

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Minsoo Shin , Eun Hwa Choi, Mi Seon Han
, Eun Hwa Choi, Mi Seon Han
, Eun Hwa Choi, Mi Seon Han
Abstract
Purpose
Periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA) syndrome is a leading cause of periodic fever in children. This study describes the clinical characteristics of PFAPA syndrome in patients from a single center.
Methods
Thirteen children diagnosed with PFAPA syndrome at Seoul National University Children's Hospital were included in this study. Retrospective medical chart reviews were performed.
Results
Among the 13 patients, 8 (61.5%) were male. The median follow-up duration was 3.3 years (range, 10 months–8.3 years). The median age of periodic fever onset was 3 years (range, 1–6 years). All patients had at least 5 episodes of periodic fever and pharyngitis, managed with oral antibiotics, before diagnosis. The median occurrence of fever was every 3.9 weeks and lasted for 4.2 days. All patients had pharyngitis and 12 (92.3%) had cervical lymphadenitis. Blood tests were performed for 12 patients, and no patients had neutropenia. Both the C-reactive protein and erythrocyte sedimentation rate were elevated at medians of 4.5 mg/dL (range, 0.4–13.2 mg/dL) and 29 mm/hr (range, 16–49 mm/hr), respectively. Throat swab cultures and rapid streptococcal antigen tests were negative. Nine (69.2%) patients received oral prednisolone at a median dose of 0.8 mg/kg, and in 6 (66.7%) patients, fever resolved within a few hours. Three (23.1%) patients received tonsillectomy and adenoidectomy.
Figures and Tables
Table 1
Clinical manifestations of 13 patients with periodic fever, aphthous stomatitis, pharyngitis, and adenitis syndrome
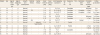
Abbreviations: PD, prednisolone; T & A, tonsillectomy and adenoidectomy; CL, cervical lymphadenitis; P, pharyngitis; N, nausea; ITP, idiopathic thrombocytopenic purpura; AP, abdominal pain; FS, febrile seizure; R, rash; T, tongue change; GN, glomerulonephritis; H, headache.
*Father, mother, and brother had history of adenoid hypertrophy; †Rash on periorbital, cervical, and trunk area; ‡Patient 3 and 7 had strawberry and whitish tongue, respectively.
![]()
Table 2
Laboratory findings of 13 patients with periodic fever, aphthous stomatitis, pharyngitis, and adenitis syndrome at the time of diagnosis

Abbreviations: WBC, white blood cell count; Seg, segmented neutrophil; ANC, absolute neutrophil count; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; Ag, antigen; PCR, polymerase chain reaction; N.D., not done; AdV, adenovirus; RV, rhinovirus; EV, enterovirus.
*At the time of diagnosis, the patient did not have any respiratory symptoms.
![]()
Table 3
Clinical manifestations of periodic fever, aphthous stomatitis, pharyngitis, and adenitis syndrome in children reported in Korea*

![]()
References
1. Marshall GS, Edwards KM, Butler J, Lawton AR. Syndrome of periodic fever, pharyngitis, and aphthous stomatitis. J Pediatr. 1987; 110:43–46.

2. Marshall GS, Edwards KM, Lawton AR. PFAPA syndrome. Pediatr Infect Dis J. 1989; 8:658–659.
3. Thomas KT, Feder HM Jr, Lawton AR, Edwards KM. Periodic fever syndrome in children. J Pediatr. 1999; 135:15–21.
4. Feder HM, Salazar JC. A clinical review of 105 patients with PFAPA (a periodic fever syndrome). Acta Paediatr. 2010; 99:178–184.
5. Hofer M, Pillet P, Cochard MM, Berg S, Krol P, Kone-Paut I, et al. International periodic fever, aphthous stomatitis, pharyngitis, cervical adenitis syndrome cohort: description of distinct phenotypes in 301 patients. Rheumatology (Oxford). 2014; 53:1125–1129.
6. Kolly L, Busso N, von Scheven-Gete A, Bagnoud N, Moix I, Holzinger D, et al. Periodic fever, aphthous stomatitis, pharyngitis, cervical adenitis syndrome is linked to dysregulated monocyte IL-1β production. J Allergy Clin Immunol. 2013; 131:1635–1643.
7. Kang HR, Kim SW, Bae GB, Park JH, Kang YM, Lee JM, et al. A case of PFAPA (Periodic fever, aphthous stomatitis, pharyngitis, and cervical adenitis) syndrome. Korean J Infect Dis. 2001; 33:219–222.
8. Chae JH, Hwang AR, Park SH, Suh BK. A case of PFAPA (periodic fever, aphthous stomatitis, pharyngitis, cervical adenitis) syndrome. Korean J Pediatr. 2006; 49:991–995.
9. Hong SP, Shin HJ, Kim YH, Choe BK, Choi WJ, Kim AS, et al. A case of PFAPA syndrome mimicking cyclic vomiting syndrome. Korean J Pediatr Gastroenterol Nutr. 2006; 9:85–91.
10. Song J, Hong S, Kweon Y, Jung S, Cha S. A case of PFAPA (periodic fever, aphthous stomatitis, pharyngitis, cervical adenitis) syndrome. Korean J Pediatr Infect Dis. 2007; 14:194–198.
11. Renko M, Lantto U, Tapiainen T. Towards better diagnostic criteria for periodic fever, aphthous stomatitis, pharyngitis and adenitis syndrome. Acta Paediatr. 2019; 108:1385–1392.
12. Dale DC, Welte K. Cyclic and chronic neutropenia. Cancer Treat Res. 2011; 157:97–108.
13. Ben-Chetrit E, Touitou I. Familial mediterranean fever in the world. Arthritis Rheum. 2009; 61:1447–1453.
14. Butbul Aviel Y, Harel L, Abu Rumi M, Brik R, Hezkelo N, Ohana O, et al. Familial mediterranean fever is commonly diagnosed in children in Israel with periodic fever aphthous stomatitis, pharyngitis, and adenitis syndrome. J Pediatr. 2019; 204:270–274.
15. Gattorno M, Caorsi R, Meini A, Cattalini M, Federici S, Zulian F, et al. Differentiating PFAPA syndrome from monogenic periodic fevers. Pediatrics. 2009; 124:e721–8.
16. Dytrych P, Krol P, Kotrova M, Kuzilkova D, Hubacek P, Krol L, et al. Polyclonal, newly derived T cells with low expression of inhibitory molecule PD-1 in tonsils define the phenotype of lymphocytes in children with periodic fever, aphtous stomatitis, pharyngitis and adenitis (PFAPA) syndrome. Mol Immunol. 2015; 65:139–147.
17. Cheung MS, Theodoropoulou K, Lugrin J, Martinon F, Busso N, Hofer M. Periodic fever with aphthous stomatitis, pharyngitis, and cervical adenitis syndrome is associated with a CARD8 variant unable to bind the NLRP3 inflammasome. J Immunol. 2017; 198:2063–2069.
18. Di Gioia SA, Bedoni N, von Scheven-Gête A, Vanoni F, Superti-Furga A, Hofer M, et al. Analysis of the genetic basis of periodic fever with aphthous stomatitis, pharyngitis, and cervical adenitis (PFAPA) syndrome. Sci Rep. 2015; 5:10200.
19. Renko M, Salo E, Putto-Laurila A, Saxen H, Mattila PS, Luotonen J, et al. A randomized, controlled trial of tonsillectomy in periodic fever, aphthous stomatitis, pharyngitis, and adenitis syndrome. J Pediatr. 2007; 151:289–292.
20. Abramson JS, Givner LB, Thompson JN. Possible role of tonsillectomy and adenoidectomy in children with recurrent fever and tonsillopharyngitis. Pediatr Infect Dis J. 1989; 8:119–120.
21. Garavello W, Romagnoli M, Gaini RM. Effectiveness of adenotonsillectomy in PFAPA syndrome: a randomized study. J Pediatr. 2009; 155:250–253.
22. Lantto U, Koivunen P, Tapiainen T, Renko M. Long-term outcome of classic and incomplete PFAPA (periodic fever, aphthous stomatitis, pharyngitis, and adenitis) syndrome after tonsillectomy. J Pediatr. 2016; 179:172–177.e1.
23. Peridis S, Pilgrim G, Koudoumnakis E, Athanasopoulos I, Houlakis M, Parpounas K. PFAPA syndrome in children: A meta-analysis on surgical versus medical treatment. Int J Pediatr Otorhinolaryngol. 2010; 74:1203–1208.
 XML Download
XML Download