

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Staphylococcus aureus is a nosocomial pathogen that has an exceptional ability to rapidly acquire resistance to antibiotics. After the emergence of methicillin-resistant S. aureus (MRSA), it has since then spread worldwide to become one of the leading causes of human bacterial infections.1) It remains a widespread problem not only in healthcare settings, but also in the community.
Because staphylococcal chromosomal cassette mec (SCCmec) typing has low discriminatory power, many molecular typing methods to discriminate MRSA for epidemiologic purposes have been developed. The gold standard in investigating MRSA outbreaks is pulse-field gel electrophoresis (PFGE) typing,2) however, because it is time-consuming and difficult to compare results from different laboratories, multi-locus sequence typing (MLST),3) and spa typing4) methods have been used to overcome reproducibility and exchange of results from different laboratories.
Healthcare institutions have been investing numerous resources to monitor and prevent healthcare associated (HA)-MRSA infections, which mostly cause infections in patients with underlying conditions or risk factors. However, in the recent decades, community associated (CA)-MRSA have disseminated worldwide to cause infections in otherwise healthy individuals, and PFGE type USA300, MLST sequence type (ST) 8, SCCmec type IVa clone has been one of the leading causes of CA-MRSA severe skin infections. Reports of this USA300 clone associated outbreaks have been published in the US, Europe, and Japan.56789)
An increase in both HA- and CA-MRSA outbreaks have also been reported in newborn and neonatal intensive care units (NICUs),1011) with molecular epidemiologic studies showing USA300 to be a major cause.121314) Methods to combat and prevent epidemics have been developed, and many institutions have been monitoring MRSA colonization in neonates and applying protocols involving universal decolonization methods such as application of mupirocin and chlorhexidine bathing to eradicate MRSA colonization. Many factors are involved in the prolonged transmission and frequent relapses of MRSA colonization in the NICU, which remain issues to be overcome.
The aim of this study was to investigate the molecular epidemiology of an MRSA outbreak at a nursery and NICU to identify the source of infection and understand the characteristics of the epidemic causing strain to prevent further transmission, prolonged carriage, and recolonization.
MATERIALS AND METHODS
1. Study design
An outbreak of MRSA occurred from August to September 2017, at a nursery and NICU center of a 670-bed secondary teaching and referral hospital in Korea (Fig. 1). This hospital has an average of about 150 normal and high-risk deliveries annually, and the nursery has 8 beds and NICU has 5 beds with one isolation room. A total of 11 nursing staff members are assigned to the nursery/NICU center. The nursery and NICU are separated into two isolated sections with glass walls and doors; and situated between the two sections is the nurses' station.
 | Fig. 1Timeline of the discovery of MRSA skin infections and colonizers.Patients with MRSA infections (square icon) and colonization (circle icon) are shown on the timeline. Their initial admission periods are shown as arrows. Patient C and D's MRSA isolates were not collected. Patients A-F had skin infections, and patient L was diagnosed with MRSA sepsis. Intervention included strict hand hygiene, cohorting of MRSA positive patients, and MRSA eradication by mupirocin oint application.
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus.
|
During the outbreak which lasted for a span of 2 months, all patients admitted at the nursery/NICU were included as study participants. Upon admission during this period, all patients underwent initial nasal, axillary, and periumbilical MRSA skin swab cultures. In 1-week intervals from the initial screening, a follow up culture was taken. When any of the sites were positive for MRSA, mupirocin oint application 3 times daily for 5 days was applied. The patients were also monitored for any symptoms or signs of MRSA infections, and upon discovery of any skin lesions or symptoms of sepsis, appropriate cultures from sites of infection were taken. All nursing and maintenance staff members of the nursery/NICU and delivery room, as well as all pediatric and obstetrics/gynecology residents and staff members that had any contact with the newborns or nursery/NICU facility were included in the initial MRSA nasal screening and follow up screening of healthcare workers.
Skin and soft tissue infection was defined in accordance with the practice guidelines for the diagnosis and management of skin and soft tissue infections updated by the Infectious Disease Society of America in 2014.15) Sepsis caused by MRSA was defined as a patient with fever (axillary body temperature ≥38.0°C) and MRSA cultured from the blood. An MRSA colonizer was defined as a patient with MRSA cultured from either the nasal, axillary, or periumbilical skin culture, without any symptoms or signs of infection. An MRSA carrier was defined as a healthcare worker who had MRSA cultured from an intranasal swab culture.
The Institutional Review Board (IRB) of Daejeon St. Mary's Hospital approved this study (IRB No. DC17SES10095). Informed consent was waived.
2. Bacterial isolation, identification, and antibiotic susceptibility testing
All MRSA isolated from patients with MRSA infections, colonizers, and healthcare workers were collected. After initial MRSA identification and antibiotics susceptibilities were tested using the automated microbiology system MicroScan Pos Breakpoint Combo Panel Type 44 (Siemens Healthcare Diagnostics Inc., West Sacramento, CA, USA), the isolates were stored at −70°C. The stored MRSA isolates were sub-cultured on mannitol salt agar plates at 37°C for 24 hours, producing yellow colonies within yellow zones.
3. DNA extraction and MRSA molecular typing
The chromosomal DNA of the sub-cultured MRSA isolates were extracted using a DNA extraction kit (DNeasy Kit; QIAGEN, Valencia, CA, USA) according to the instructions recommended by the manufacturer.
To use as a positive control, an MRSA isolate that had previously been identified and characterized as PFGE type USA 300, SCCmec type IVa, ST 8 was included in the study.
To identify the structural types of the mec element among the MRSA strains isolated during the study period, the protocol for multiplex polymerase chain reaction (PCR) strategy developed and validated by Oliveira and de Lencastre16) was followed, using the same oligonucleotide primers and PCR conditions. For MRSA isolates that were SCCmec type IV, a multiplex PCR of the J1 region upstream of the ccrAB locus in the staphylococcus cassette chromosome, which distinguishes the subtypes of SCCmec type IV, was performed using previously described methods reported by Milheiriço et al.17)
Typing using MLST of the MRSA isolates was performed by amplification and sequencing of the internal fragments of the seven housekeeping genes (arcC, aroE, glpF, gmk, pta, tpi, and ygiL) using oligonucleotide primers as previously described by Enright et al.,3) under the following PCR conditions: initial denaturation for 4 minutes at 94°C; 35 cycles of denaturation for 30 seconds at 94°C, annealing for 30 seconds at 53°C for the primers aroE, glpF, gmk, and pta, 57°C for the primers arcC, tpi, and ygiL, extension for 60 seconds at 72°C; and final extension for 4 minutes at 72°C. The sequences of each of the seven housekeeping genes were submitted to the MRSA database (https://pubmlst.org/saureus/) to designate a seven-integer number to identify the allelic profile for assigning the ST.
Spa typing was performed by amplification and sequencing of the spa gene which encodes protein A of S. aureus. The spa repeat region was amplified using forward primer spa-1113f (5′-AAAGACGATCCTTCGGTGAGC-3′) and reverse primer spa-1514r (5′-CAGCAGTAGTGCCGTTTTGCTT-3′) as previously described.1819) The sequences were then used to identify the repeat succession to determine the spa type using the database on the ridom spa server (https://spa.ridom.de/). A novel spa type was designated by submitting the chromatogram files of the forward and reverse sequences on the ridom spa server.
4. Virulence gene detection
The presence of the cytotoxin, Panton-Valentine leukocidin (PVL), was detected by PCR amplification and gel electrophoresis of the PVL gene. The following primers were used to screen for the PVL gene in the MRSA isolates: luk-PV-1, 5′-ATCATTAGGTAAAATGTCTGGACATGATCCA-3′ and luk-PV-2, 5′-GCATCAASTGTATTGGATAGCAAAAGC-3′.20)
Isolates showing low-level resistance to mupirocin underwent gene sequencing of the 450-bp portion of the native isoleucyl-tRNA synthetase (ileS)'s Rossman fold region containing the sequence of the known V588F mutation, as described previously by Yang et al.21): Mrm1 (5′-TCC CAG CAG ATA TGT ATT TAG AAG GT-3′) and Mrm2 (5′-AAC CAC TTG GTC AGG TAC AAT CAC A-3′).
RESULTS
1. Description of the outbreak and infection control measures
The outbreak was first suspected when the following events occurred: a newborn visited the emergency room 1 day after discharge due to irritability, multiple pustules on the axilla, and severe omphalitis with mucopurulent discharge from the umbilical stump (A). The following day, a second case discharged 2 days prior, visited the outpatient clinic presenting with axillary and inguinal pustules, and left thigh cellulitis (B). Two days later, 2 newborns (C, D) that were discharged from the hospital's nursery within a span of 2 days visited the outpatient clinic with multiple pustular lesions on the nasal, axillary, and umbilical area. When the pus culture results of the first 2 cases of multiple pustulosis showed heavy growth of MRSA, an MRSA outbreak at the hospital's nursery/NICU center was suspected, and immediately, the infection prevention and control team was alerted (Fig. 1).
All 8 patients admitted in the nursery/NICU at the time were examined thoroughly for any signs of skin infection and underwent surveillance by intranasal and axillary skin swab cultures. Two patients in the NICU were discovered with multiple axillary pustulosis (E, F), and initially 2 patients (I, J) were found to be colonized with MRSA. All patients with MRSA infection or colonization were isolated, and strict contact precaution was enforced (Fig. 1).
To find the source of MRSA, all 32 healthcare workers including nurses, staff physicians, residents, and interns working in the nursery/NICU and delivery room underwent MRSA initial screening by intranasal skin swab culture. Because X-ray technologists and NICU cleaning staff did not have direct contact with the patients, they were left out of the initial screening. A nurse in the nursery/NICU and an obstetrician were found to be MRSA carriers (G, H).
All patients with MRSA infections and MRSA colonizers underwent twice daily intranasal 2% mupirocin ointment (JW Pharmaceutical, Seoul, Korea) application for 7 days. Chlorhexidine bathing was not done due to controversies on its safety in use on neonates. The 2 healthcare workers (G, H) found to be MRSA carriers were advised to administer intranasal 2% mupirocin for 7 days as well. All newborns received weekly MRSA surveillance cultures.
Twelve days after the start of intervention, a 4-day old neonate outborn at another hospital was admitted to the nursery/NICU due to fever (L), and MRSA was grown on the patient's initial blood culture. The following week, 2 more newborns (K, M) were newly found to be colonized with MRSA. With the possibility of prolonged MRSA transmission, healthcare workers who were left out of the initial screening, as well as workers found to be MRSA carriers at the initial screening, were included in the second healthcare worker screening of nasal MRSA. The nurse (H) who was initially positive for MRSA was again positive for MRSA, and it was found that the nurse had not applied mupirocin ointment as advised. An obstetrician was also newly identified as a nasal MRSA carrier (N). No new cases of MRSA infection or colonization occurred afterwards. A total of 41 patients in the nursery/NICU were screened, and 11 were positive for MRSA during the study period (Fig. 1).
2. Clinical characteristic of study patients
During the period of MRSA outbreak, MRSA was isolated from a total of 11 neonates. Of these, 7 were isolated from the sites of infection (infection group), and 4 were cultured from colonized skin sites (colonized group). Of the patients included in the infection group, 5 were also found to have nasal/axillary MRSA colonized. The mode of delivery was cesarean delivery in 57.1% of the infection group vs. 75% in the colonization group, and the median gestational age (interquartile range [IQR]) was 38+3 (37+3–39+1) weeks in the infection group vs. 37+4 (33+1–41+0) weeks in the colonized group. The median age at MRSA isolation (IQR) was 6 days (5.0–9.0) in the infection group and 9 days (3.3–19.3) in the colonized group (Table 1).
Table 1
Clinical characteristics of patients with MRSA isolated during the outbreak

Values are presented as number of patients (%) or median (IQR).
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; IQR, interquartile range.
![]()
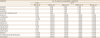
The 7 patients with MRSA infection included 4 diagnosed with multiple skin pustulosis, 1 with pustulosis and omphalitis, 1 with pustulosis and thigh cellulitis, and 1 patient with MRSA bacteremia without evidence of skin infection (Table 2).
Table 2
Clinical and molecular characterization of the MRSA causing infections in neonates during the outbreak
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; SCCmec, staphylococcal chromosomal cassette mec; MLST, multi-locus sequence typing; PVL, Panton-Valentine leukocidin; ACME, arginine catabolic mobile element; ST, sequence type; N, negative; P, positive.
*Strain not available for molecular genotype study; †New spa type; ‡Included as positive control.
![]()
3. Molecular epidemiology and antibiotic susceptibilities of the isolated MRSA during the outbreak
The MRSA isolated from the two patients who were diagnosed with multiple pustulosis at the outpatient department (C, D) were unable to be collected. Therefore, a total of 12 MRSA isolates from neonates with MRSA infection (n=5), colonization (n=4), and healthcare workers (n=3, 2 from the same nurse 1 month apart) were collected during the outbreak and analyzed. Healthcare worker G's MRSA isolate was un-typed due to failure of subculture (Fig. 1).
The MRSA strain causing skin infections in the nursery/NICU was SCCmec type II, ST 89, spa type 375 (Table 2), and was determined to be the outbreak strain. The strain causing MRSA bacteremia in the outborn patient admitted for sepsis was identified as SCCmec type IVa, ST 72, and a novel spa type designated as t17879. All typed MRSA isolates causing colonization in neonates and healthcare workers were SCCmec type IVa, ST 72. However, they differed in spa types: 2 of the neonates were colonized with the same spa type as the 2 isolates cultured at different time periods from the same nursery nurse (H), t664. Two other neonates were colonized with another spa type, t324. The isolate from the obstetrician (N) was also a different spa type, t2413 (Fig. 1 and Table 3).
Table 3
Molecular typing and virulence of MRSA causing infections and colonization

| MLST type (SCCmec Type) | Spa type (No.) | PVL | ||
|---|---|---|---|---|
| Neonate | HCW | |||
| Infection | Colonization | |||
| ST 89 (II) | t375 (4) | − | ||
| ST 72 (IVa) | t17879 (1) | − | ||
| t324 (2) | + | |||
| t664 (2) | t664 (2)* | + | ||
| t2413 (1)† | − | |||
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MLST, multi-locus sequence typing; SCCmec, staphylococcal chromosomal cassette mec; HCW, health-care worker; PVL, Pantone-Valentine leukocidin; ST, sequence type; −, negative; +, positive.
*Two isolates were cultured from the same nurse in neonatal intensive care unit; †Obstetrician.
![]()
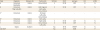
Of the total 9 MRSA isolates collected from neonates, SCCmec type IVa, ST 72 isolates (n=5) were resistant to penicillins, but susceptible to all other antibiotics. The outbreak causing SCCmec type II, ST 89, t375 strains (n=4) were multidrug resistant, showing resistance to antibiotics including penicillins, aminoglycosides, macrolides, clindamycin, and low-level resistance to mupirocin (minimum inhibitory concentration [MIC] 256 μg/mL) (Table 4).
Table 4
Antibiotic susceptibilities of MRSA isolated from neonates during the outbreak by MLST and spa type
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MLST, multi-locus sequence typing; ST, sequence type.
*All (n=4) had mupirocin intermediate susceptibility (minimum inhibitory concentration 256 μg/mL).
![]()
4. Virulence of the MRSA isolates
The presence of the PVL cytotoxin gene was investigated. The MRSA isolate used as a positive control, SCCmec type IVa, ST 8, t008, was positive for the PVL gene. The outbreak isolates causing skin infections were negative, however, two spa types belonging to ST 72, SCCmec type IVa, t664 and t324, were positive for the PVL cytotoxin.
The mechanism allowing the outbreak strain to show low-level mupirocin resistance was sought by sequencing the ileS gene. The outbreak MRSA (samples No. 4, 5, 7, and 8) showed a G→T point mutation at the 1852 position, resulting in an amino acid change from valine to phenylalanine (V588F) in the region of the Rossman fold of the isoleucine synthetase where mupirocin binds (Fig. 2).
 | Fig. 2ileS gene sequence and chromatogram image of MRSA isolates with low-level mupirocin resistance showing missense mutation. The gene sequence of the ileS gene of the outbreak strains (samples No. 4, 5, 7, and 8) showed a G→T point mutation at the 1852 position, resulting in an amino acid change from valine to phenylalanine (V588F) in the region of the Rossman fold of the isoleucine synthetase where mupirocin binds (S. aureus ileS gene sequence was obtained from PubMed GenBank accession No. X74219.1).Abbreviations: ileS, isoleucyl-tRNA synthetase; MRSA, methicillin-resistant Staphylococcus aureus.
|
DISCUSSION
Infections caused by MRSA continue to be an unceasing problem, both in hospitals and communities. The colonization of MRSA in newborns and patients in critical conditions predisposes them to subsequent MRSA infections, and therefore, all measures must be taken to not only prevent the colonization of MRSA, but also to eradicate sources of MRSA which can cause prolonged transmission in such settings. Therefore, the purpose of this study was to investigate an MRSA outbreak at a secondary referral university hospital's nursery and NICU to identify the source of infection and understand the characteristics of the epidemic causing strain to prevent further transmission, prolonged carriage, and recolonization. During the outbreak period, a total of 7 cases of MRSA infections occurred, 4 neonates were found to be colonizers, and 3 healthcare workers were found to be MRSA carriers.
To find the outbreak causing strain, MRSA isolates collected during the study period underwent genotyping. In this study, the skin infection causing outbreak strain was SCCmec type II, ST 89, t375. This strain has been reported to be a long-term persistent CA-MRSA strain causing staphylococcal scalded skin syndrome in Korean children with multidrug-resistance,22) and is also a strain found to cause skin and soft tissue infections in Japan.23) All other neonates were colonized or infected with SCCmec type IV, ST 72; which are one of the most prevalent CA-MRSA types causing skin infections in children in Busan,24) and most commonly found in adult carriers in Gyeongsang province in Korea.25)
In this study, given that MLST did not provide a high enough discriminatory power to further distinguish between strains within the same MLST sequence types, spa typing was used. Spa typing was especially useful in determining the epidemiological relationship between the isolates from outborn neonate admitted for MRSA sepsis and the other MRSA colonized neonates, which were all SCCmec type IV, ST 72. The isolate from outborn neonate was designated a novel spa type, t17879, which was a different spa type from the inborn neonates, who were colonized with spa types t664 and t324. In a MRSA study performed on Korean adults in Gyeongsang province, SCCmec type IV, ST 72, t664 (52.9%), and t324 (23.5%) were the most common types found in both colonizers and patients with clinical infections.25)
Healthcare workers are known to be possible sources or routes of MRSA transmission in hospital wards and intensive care units. In this study, through spa typing, it was possible to observe the significant role of healthcare workers on the spread of MRSA within the NICU, and how MRSA carriers who have constant contact with neonates can be a cause of prolonged MRSA transmission. During the outbreak, a nursery nurse was found to have MRSA nasal carriage early on after outbreak recognition. However, failure of MRSA eradication in this healthcare worker possibly led to a continued transmission to neonates with whom the nurse had direct contact with. The nurse was most likely to be the source or route of MRSA transmission because two neonates who were colonized with the same spa type as the nurse (t664) were both preterms with prolonged admission in the NICU, however, were admitted at different time periods without any overlap. This emphasizes the importance of recognizing and decolonizing healthcare workers who are MRSA carriers early on in an MRSA outbreak as part of an approach for infection control.
Multidrug resistance enhances an organism's fitness for survival, especially under conditions of antibiotics selective pressure, leading to capability for prolonged colonization. We found that the outbreak causing strain in this study was multidrug resistant, including resistance to erythromycin and clindamycin. Also, low-level mupirocin resistance (MIC 256 μg/mL) was detected in the outbreak strain, and sequencing of the ileS gene revealed a point mutation causing an amino acid change from valine to phenylalanine at the residue 588 in the region of the Rossman fold (Fig. 2), which is the most common mutation found in MRSA isolates that show low-level resistance to mupirocin.212627) The clinical significance of low-level mupirocin resistance is not yet fully understood, however, studies have shown that although MRSA isolates that show low-level mupirocin resistance may be eradicated with mupirocin as effectively as susceptible isolates, the rate of recolonization is higher.2829) This is significant especially in hospital settings, because mupirocin is not only used to treat skin infections, but also to eradicate MRSA carriage. In the NICU, protocols of intranasal mupirocin application for 5 days have been used to eradicate nasal MRSA carriage.303132) With the increase in mupirocin resistance, failure of eradication and prolonged transmission or recolonization may consequently lead to MRSA infection outbreaks.
There are two major mechanisms known for resistance to mupirocin: MRSA isolates that demonstrate a high level mupirocin resistance with MIC >256 μg/mL acquire the plasma-mediated mupA or mupB gene, which encodes a novel ileS,3334) whereas MRSA isolates with low-level mupirocin resistance (MIC 8 to 256 μg/mL) show nonsense point mutations affecting the Rossman fold where mupirocin binds in the native ileS gene.26) The prevalence of mupirocin resistance is increasing worldwide, and a study done on MRSA causing infections in children with atopic dermatitis showed that since 2009, the proportion of MRSA resistant to mupirocin has increased from 4.3% to 35.6% in 2016.35) Therefore, the need to monitor both low-level and high-level mupirocin resistance in MRSA is essential.
The ability of S. aureus to produce PVL, which is a cytotoxin that causes leukocyte destruction and tissue necrosis, leads to an increased virulence, and is associated with severe skin lesions such as cellulitis, furunculosis, cutaneous abscesses, and skin necrosis.20363738) Mostly found in the USA300, SCCmec type IV, ST 8 clone, there are reports of other clones that harbor this cytotoxin.39) Because the outbreak strain in this study, SCCmec type II, ST 89, t375, presented mainly as skin infections, the presence of the PVL cytotoxin was examined. The outbreak MRSA strain did not carry the PVL gene, and there have not yet been any reports that SCCmec type II, ST 89 clones produce this toxin.
Although the presence of the PVL gene does not imply that the gene will be expressed to transcribe the toxin, multidrug-resistant MRSA isolates that produce PVL may pose a severe threat to patients because multidrug resistant MRSA demonstrating resistance to toxin-suppressing antibiotics such as clindamycin and rifampin limits the choice in antibiotics for treatment of infections. In this study, 2 spa types were found to carry the PVL gene, t324, which was found in 2 colonized neonates, and t664, which was isolated from a nurse who was a possible source or route of transmission to 2 colonized neonates. Although both strains did not yet cause diseases in the carriers, their high potential for severe infections make them a threat in the NICU. Therefore, monitoring PVL-producing MRSA for screening, decolonization, and determining treatment choice is essential.
In conclusion, during this MRSA outbreak, many different MRSA types were found to co-circulate. Identifying the outbreak strain as well as strains co-circulating in the intensive care unit and investigating their virulent characteristics through molecular epidemiologic studies broadens clinicians understanding about their clinical burden, and aids in controlling infections and transmission of strains that are possible threats to patients. This study showed the importance of eradicating not only the outbreak strain, but also decolonizing healthcare workers who could play a vital role in the transmission of MRSA with virulent potentials.
 XML Download
XML Download