exhibit the inoculum effect against cefazolin, an antibiotic widely used to treat bacterial infections [12]. Cefazolin inoculum effect (CIE) is closely related to type A or C blaZ MSSA isolates [34]. Hence, the use of cefazolin for treating severe infections or large burden infections caused by CIE positive MSSA can lead to treatment failure [13456]. Cefazolin is frequently used as the antibiotic of choice for severe MSSA infections such as osteomyelitis and septic arthritis, due to its high tolerability and favorable dosing schedule [78].
The accessory gene regulator (agr) locus is a quorum-sensing (QS) gene cluster and virulence regulator of S. aureus and can play an important role in virulence [910]. Many studies have demonstrated that agr genotype can affect the antibiotic response of methicillin-resistant S. aureus (MRSA) [11121314]. Several studies have demonstrated that infection caused by MSSA with reduced vancomycin susceptibility was associated with poor clinical outcomes [15161718]. Further, Kok EY et al. reported that the reduced vancomycin susceptibility was associated with dysfunctional agr in MSSA bacteremia [19]. Although a previous study suggested that CIE could be associated with dysfunctional agr locus in MSSA bacteremia [20], there is a dearth of literature regarding agr genotype and its functional effects in MSSA. This study was aimed to demonstrate the association between the functionality or genotypic variation of agr locus in MSSA and the inoculum effect of beta-lactam antibiotics and its clinical significance.
Materials and Methods
1. Bacterial isolates and clinical information
The MSSA blood isolates were collected at a 2000-bedded tertiary care hospital in Korea during June 2014 to December 2017. Only the first bloodstream isolate from each patient was included in the study. Isolation of S. aureus and antimicrobial susceptibility tests were performed at the clinical microbiology laboratory of our institute using an automated system. Demographic data and clinical information about the study participants were retrospectively collected by the review of medical records. The study protocol (IRB No. H1910-030-084) was approved by the IRB at Pusan National University Hospital. and informed consents were waived.
2. Cefazolin Susceptibility tests and inoculum effects
The cefazolin minimal inhibitory concentrations (MICs) were determined by a broth microdilution method using cation-adjusted Mueller-Hinton II broth (Becton, Dickinson and Company, Sparks, MD), according to Clinical and Laboratory Standards Institute (CLSI) guidelines, except for the inoculum size of the strains [21]. MICs of high inoculum (HI, ~5 x 107 CFU/ml) were compared to the standard inoculum (SI, ~5 × 105 CFU/ml) to identify the stains with the CIE. The MIC value of each isolate was measured by two independent researchers. S. aureus strain TX 0117 (a high-level producer of type A β-lactamase), S. aureus ATCC 29213 (known to produce small amounts of type A β-lactamase), and S. aureus ATCC 25923 (a β-lactamase negative strain) were used as controls [122]. The CIE was defined as an increase in MICs to ≥16 μg/ml at high inoculums from the susceptible range of MIC at standard inoculum [23]. The MICs of vancomycin and linezolid were measured by the broth microdilution method and E-test (bioMérieux, Marcy-l'Étoile, France). The E-test was performed according to the manufacturer’s protocol. The data regarding susceptibility to agents other than cefazolin, vancomycin, and linezolid were collected through a review of medical record of microbiological data.
3. blaZ gene typing
Polymerase chain reactions (PCRs) were performed to amplify a 355-bp region within the blaZ gene by using the following primers: 5′-CAAAGATGATATAG TTGCTTATTC-3′ and 5′-CATATGTTATTGCTTGCACCAC-3′ [3]. PCR products were analyzed by DNA sequencing, and results were analyzed using the NCBI BLAST web interface (http://blast.ncbi.nlm.nih.gov/Blast.cgi). The β-lactamase type of each strain was classified based on the amino acid residues at positions 128 and 216 encoded by the blaZ gene [24].
4. agr functionality test and agr/blaZ genotyping
The functionality of the agr locus was measured by δ-hemolysin expression assays using S. aureus strain RN4220 as an indicator, and the absence of, or barely detectable, synergistic hemolysis was defined as agr dysfunction [25]. The genomic DNA of the isolates was extracted by the spin-column-based extraction method using a commercially available kit (Qiagen, Hilden, Germany). To determine agr group genotype, agr group specific multiplex PCR was performed using the primers that were previously described [26]. To determine blaZ gene genotype, PCR was performed using previously described primers and PCR products were analyzed by DNA sequencing [3].
5. Statistical analysis
R version 3.3.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analyses. Categorical variables were compared using Pearson’s chi-square test or Fisher’s exact test, and non-categorical variables were tested using the Mann-Whitney U-test or Kruskal Wallis test. All tests of significance were 2-tailed, and the results with P <0.05 were considered statistically significant.
Results
A total of 197 MSSA blood isolates were collected during the study period. The mean age of patients with MSSA bacteremia was 62.3 ± 20.3 years and 67% of these patients were males. Among the MSSA bacteremia patients, 54.3% had more than one comorbidity (mean Charlson comorbidity index score: 3.4 ± 2.5). The prevalence of the community-onset bacteremia was 57.4% and bones and joints were the most common site of infection (18.3%) followed by skin and soft tissues (15.2%).
From the 197 MSSA blood isolates, two samples were excluded from the analysis due to unclear agr genotype. In the remaining 195 isolates, genotype I was the most common (67.5%), followed by type III (16.2%), type IV (9.1%), and type II (6.1%). Sixty-eight MSSA isolates (34.5%) showed dysfunctional agr gene. We did not observe significant differences between the demographic and clinical characteristics between the 4 agr genotypes (Table 1). Although we observed a trend of association between agr type III positive MSSA bacteremia and skin and soft tissue infection, it was not statistically significant (Table 1).
Table 1
Comparison of demographic, clinical, and microbiological characteristics according to the agr genotype of methicillin-susceptible Staphylococcus aureus bacteremia isolates
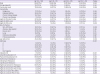
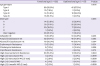
The proportion of dysfunctional agr was significantly higher in agr type III than other genotypes. Further, the proportion of blaZ genotype varied significantly according to the agr type; type B blaZ was most common in agr type I, whereas type A blaZ was most common in agr type III. Furthermore, more than 40% of agr type III MSSA exhibited CIE, whereas less than 10% of other agr genotype MSSA exhibited CIE (P <0.001). Significantly, resistance to erythromycin and clindamycin was most prominent in agr type III MSSA isolates (Table 1). The genotypes of blaZ and agr were significantly different between functional and dysfunctional agr positive MSSA (Table 2) isolates. However, we did not observe a statistically significant difference in the CIE positivity in these two groups (Table 2). The proportion of MSSA isolates with reduced vancomycin MIC was similar in four agr types (Table 1). Similarly, the proportion of MSSA with reduced vancomycin MIC was not significantly different between the dysfunctional and functional agr group (Table 2).
Table 2
Comparison of demographic, clinical and microbiological characteristics according to the functionality of agr locus of methicillin-susceptible Staphylococcus aureus bacteremia
Our results showed that among the four agr types, MSSA with the agr type III was associated with CIE. Isolates from agr III group exhibited a significantly higher CIE (40%) than the non-agr III group where only 5.5% isolates exhibited CIE (Fig. 1A). The agr III group also showed positive association with type A blaZ gene (Fig. 1B), and resistance to other antibiotics; erythromycin (Fig. 1C, 56.2% vs. 3.7%, P <0.001), clindamycin (43.8% vs. 2.5%, P <0.001), and high dose gentamicin (31.2% vs. 14.1%, P = 0.035).
Figure 1
(A) Proportion of cefazolin inoculum effect (CIE) positivity, (B) blaZ genotype, (C) erythromycin resistance between agr type III and non agr type III methicillin susceptible Staphylococcus aureus.

Interestingly, all of the CIE-positive isolates had type A or type C blaZ genotype. Therefore, we performed a subgroup analysis of MSSA with type A and C blaZ genotype. In subgroup analysis of type A blaZ positive MSSA, our results showed that while more than 90% of agr III isolates exhibited CIE, a very low proportion of non-agr III isolates (10%) had CIE (Fig. 2A). Furthermore, CIE was also associated with erythromycin resistance (Fig. 2B). However, there was no significant association between the CIE and agr functionality (Fig. 2C), and the functionality of agr genotype was not associated with CIE in the subgroup analysis of type C blaZ positive MSSA as well.

Discussion
Our study demonstrated that the inoculum effect of MSSA against β-lactam antibiotics, such as cefazolin, ampicillin/sulbactam, and piperacillin/tazobactam was associated with the agr type III, which was also the second most prevalent agr genotype observed in our study. These findings are consistent with a previous study [20]. However, unlike an earlier study, which concluded that agr dysfunction of MSSA was independently associated with inoculum effect against cefazolin [20], our results showed that there was no association between agr functionality and inoculum effect against β-lactam antibiotics. Instead, we found that agr group III was significantly associated with CIE. Moreover, the association between the agr type and CIE was more apparent in the type A blaZ gene-positive MSSA isolates. Although type A blaZ genotype has been positively associated with CIE, it is not uncommon to find MSSA isolates with the type A blaZ gene that do not show CIE [342728]. In our study, almost all of the MSSA with agr type III and type A blaZ genotype exhibited CIE. Therefore, there is a possibility that agr type III can be a useful indicator to discriminate CIE positivity among type A blaZ positive MSSA isolates.
Our study further demonstrated that a higher proportion of agr type III MSSA showed clindamycin and macrolide resistance, and a majority of such isolates had type A blaZ genotype. Clindamycin and macrolide resistance of MSSA is associated with CIE, and the association between CIE and clindamycin and macrolide resistance was significant among MSSA with type A blaZ genotype [29]. Our results suggest that agr type III is closely related to CIE, and clindamycin and erythromycin resistance. Collectively, these results indicate that cefazolin should be used with caution in treating high-inoculum MSSA infection if the isolates exhibited resistance to clindamycin or erythromycin [23].
Earlier studies have demonstrated an association between dysfunctional agr locus and reduced susceptibility to vancomycin and an enhanced capacity to produce biofilms in MSSA [1830]. Further, many studies reported that irrespective of vancomycin use as a therapeutic agent, reduced susceptibility to vancomycin in MSSA affected treatment outcomes [17293132]. Holmes NE et al. suggested that dysfunctional agr could be a predictor of high vancomycin MIC in MSSA infections [33]. However, in our study, neither dysfunctional agr nor agr genotype variation was associated with reduced vancomycin susceptibility.
The reason for the close association between the agr genotype with blaZ genotype, the inoculum effect of β-lactam antibiotics, and resistance of non- β-lactam antibiotics is not known. However, some data regarding the association between certain toxin genes and certain agr types is available. For instance, agr type III is associated with menstrual toxic shock syndrome toxins, while agr type IV genotype is associated with exfoliatins [343536]. Jarraud S et al. suggested that the bacterial pathogenicity is a cumulative result of specific combinations of virulence and regulatory genes in the appropriate genetic background [35]. In light of the available scientific literature and our results, we propose that certain agr alleles might associate with certain antibiotic resistance genes in a particular genetic background.
Although our study has some interesting and thought-provoking outcomes, it has several limitations. Firstly, our study was conducted at a single center in the southeastern region of Korea. Earlier studies have shown a varying prevalence of CIE positive MSSA or distribution of agr type among clinical isolates [3202737]. The inconsistent prevalence of CIE positive MSSA or distribution of agr types suggested that CIE positivity and its association with agr type could vary according to the geographic regions. Therefore, although our results form a credible reference for CIE positive MSSA and agr types, they lack universal relevance, and therefore, should be applied cautiously to other geographical regions. Second, we used the δ-hemolysin assay to detect MSSA isolates with agr dysfunction due to the convenience and lower cost than Northern blotting [38]. However, the δ-hemolysin assay may not be a sensitive marker for agr dysfunction and has shown an ambiguous result in an earlier report [39]. However, to minimize the shortcomings of the assay, two independent researchers analyzed the assay results. Moreover, the assays were repeated in events where discrepancies were observed in the results.
In summary, our results showed that the positivity of CIE and resistance of clindamycin could be associated with agr type III rather than agr dysfunction in MSSA bacteremia isolates. These findings were more prominent among MSSA with type A blaZ. Hence, we propose that Type A blaZ genotype with agr type III could be a useful indicator to genetically differentiate CIE positive MSSA isolates.
 XML Download
XML Download