

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Perineal trauma can occur spontaneously or as a result of obstetric interventions, such as an episiotomy or operative vaginal delivery.12 The reported incidence of perineal trauma during vaginal delivery is approximately 85%, but can vary in different settings, depending on clinical practice and conditions during vaginal delivery.2 Anal sphincter injuries, which are the most severe perineal trauma events, have gradually increased in number over the last several decades, with incidence rates ranging from 4.1% to 16.0% in several population-based studies.34 Perineal trauma during vaginal delivery has been shown to be associated with significant maternal morbidities, including blood loss, perineal pain, infection, dyspareunia, urinary incontinence, flatus, and fecal incontinence, and to lead to the development of comorbidities, including sexual dysfunction, pelvic organ prolapse, and rectovaginal and vesicovaginal fistulas.356 Thus, the prevention of perineal trauma is important because its associated morbidities have a profound effect on both the physical and psychological well-being of the mother, which may result in social isolation and the marginalization of those with ongoing morbidity.7
Hyaluronidase (HAase) is an enzymatic complex that depolymerizes and hydrolyzes hyaluronic acid, which reduces the viscosity of hyaluronic acid and improves both tissue diffusion and the resorption rate of excess fluids.89 HAase is involved in several physiological and pathological reactions and, therefore, has been utilized in various fields of medicine, such as fertilization,10 wound healing,11 ophthalmic surgery,12 and local anesthesia.13 During the 1950s and 1960s, HAase was used to prevent perineal trauma and to reduce the need for an episiotomy.141516171819202122 Some studies have suggested a beneficial effect for perineal HAase injections during spontaneous vaginal delivery: HAase injections reduced the frequency of episiotomy and severe perineal lacerations (third- or fourth-degree perineal lacerations) and increased the frequency of an intact perineum following delivery.2122 However, no difference in the incidences of episiotomy and severe perineal lacerations has been reported in randomized trials.2223 Although HAase is commonly used in clinical practice, its potential use as a method to prevent perineal trauma is controversial. Therefore, we aimed to evaluate whether perineal HAase injections during vaginal deliveries reduce perineal trauma in nulliparous women.
Go to : 
MATERIALS AND METHODS
Study design and participants
This multi-center, double-blind, placebo-controlled, randomized study included women undergoing vaginal delivery from January 2016 to March 2017 at five university-based clinical centers in Korea. Inclusion criteria were a maternal age between 19 and 40 years, gestational age between 37 weeks, 0 days and 41 weeks, 6 days, nulliparous women with no previous record of vaginal birth, vertex presentation, and singleton pregnancy. Exclusion criteria were multifetal gestations, non-vertex presentation, fetal congenital anomaly, estimated birth weight ≥4000 g, abnormal placental implantation, hypersensitivity to HAase, and women in whom vaginal delivery was not feasible.
Eligible women were randomly assigned to one of two groups (HAase injection and control group) using a permuted block randomization method previously generated by a statistician. To calculate the sample size, we presumed that the frequency of perineal injuries greater than or equal to first-degree lacerations in women without HAase treatment was 75.7%.15 If the same number of women were enrolled in the study and control groups, 73 women were needed in each group to detect a 31% risk reduction in perineal injury, with a type I error rate of 5% and a power of 80%.24 Therefore, considering a drop-out rate of 20%, we enrolled 184 women.
Procedures and perineal management
The HAase injection group was injected with 3 mL of 5000 IU HAase (Hirax®, BMI Korea, Seoul, Korea) mixed with 3 mL of 1% lidocaine hydrochloride solution, and the control group was treated with a combination of 3 mL of normal saline and 3 mL of 1% lidocaine hydrochloride solution. They received injections with their treatment solutions in the perineal subcutaneous tissue at the center and in the left and right of the perineum within 1 hour before fetal expulsion through the vagina. An episiotomy was performed upon each clinician's judgment with indications including a rigid perineum or fetal distress.
Study outcomes
Data were collected during labor and at 1 hour and 24 hours after delivery. All deliveries and postpartum evaluations were conducted by one of the authors according to the research protocol and described procedures.
The primary outcomes were perineal lacerations (greater than or equal to a first-degree laceration). Secondary outcomes were perineal edema and episiotomy. Perineal laceration was classified according to the classification originally described by Sultan and Fernando25: 1) a first-degree laceration is that of either the vaginal epithelium or perineal skin only; 2) a second-degree laceration involves the perineal muscles, but not the anal sphincter; 3) a third-degree laceration exhibits disruption of the anal sphincter muscles; and 4) a fourth-degree laceration is a third-degree tear with disruption of the anal epithelium. Severe perineal lacerations were defined as third- and fourth-degree lacerations. If an episiotomy was performed and no evidence of a third- or fourth-degree lacerations was observed, the event was categorized as a first- or a second-degree laceration. Perineal edema was identified by the application of pressure to the swollen skin of the perineum with a finger and categorized into five grades: 1) Grade 0 showed no change in pre-delivery contour; 2) Grade 1 had mild pitting and slight indentation with a depth within 2 mm; 3) Grade 2 had moderate pitting edema, and the indentation subsided rapidly (10–15 seconds) with a depth of 4 mm; 4) Grade 3 had deep pitting, and the indentation remained for a short time (about 1 minute) with a depth of 6 mm and appeared swollen; and 5) Grade 4 had deep pitting, the indentation subsided over 2–5 minutes with a depth of about 8 mm, and the perineum was very swollen.26 Perineal edema was evaluated at 1 hour and 24 hours after delivery. Information on side effects, such as fever, infection, and pain, were evaluated in both groups to determine the safety of HAase.
Statistical analysis
Analyses were performed according to the intention-to-treat principle. We compared continuous variables using the two-sample t-test or Wilcoxon rank-sum test and categorical variables using the χ2 test or Fisher's exact test. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA). p values <0.05 were considered statistically significant.
Ethical approval
Ethical approval was obtained from the institutional review boards of Dongguk University Ilsan Hospital (reference 2015-132), Asan Medical Center (reference 2016-0087), Kangbuk Samsung Hospital (reference KBSMC 2015-12-017), Samsung Medical Center (reference SMC 2015-11-039), and Soonchunhyang University Seoul Hospital (reference SCHUH 2015-10-014). Written informed consent was obtained from all participants. This study was retrospectively registered at the Clinical Research Information Service (CRIS, http://cris.nih.go.kr) in Korea on May 9, 2018 (KCT0002855, URL: https://cris.nih.go.kr/cris/en/search/search_result_st01.jsp?seq=11421).
Go to :
RESULTS
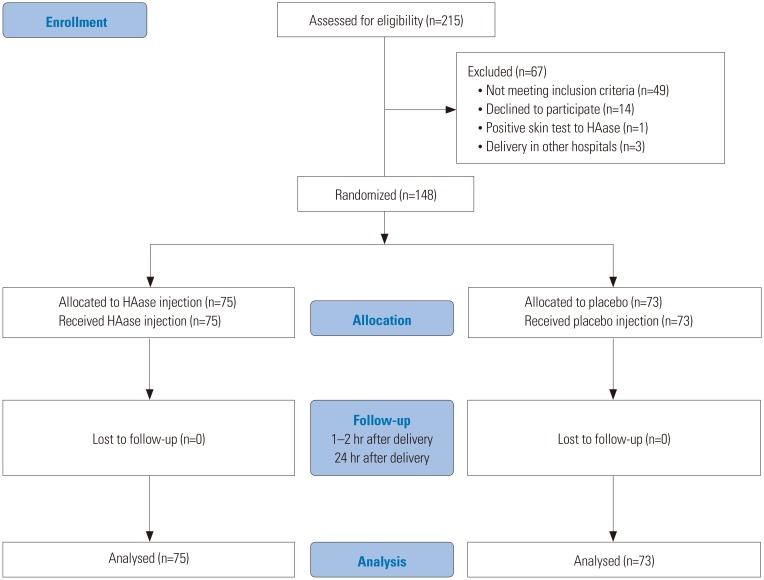
A total of 215 eligible women were screened, and 148 women were enrolled and underwent randomization. 75 women were assigned to the HAase injection group, and 73 women were assigned to the control group (Fig. 1). One woman in the control group was not evaluated after delivery, because she delivered by emergency cesarean section after perineal injection.
A total of 84 women (56.8%) underwent an episiotomy, and 13 women (8.8%) had an intact perineum. First-, second-, third-, and fourth-degree lacerations were observed in 34 women (23.0%), 88 women (59.5%), 11 women (7.4%), and one woman (0.7%), respectively. Maternal variables and newborn outcomes, including maternal age, gestational age at delivery, maternal body mass index (BMI), birth weight, and head circumference of newborns, were similar in the HAase injection and control groups (Table 1).
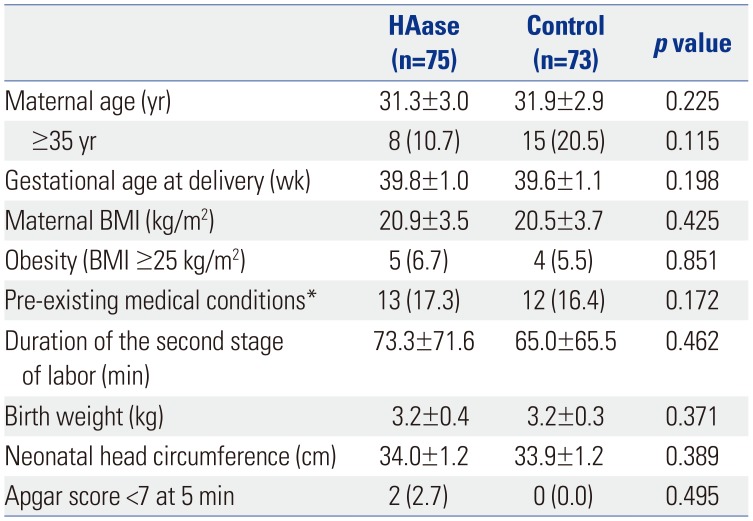
Table 1
Characteristics of Mothers, Newborns, and Deliveries
HAase, hyaluronidase; BMI, body mass index.
Data are presented as a mean±standard deviation or n (%) unless otherwise indicated.
*Pre-existing medical conditions include underlying diseases, such as maternal hypertension, diabetes, and hypothyroidism, or diseases during pregnancy, such as hepatitis, nephritis, and pneumonia.
![]()
We compared perineal lacerations between the HAase injection group and the control group (Table 2). No significant differences were found in the degree of perineal laceration between the groups. Intact perineum was observed in 10.7% of the women in the HAase injection group and 6.8% of the women in the control group. However, the difference therein between the two groups was not statistically significant (p=0.422).There were also no significant differences in the incidence of severe perineal lacerations between the two groups (p=0.498). Even when analysis was conducted among women without episiotomy, there were no statistically significant differences in the degrees of perineal laceration between the two groups (p=0.574).
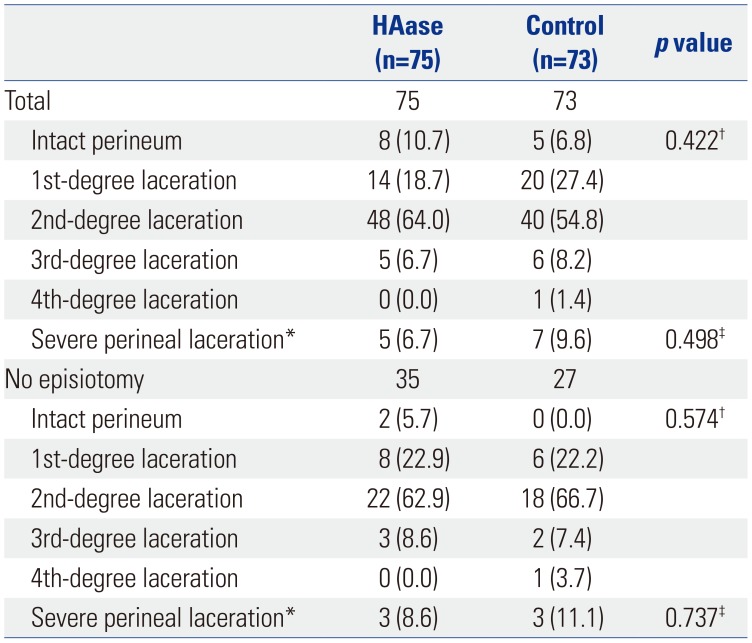
Table 2
Comparison of Perineal Lacerations between the Group Treated with Hyaluronidase Injections and the Control Group
HAase, hyaluronidase.
Data are presented as n (%) unless otherwise indicated. The control group had data missing from one woman due to an emergency cesarean delivery.
*Severe laceration was defined as a 3rd-/4th-degree laceration; †Greater than or equal to first-degree; ‡Severe perineal lacerations were compared using χ2 test and Fisher's exact test.
![]()
We compared perineal edema at 1 hour and 24 hours after vaginal delivery between the HAase injection and control groups (Table 3). The women who received HAase injections showed significantly improved perineal edema at 24 hours. compared to women in the control group who received a placebo (p=0.008).
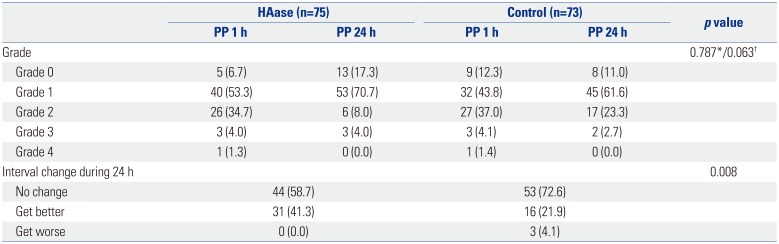
Table 3
Comparison of Degrees of Perineal Edema between the Group Treated with Hyaluronidase Injections and the Control Group
![]()
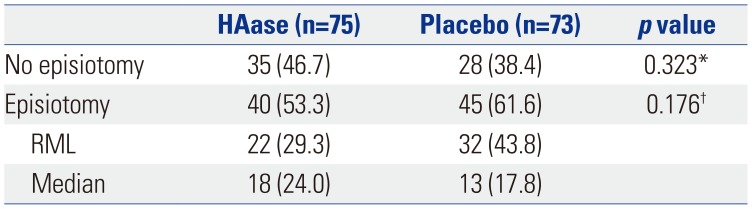
We compared the rates and types of episiotomy between the HAase injection and the control groups (Table 4). Episiotomy was more frequently performed in the control group than in the HAase injection group (61.6% vs. 53.3%, p=0.323, respectively); however, the difference was not statistically significant. There was also no significant difference in the types of episiotomy between the two groups (p=0.176).
Neither group reported serious adverse events. However, mild adverse events were reported in two women in the HAase injection group: One woman complained of fever after delivery, but recovered before discharge from the hospital. We confirmed that the fever was not related to HAase. The other woman complained of perineal pain at the injection site, but recovered before discharge from the hospital. Other mild adverse events, including changes in blood pressure, pulse rate, white blood cell count, and platelet count, were observed, although the differences between the two groups were not significant.
Go to :
DISCUSSION
Perineal trauma after vaginal delivery, especially third- and fourth-degree lacerations, can result in substantial morbidities that negatively affect a mother's quality of life. HAase was used during childbirth in the 1950s and 1960s to prevent perineal trauma, but was gradually replaced with episiotomy. However, many reports have demonstrated that an episiotomy is a risk factor for perineal trauma.27 Therefore, the utilization of HAase injections into the perineum during labor to prevent perineal trauma and to decrease the frequency of episiotomies is important and is the focus of our study. In our study, there were no significant differences in the frequencies of perineal lacerations and episiotomy, although perineal edema was significantly improved in the HAase injection group, compared to the control group.
There are several possible reasons for the observed lack of difference in the incidences of severe perineal lacerations and episiotomy between HAase and control groups despite a lower rate of severe perineal lacerations and episiotomy in the HAase injection group. Several studies have reported a reduction of perineal trauma using HAase injections; however, most of these studies are case series, and the number of studies was small.152328 Randomized controlled trials have found no statistically significant differences in severe perineal outcomes between women who received perineal HAase injections and those who received placebo injections152428; however, the women who received perineal HAase injections during the second stage of labor had a lower incidence of perineal laceration.1528 Notwithstanding, the techniques used, the timing of the injections, and the doses of HAase administered varied in each study, which makes it difficult to compare results among the studies. The HAase injections in our study did not prevent severe perineal trauma, which may have been the result of an inadequate drug effect duration or drug dosage. We used 5000 IU of HAase within 1 hour within fetal expulsion through the vagina. However, it may not have allowed enough time for HAase to soften and relax the perineal tissue and increase tissue elasticity. In addition, the low incidence in severe perineal lacerations between the HAase injection and control groups may explain the lack of difference. It is also possible that HAase has no effect on perineal tissue elasticity or that local infiltration may make the perineum thicker and may interfere with perineal elasticity.
HAase injections in our study were found to be effective in the reduction and recovery of perineal edema during the first 24 hours after delivery. Perineal edema is associated with perineal pain and postpartum discomfort after vaginal delivery. Rapid recovery from perineal edema allows for the resumption of maternal activities of daily living, such as lying down, sitting, walking, infant care, breastfeeding, and urination.429 Our study showed that a high percentage of women in the HAase injection group had improved perineal edema at 24 hours, which suggests that HAase injections improve tissue diffusion and the resorption rate of excess fluid.
In our study, episiotomy was performed slightly less in the HAase injection group than in the control group, although the difference was not statistically significant. Among women with episiotomies, right mediolateral episiotomy was performed more frequently in both groups. Since episiotomy is known to be a risk factor for severe perineal laceration, many researchers have recommended selective episiotomy during vaginal delivery. The type of episiotomy can affect the incidence of severe perineal lacerations. As for perineal edema, although there are few studies about the relationship between the types of episiotomy and perineal edema and HAase injections, the performance of episiotomy or types of episiotomy could affect the degree of perineal edema and recovery. In this study, we performed selective episiotomy, which was performed when it was indicated for reducing the confounding effect of routine episiotomy to perineal trauma. Further study is needed to identify the association between HAase injections and episiotomy (performance and type) and perineal laceration or edema after delivery. No HAase injection-related severe complications in the mothers and newborns were observed, which suggests that HAase injections during labor are safe.
The strength of our study is its double-blind, placebo-controlled, randomized design. As a limitation, our study was a multi-center study, which can introduce measurement bias. Further research with a larger sample cohort is recommended to elucidate the appropriate dose of HAase and the optimal injection time to prevent perineal lacerations during vaginal delivery.
In conclusion, although there were no significant differences in the frequencies of severe perineal lacerations, perineal HAase injections during delivery in nulliparous women significantly reduced perineal edema, compared to the placebo group, and are safe for both the mother and fetus.
Go to :
 XML Download
XML Download