

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ulcerative colitis (UC) is a chronic relapsing and remitting inflammatory disease of the colon.1 Biologic therapy with tumor necrosis factor alpha (TNF-α) inhibitors, such as infliximab (IFX) and adalimumab (ADA), is currently the most effective treatment for inducing and maintaining clinical remission in patients with moderate to severe UC, and has been reported to reduce the risk of hospitalization and surgery.2 IFX and ADA were approved for patients with UC in South Korea in 2010 and 2013, respectively. Considering the differences in the molecular constructs, routes of administration, and dosing intervals of these two TNF-α inhibitors, there may be differences in efficacy. However, although randomized clinical trials (RCTs) have demonstrated that IFX and ADA are superior to placebo in the treatment of UC,34 there have been no head-to-head comparison trials of these two agents. As such, the need to understand the relative effectiveness of these two agents has remained unmet, and decisions on the choice of TNF-α inhibitor have primarily been based on the preferences of the patients and clinicians.
An indirect comparison meta-analysis previously suggested that IFX is more effective than ADA in inducing remission, response, and mucosal healing at 8 weeks, although these two agents exhibited comparable efficacy after 52 weeks of maintenance treatment in patients with UC.5 Another network meta-analysis showed no difference in the induction and maintenance of remission and response between IFX and ADA in patients with UC.6 Additionally, a recent network meta-analysis revealed no difference in the rates of hospitalization and colectomy for UC between IFX and ADA.7 However, these results are from indirect comparisons rather from direct comparisons. Moreover, prior network meta-analysis studies are limited by a lack of head-to-head trials, a small number of registration trials, short follow-up (within 54 weeks), and restricted inclusion criteria in registration trials.
Although several observational studies have compared clinical outcomes between IFX and ADA in patients with UC, their results were inconsistent.8910111213 Furthermore, most of the previous studies on this topic were performed in Western countries.8910111213 Despite the increasing number of patients with UC in Asia,1415 data on the comparative effectiveness of IFX and ADA in Asian patients are extremely scarce. Therefore, we conducted a nationwide population-based study to compare the efficacy of IFX and ADA in biologic-naïve Korean patients with UC using a health claims administrative database. To better evaluate the real-world outcomes of these two biologics, we compared clinically important outcomes, including colectomy, emergency room (ER) visits, hospitalizations, and need for corticosteroids.
MATERIALS AND METHODS
Data source
The South Korean government operates a mandatory nationwide insurance system (National Health Insurance, NHI); therefore, all information about health-care utilization is registered in a comprehensive database, which is operated by the Health Insurance Review and Assessment Service (HIRA). The NHI provides mandatory universal health insurance covering all forms of health-care utilization, including outpatient care, pharmaceutical services, and hospitalization. Medical institutions electronically submit health-care use information to ensure reimbursement, and this information is integrated into the HIRA claims database, which covers the entire population of South Korea (approximately 51 million people). The HIRA database contains information on all patients, including demographic characteristics, ambulatory care history, principal diagnosis, and comorbidities, according to International Classification of Diseases 10th revision (ICD-10) codes, prescriptions, and diagnostic or surgical procedures.161718 The source population for this study was derived from NHI claims data from 2008 to 2016.
Patient identification and data capture
To improve the diagnostic accuracy of UC, only patients with data on both appropriate diagnostic codes and UC-related medicine prescriptions were selected.161718 The ICD-10 codes K51.0–51.9 indicate UC. UC-related medicine prescriptions were defined as prescriptions of 5-aminosalicylic acid (ASA) for ≥1 month, immunomodulators (azathioprine or 6-mercaptopurine) at least once, and/or biologics at least once.161718 To rule out the use of drugs for other autoimmune diseases, these medications were confined to prescriptions received from a gastroenterology clinic. During the study period, the biologics approved for the treatment of UC in South Korea were IFX, ADA, and golimumab. However, the actual use of golimumab was very rare during the study period because this biologic was approved only in May 2015. Therefore, in this study, golimumab could not be compared with IFX and ADA.
The date of UC registration in the HIRA database was considered the date of diagnosis. Given that previous prevalent cases could confound the incidence rate, we set a washout period of 2 years; therefore, we were able to analyze patients with UC diagnosed from January 1, 2010, to December 31, 2016. Patients in whom the first line of biologics was golimumab, those who were exposed to both IFX and ADA, and those with a history of colectomy before starting biologic therapy were excluded from the analysis.
The primary outcomes of interest were colectomy, ER visits, hospitalizations, and need for corticosteroids after the first use of biologics. Colectomy was identified using the procedural code. ER visits were defined as patient visits to the ER with UC as the primary diagnosis. Hospitalization was defined as admission for ≥3 days in the department of gastroenterology. Finally, new corticosteroid use was defined as moderate- to high-dose corticosteroid use (≥30 mg prednisolone, ≥50 mg methylprednisolone, or ≥200 mg hydrocortisone) after 2 months of the first prescription of biologics.
Statistical analysis
The incidence rates of colectomy, ER visits, hospitalizations, and need for corticosteroids were calculated per 100 person-years, and 95% confidence intervals (CIs) for the incidence rate were estimated using a Poisson distribution. For each group, the crude risk of outcomes was described using the Kaplan-Meier method and log-rank test. We used Cox proportional hazard models to adjust for potential confounding variables. Baseline covariates, including sex, the period from UC diagnosis to first biologics use, age, region, hospital scale, and steroid use at the time of first biologics use, were adjusted as time-fixed covariates. The use periods of cumulative biologics and concomitant medications, including 5-ASA and immunomodulators, were adjusted as time-dependent covariates.
We further performed a sensitivity analysis on patients who used biologics for ≥6 months and a stratified analysis based on the use of TNF-α inhibitor monotherapy or combination therapy with immunomodulators (concomitant use of immunomodulators). Concomitant use of immunomodulators was defined as prescriptions within 30 days before and/or after the start date of biologics. The results are presented as hazard ratios (HRs) with corresponding 95% CIs. All analyses were performed using the SAS Enterprise Guide (SAS Institute Inc., Cary, NC, USA), and p<0.05 was considered statistically significant.
Ethical considerations
All identifiable personal information in medical records was de-identified to comply with the Health Insurance Portability and Accountability Act. In addition, as the information in the HIRA database is encrypted, the database does not contain personal identifiers. The protocol of this study was approved by the Institutional Review Board of Severance Hospital, Yonsei University College of Medicine (IRB No. 4-2017-0927).
RESULTS
Patient characteristics
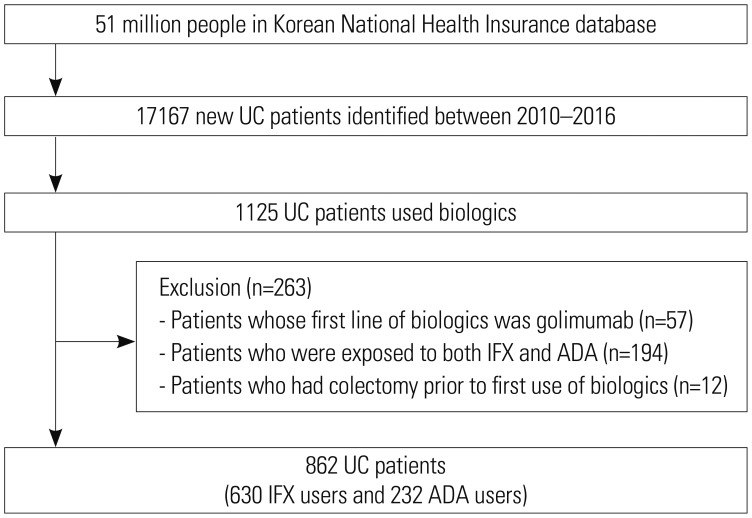
We identified 17167 patients who were diagnosed with UC between 2010 and 2016, of whom 1125 started their first TNF-α inhibitors during the study period. Of these 1125 patients, 57, 194, and 12 were excluded because of the use of golimumab, the use of both IFX and ADA, and a history of colectomy before the start of biologics, respectively. Ultimately, 862 patients were included in the study, of whom 630 were treated with IFX and 232 were treated with ADA (Fig. 1). The median follow-up period after starting TNF-α inhibitors was 1.8 years (interquartile range, 0.8–3.3 years).
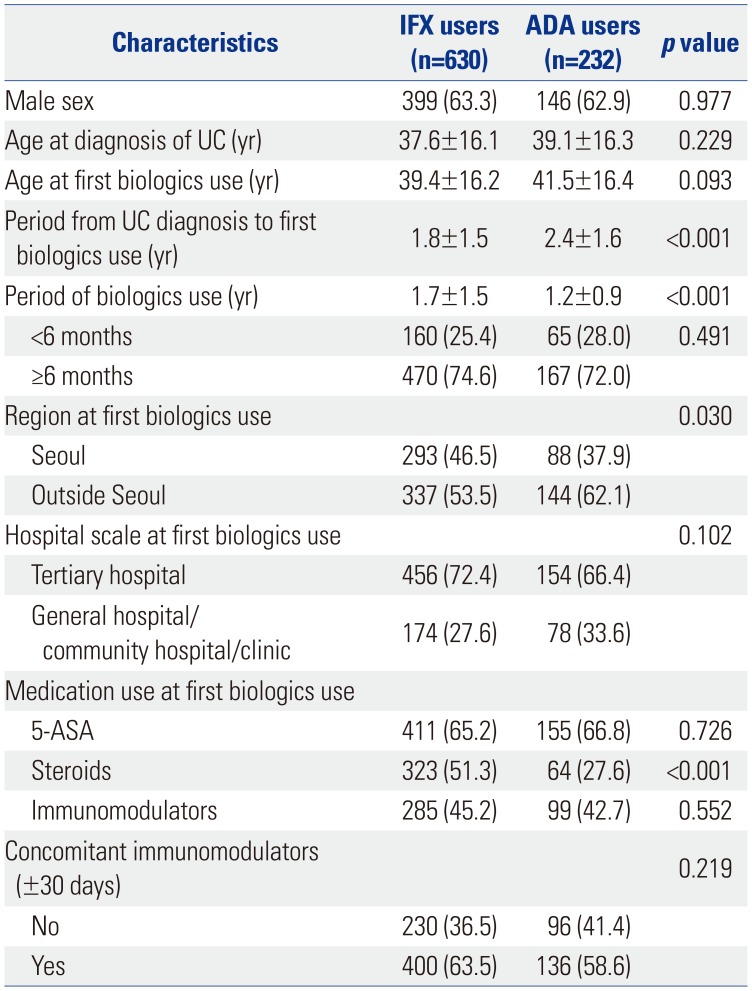
Table 1 shows the comparison of the baseline characteristics of IFX users and ADA users. Sex, age at UC diagnosis, and age and hospital scale at first biologics use were not different between IFX users and ADA users. The mean period from UC diagnosis to first biologics use was shorter in IFX users than in ADA users (1.8±1.5 years vs. 2.4±1.6 years, p<0.001), whereas the mean period of biologics use was longer in IFX users than in ADA users (1.7±1.5 years vs. 1.2±0.9 years, p<0.001). During the follow-up period, 429 (68.1%) of 630 IFX users continued IFX therapy, and 183 (78.9%) of 232 ADA users continued ADA therapy. The rate of steroid use at the time of first biologics use was higher in IFX users than in ADA users (51.3% vs. 27.6%, p<0.001), whereas the rate of concomitant immunomodulator use was not different between IFX users and ADA users (63.5% vs. 58.6%, p=0.219).
Comparative effectiveness of ADA vs. IFX
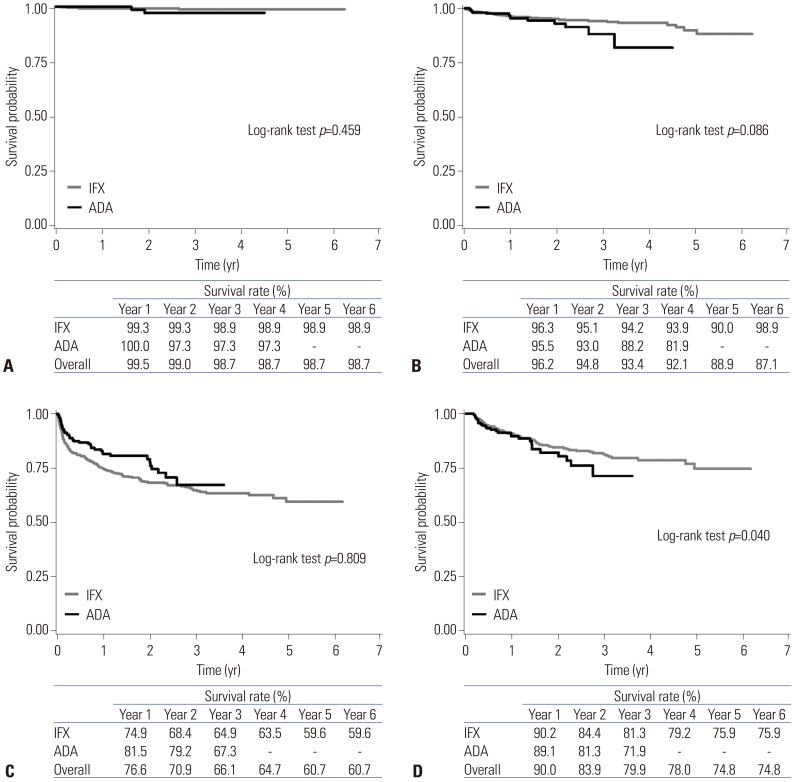
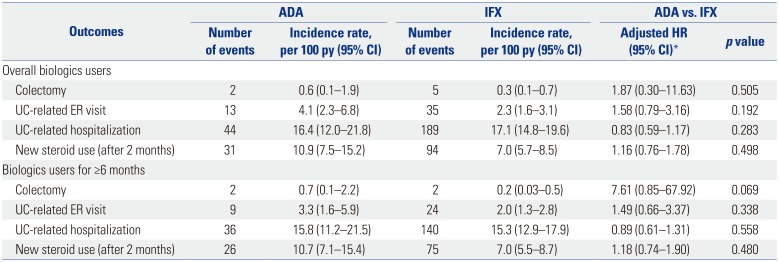
There were no significant differences in the cumulative probabilities of colectomy (p=0.459) (Fig. 2A), ER visits (p=0.086) (Fig. 2B), and hospitalizations (p=0.809) (Fig. 2C). At 1 and 3 years after the start of the first biologics, the cumulative rates of colectomy were 0.7% and 1.1%, respectively, for IFX users and 0% and 2.7%, respectively, for ADA users. The number of patients who underwent colectomy during the follow-up period was 5 among IFX users and 2 among ADA users. The surgical procedure codes for these patients were as follows: Q2671 right or left hemicolectomy (one IFX user and one ADA user), Q2672 total colectomy (three IFX users and one ADA user), and QA925 total coloproctectomy with ileostomy (one IFX user). Meanwhile, the cumulative rates of ER visits at 1 and 3 years were 3.7% and 5.8%, respectively, for IFX users and 4.5% and 11.8%, respectively, for ADA users. For hospitalization, the cumulative rates at 1 and 3 years were 25.1% and 35.1%, respectively, for IFX users and 18.5% and 32.7%, respectively, for ADA users. Even after adjustment for confounding variables, there were no significant differences in the risk of colectomy (HR, 1.87; 95% CI, 0.30–11.63), ER visits (HR, 1.58; 95% CI, 0.79–3.16), and hospitalizations (HR, 0.83; 95% CI, 0.59–1.17) between the two groups (Table 2).
Sensitivity analysis and stratified analysis
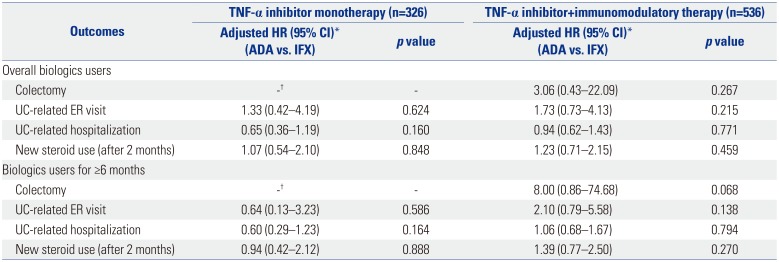
In a sensitivity analysis restricted to patients who used biologics for ≥6 months, we also observed no significant differences in the risk of colectomy (HR, 7.61; 95% CI, 0.85–67.92), ER visits (HR, 1.49; 95% CI, 0.66–3.37), hospitalizations (HR, 0.89; 95% CI, 0.61–1.31), and corticosteroid use (HR, 1.18; 95% CI, 0.74–1.90) between IFX users and ADA users (Table 2). Additionally, on stratified analysis, there were no significant differences in the risk of ER visits, hospitalizations, and corticosteroid use between IFX users and ADA users with either TNF-α inhibitor monotherapy or combination therapy (Table 3).
DISCUSSION
In this nationwide population-based study of 862 biologic-naïve Korean patients with UC, we found that IFX and ADA were comparable in terms of the risk of colectomy, UC-related ER visits, UC-related hospitalizations, and new initiation of corticosteroids. These results were stable even when only patients who used biologics for ≥6 months were analyzed. Additionally, these results were unchanged in patients treated with biologic monotherapy or those treated with combination therapy with immunomodulators. Our findings indicate that IFX and ADA elicit comparable effects on UC-related, clinically important, real-world outcomes.
Most studies on the comparative outcomes of IFX and ADA in UC have been conducted in Western countries, and data on this topic in Asian countries are extremely scarce. Our results are consistent with the results from prior Western studies. Although our study could not compare the rates of induction and maintenance of remission between IFX and ADA, several Western observational studies have reported no difference in clinical remission and response between these two drugs. A retrospective study performed in the United States including biologic-naïve IFX-treated (n=424) and ADA-treated (n=380) patients with UC showed no significant differences in time to remission, no rectal bleeding, normal stool count, and normal physician global assessment.9 In a Canadian single-center cohort study involving 53 patients with UC, the responses to induction and maintenance therapy were similar between IFX and ADA.13 Recently, a Japanese study involving 25 biologic-naïve patients with UC also demonstrated no statistical differences in clinical response, remission, mucosal healing, and steroid-free remission rates at weeks 14 and 54 between IFX users (n=10) and ADA users (n=15).19
In addition, similar to our findings, some Western studies have reported no difference in the risk of surgery, hospitalization, and steroid utilization between IFX and ADA users. In a US study conducted at two tertiary referral academic centers, there were no differences in UC-related surgery, hospitalizations, or prednisone prescription within 1 year after the initiation of IFX (n=337) or ADA (n=82).8 An Italian population-based cohort study using health administrative databases also revealed that the risk of steroid utilization did not differ between 469 IFX and 91 ADA new users with UC.12 Furthermore, consistent with these results, an indirect comparison through a recent network meta-analysis showed no difference in the rates of UC-related hospitalization and colectomy between IFX and ADA, although only two RCTs were included in this network meta-analysis.7
However, a few Western studies showed different results from those of our study. In a US administrative claims-based study of 1400 patients with UC who were new users of TNF-α inhibitors, there were no significant differences in the risk of all-cause or UC-related hospitalization and serious infections between IFX- and ADA-treated patients; however, the need for corticosteroid use was lower in IFX-treated than in ADA-treated patients.10 In this study, the risk of surgery was low in both IFX- and ADA-treated patients, and the number of surgical events was very small, precluding meaningful analysis.10 In contrast, a nationwide population-based study of 1719 biologics-naïve patients with UC in Denmark demonstrated that the risks of surgery and new corticosteroid initiation were comparable among IFX users and ADA users; however, ADA was associated with a higher risk of all-cause hospitalization and serious infections, and showed a trend toward a higher risk of UC-related hospitalization, compared with IFX.11 Although the results of these two studies are not identical, these results may suggest that IFX may be more beneficial than ADA in the treatment of UC. In line with these results, two network meta-analyses also indicated the superiority of IFX over ADA in patients with UC.2021 A network meta-analysis by Danese, et al.20 showed the superiority of IFX over ADA in both inducing and maintaining remission in UC. Recently, another network meta-analysis by Cholapranee, et al.21 revealed that ADA was inferior to IFX in inducing mucosal healing in UC. However, the results of these network meta-analyses are indirect comparisons based on comparison trials of “IFX vs. placebo” and “ADA vs. placebo,” rather than head-to-head comparisons.
Although the reason for the difference between our findings and those from some Western studies cannot be clearly elucidated, there may be a few potential explanations. First, although IFX and ADA have similar mechanisms of action in targeting TNF-α, there are subtle differences in pharmacokinetics, which may explain the difference in efficacy. The dose of IFX administered intravenously is determined based on body weight, whereas ADA administered subcutaneously is a fixed-dose drug that does not take body weight into consideration. This may result in a difference in bioavailability. The prevalence of obesity is relatively lower in Korea than in the United States and Europe.22 More specifically, the data from the Organization for Economic Cooperation and Development showed that the prevalence of obesity defined by body mass index (BMI) ≥30 kg/m2 among individuals older than 15 years was the highest in the United States at 38.2% and the second lowest in Korea at 5.3% in 2017.22 Although there are no data on the prevalence of obesity in Korean patients with UC, it is expected to be lower than the prevalence of obesity in US patients with inflammatory bowel disease (IBD), reported as 18–33%.232425 ADA, a fixed-dose drug, may be advantageous for non-obese patients, but disadvantageous for obese patients, considering only the drug effect. Indeed, a prior study reported that higher BMI in patients with IBD is predictive of dose escalation during ADA treatment.26 Additionally, a retrospective cohort study demonstrated a higher need for dose escalation due to early loss of response in obese patients with Crohn's disease treated with ADA, but not in those treated with IFX.27 Moreover, another study observed a trend toward a lower trough level in ADA-treated patients with a BMI of >30 kg/m2.28 The relatively lower BMI in Korean patients than in Western patients may have helped overcome the disadvantage of ADA bioavailability. Second, in our clinical practice, patients with more severe disease may have been preferentially prescribed IFX rather than ADA. This may cause bias in the results against IFX because more severe patients with a higher risk for surgery and hospitalization may be more likely to be prescribed IFX. Actually, in our study, the rate of steroid utilization at the first biologics use was higher in patients initiated on IFX than in those initiated on ADA (51.3% vs. 27.6%). However, this factor was adjusted for in our analysis. Lastly, as the phenotype and genetic susceptibility of IBD differ between Western and Asian patients,1429 the efficacy of IFX or ADA may vary depending on race and ethnicity.
This is the first nationwide population-based study to compare the real-life outcomes of IFX and ADA in Korean patients with UC. Nevertheless, our findings should be interpreted with caution, taking into account the limitations associated with the study design. First, this was a retrospective, claims-based, and observational study. Accordingly, information on disease severity and phenotypes, such as the extent of UC, were unavailable; thus, confounding factors that can affect clinical outcomes could not be considered. Second, the efficacy of IFX and ADA in clinical responses or endoscopic responses, such as mucosal healing, could not be compared because information on clinical and endoscopic activity was not available. Third, safety outcomes, such as serious or opportunistic infections, were not evaluated. Fourth, because ADA was approved for patients with UC in South Korea on July 2013, there was a limitation in assessing the long-term outcomes of ADA. Fifth, the impact of dose escalation or interval shortening, which may influence clinical outcomes, was not assessed. Sixth, we did not verify the diagnostic accuracy of UC. However, considering that this study included only patients who used IFX or ADA and that these TNF-α inhibitors are approved only for UC patients with moderate to severe activity (Mayo score 6 to 12 and endoscopy subscore ≥2) in South Korea, it seems very unlikely that non-UC patients would have been misdiagnosed as having UC. Lastly, we did not investigate factors contributing to preferences for IFX or ADA. A previous Korean study reported that the most influential reason for choosing IFX was “doctor's presence” and that for ADA was “ease of use.”30 The study also demonstrated that having a >60-minute travel time to the hospital was a significant independent predictive factor for ADA preference.30
Despite these limitations, our study provides a better understanding of the real-world outcomes of IFX and ADA in Korean patients with UC. In this administrative claims-based study, we found no significant differences in four clinically important outcomes, including colectomy, ER visits, hospitalizations, and corticosteroid use, between IFX users and ADA users. These results suggest that IFX and ADA have comparable effectiveness in biologic-naïve patients with UC. In the absence of RCTs with which to directly compare these two TNF-α inhibitors, our study suggests that for Korean patients with UC, deciding on either IFX or ADA can be based the preference of the patients and/or their clinicians.
 XML Download
XML Download