

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of ascending aorta aneurysm in the general population is reported to be 0.3–0.4%.1 Several observational studies have demonstrated that if this condition is left untreated it may lead to fatal aortic dissection or rupture.234
Indications for ascending aorta replacement surgery are based on aortic diameter and historical data on the risk of complications of elective surgery. Surgery should be performed for Marfan syndrome and a maximal aortic diameter ≥50 mm. A lower threshold of 45 mm can be considered in patients presenting with a positive family history, hypertension, coarctation, or an annual increase of more than 3 mm. Managing thoracic aortic aneurysm in patients with bicuspid aortic valve has been very controversial. European Society of Cardiology guidelines recommend that surgery should be performed in patients with a bicuspid aortic valve with a maximal diameter ≥55 mm.56 Meanwhile, however, Norton and Yang7 have emphasized the importance of aortic root phenotype in bicuspid aortic valve and have suggested that diameters of the root exceeding 45 mm should be indications for surgery.
The management of a moderately dilated ascending aorta remains controversial. For patients with one of the above indications for surgery, a lower aortic diameter threshold of >45 mm may be applied for aortic valve replacement (AVR), depending on age, body size, etiology of valvular disease, and intraoperative shape and thickness of the ascending aorta. However, these guidelines are not appropriate for all patients with dilated ascending aorta undergoing AVR surgery (e.g., patients at high risk for stroke). In such patients, a less aggressive approach of ascending aortic wrapping during AVR may be selected to reduce the cardiopulmonary bypass time and minimize the risk of circulatory arrest.
External wrapping is a simple technique that involves shorter pump and cardiac ischemia times than ascending aorta replacement, as well as reduced hypothermia, which may result in improved short-term outcomes. However, the long-term results of this method compared with replacement of the ascending aorta are unclear. Furthermore, there is significant concern that intrinsic aortic wall abnormalities present in aneurysm patients may persist after aortic wrapping, and therefore, these patients may remain at higher risk of developing sinus of Valsalva or arch aneurysms.8910 The aim of the present study was to investigate the long-term outcomes of aortic aneurysms in patients who underwent aortic wrapping, with a particular focus on identifying predictors of aortic redilation, depending on the region of three different levels.
MATERIALS AND METHODS
Ethics statement
This study was conducted in accordance with the principles embodied in the Declaration of Helsinki and was approved by the Institutional Review Board of Severance Hospital, Republic of Korea (IRB number: 2018-1593-001). The requirement for acquisition of informed consent from individual patients was waived owing to the retrospective nature of this study.
Patients
A total of 1050 patients underwent AVR for aortic stenosis or regurgitation between 1995 and 2015 at our institution. Of these, 301 consecutive patients presented with ascending aortic dilatation of 40–55 mm. Wrapping of the ascending aorta during AVR was carried out for 96 patients, and these patients were included in the present study. The decision to perform concomitant aortic procedures was influenced by aortic size, morphology of the aortic valve, and expected surgical risks of complications affecting left ventricular function. The final decision was at the discretion of the attending surgeon.
Exclusion criteria were as follows: 1) patients with defined congenital anomalies, 2) patients who underwent aortic valve repair instead of replacement, 3) patients with a history of cardiac surgery, 4) patients who underwent concomitant procedures on other valves (mitral or tricuspid) because of the possible effect on hemodynamic performance, and 5) patients with acute dissecting aortic aneurysms.
Perioperative data including echocardiographic reports, heart computed tomography (CT) imaging, and all operative records were collected from the database and through retrospective review of medical records. Aortic measurements are made using the true short axis projection acquired from double oblique views, from one blood-wall boundary to another. The aortic diameter was measured at the level of the sinuses of Valsalva, the sinotubular (ST) junction, the mid-ascending aorta, and the proximal arch. Interpretations of CT examinations were provided by a cardiothoracic radiology specialist with >10-year experience in evaluating various image modalities. During echocardiographic assessments, the size of the ascending aorta was routinely measured in the parasternal long axis view.
Surgical technique
Aortic wrapping was performed after the completion of hemostasis and protamine reversal following AVR. Polytetrafluoroethylene (PTFE) or double-velour vascular grafts were used to surround the native ascending aorta (Fig. 1). Materials for wrapping were chosen according to the surgeons' preferences. Three surgeons participated in this study and used a common technique to ensure consistency in the tightness of the wrap. The length of the vascular graft was determined according to the distance along the greater curvature between the ST junction and the origin of the innominate artery. Once the native aorta was surrounded by the graft, the graft was attached by continuous suturing with 4-0 or 3-0 polypropylene (Ethicon Inc., Somerville, NJ, USA). To prevent graft migration, several interrupted 3-0 polypropylene mattress sutures (Ethicon Inc.) were used to anchor the proximal and distal parts of the graft to the aorta.
Endpoints and data collection
The primary endpoints were all-cause death and adverse aortic events, including aortic dissection, rupture, reoperation, and sudden death. Data were obtained through regular visits to the outpatient clinic. Early mortality was defined as death within 30 days of surgery.
The secondary endpoint was diameter change of the aorta during follow-up. To assess changes in maximal diameter at individual aortic levels in patients who underwent AVR with wrapping, serial postoperative echocardiographic and CT data were reviewed. Generally, follow-up echocardiographic evaluations were performed at 6 months, 12 months, and yearly thereafter.
Statistical analysis
Simple descriptive statistics were used to summarize the data. Continuous variables are presented as mean±standard deviation. Categorical data are described using frequencies and percentages.
A paired t-test was performed to compare maximal aortic diameter measured immediately after surgery with the final follow-up measurement. Subgroup analysis using a linear mixed-effects model (LMM) was performed to analyze the overall outcomes of aortic diameter for the 96 patients who underwent more than two postoperative imaging studies. The following variables were included in the univariable model: age, sex, body surface area, presence of bicuspid aortic valve or hypertension, wrapping material (either PTFE or not), and initial ascending aortic diameter. A total of three variables were included in the multivariable model, with a significance level of 0.10. To determine the best threshold for aortic diameter with redilation as a confounding factor, receiver operating characteristic (ROC) curve analysis was performed.
The Kaplan-Meier method was used to generate survival curves and calculate 5- and 10-year survival statistics and freedom from significant redilation. The IBM SPSS Statistics package (version 23.0, IBM-SPSS Inc., Armonk, NY, USA) was used for all statistical analyses.
RESULTS
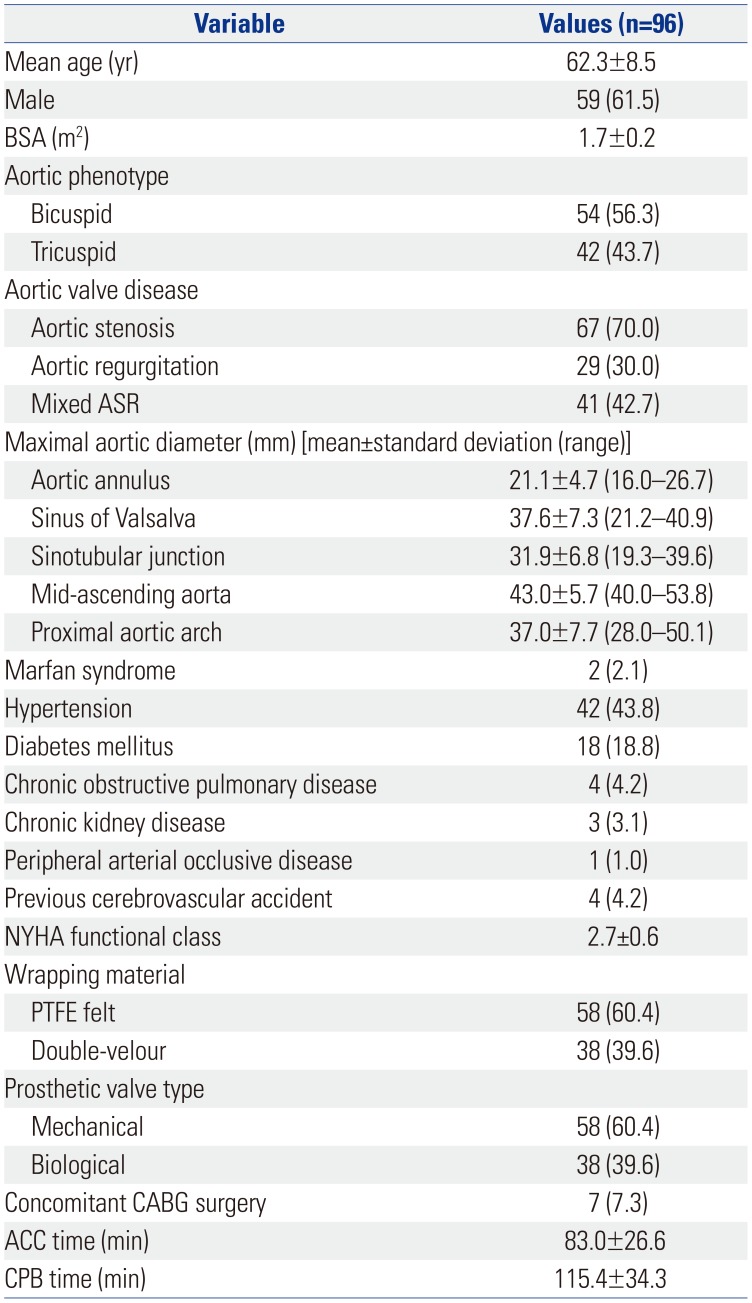
The mean age at the time of surgery was 62.3±8.5 years. Patients were predominately male (61.5%); 56.3% had bicuspid aortic valves; and 43.8% had hypertension. The dominant functional valvular disease was aortic stenosis for 70% of patients and regurgitation for 30% of patients. The mean preoperative mid-ascending aortic diameter was 43.0±5.7 mm (Table 1).
Operative data
As shown in Table 1, [Teflon® (DuPont Pharmaceuticals, Wilmington, DE, USA) or Dacron® (DuPont Pharmaceuticals, Wilmington, DE, USA) felt] was used to surround the native ascending aorta in 60.4% of patients. Double-velour vascular grafts [Hemashield® (Meadox Medicals, Oakland, NJ, USA) or Intergard® (InterVascular, La Ciotat, France)] were used in 39.6% of patients. There were no uniform institutional policies with respect to the procedures performed. Mechanical prostheses were used in more cases (60.4%) than biological prostheses (39.6%), and the mean size of prosthetic aortic valve was 22.2±1.8 mm. The mean aortic cross-clamping time was 83.0±26.6 min, and the mean cardiopulmonary bypass time was 115.4±34.3 min.
Early outcomes
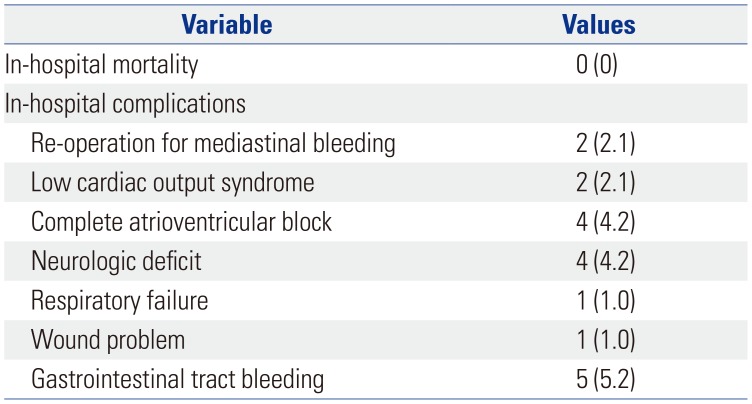
Operative mortality was zero. Two patients underwent reoperation for bleeding (2.1%). Postoperative percutaneous cardiopulmonary support was required for two patients (2.1%) due to low cardiac output syndrome, and four patients (4.2%) required pacemaker insertion due to complete AV block. Four patients (4.2%) had transient ischemic attacks, whereas three patients (3.1%) had permanent stroke. One patient (1.0%) required reintubation due to pneumonia. Table 2 summarizes the perioperative details.
Changes in aortic diameter
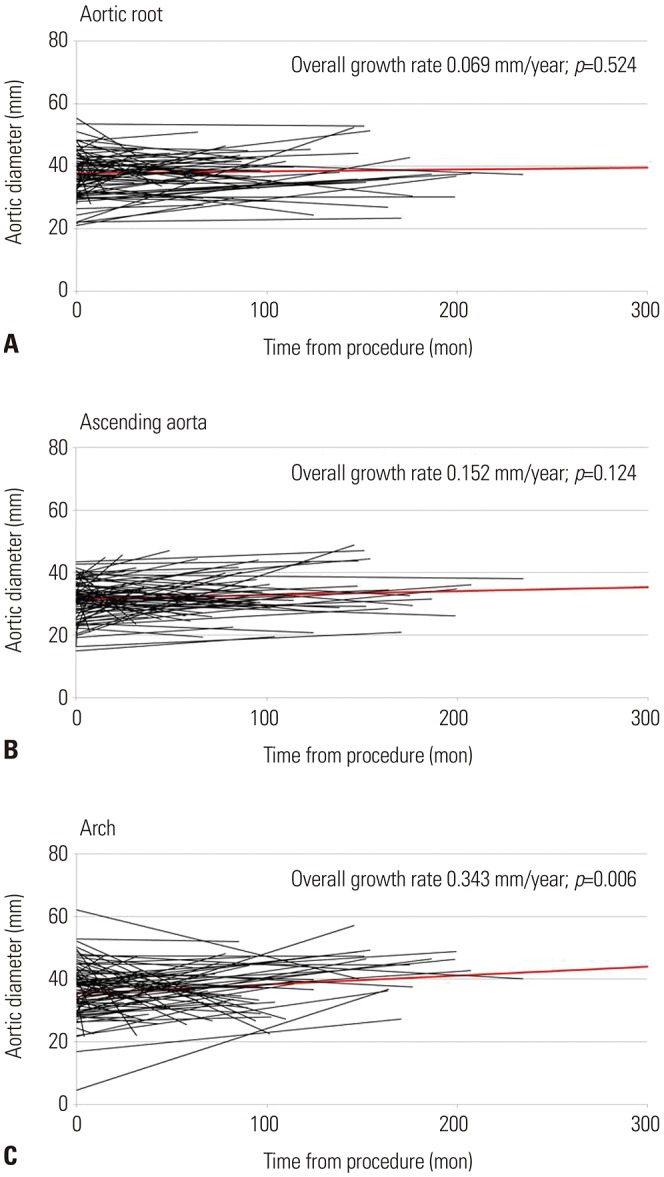
As Table 3 shows, the paired t-test revealed significant differences between aortic diameter measurements immediately after surgery and at the final follow-up (as assessed by CT/echocardiographic analysis) at the level of the proximal aortic arch only (p=0.050). Furthermore, subgroup analysis using LMM indicated that the diameter at this aortic arch level increased over time (p=0.006, Fig. 2).
Sinus of Valsalva
The size of the sinuses of Valsalva maintained stable growth rates of 0.069 mm/year (p=0.524) (Fig. 2). Significant redilation of the sinus of Valsalva was observed for two patients (2.1%). The initial aortic annulus size (p<0.001) and presence of bicuspid aortic valve (p=0.013) were associated with an increase in the size of sinus of Valsalva. However, LMM analysis indicated that these factors did not affect the growth rate over time.
Ascending aorta
Five patients (5.2%) had redilation of the ascending aorta. In these patients, an increase in ascending aorta size of 0.152 mm/year was observed, although this was not statistically significant (p=0.124). The initial sizes of the ST junction and proximal arch significantly influenced the growth rate of the ascending aorta (p=0.021 and p=0.045, respectively). When expressed as change in diameter versus time (Fig. 2), no relationship was apparent.
Aortic arch
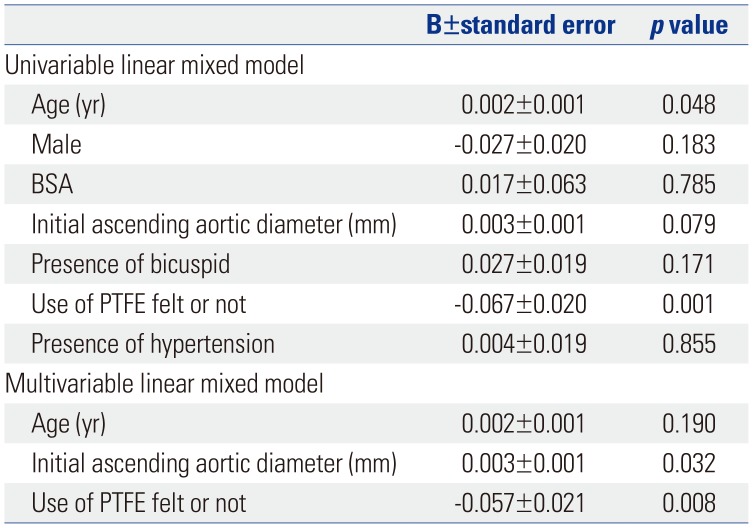
The maximum diameter of the proximal aortic arch increased at a rate of 0.343 mm/year (Fig. 2). Significant redilation of the proximal arch was observed in eight patients (8.3%) (p=0.006). Subgroup analysis of aortic arch diameter increases indicated that there was no significant influence from male sex, body surface area, presence of bicuspid aortic valve, or presence of hypertension on the rate of increase (p=0.183, 0.785, 0.171, and 0.855, respectively). However, age, initial ascending aortic diameter, and the use of PTFE wrapping material had significant effects on the rate of aortic arch dilatation (p=0.048, 0.079, and 0.001, respectively) in the univariable models (Table 4).
Predictors of aortic arch growth were assessed by multivariable LMM. This revealed that initial ascending aortic diameter (p=0.032) and the use of PTFE felt wrapping material (p=0.008) were independent risk factors for increased aortic arch diameter (Table 4).
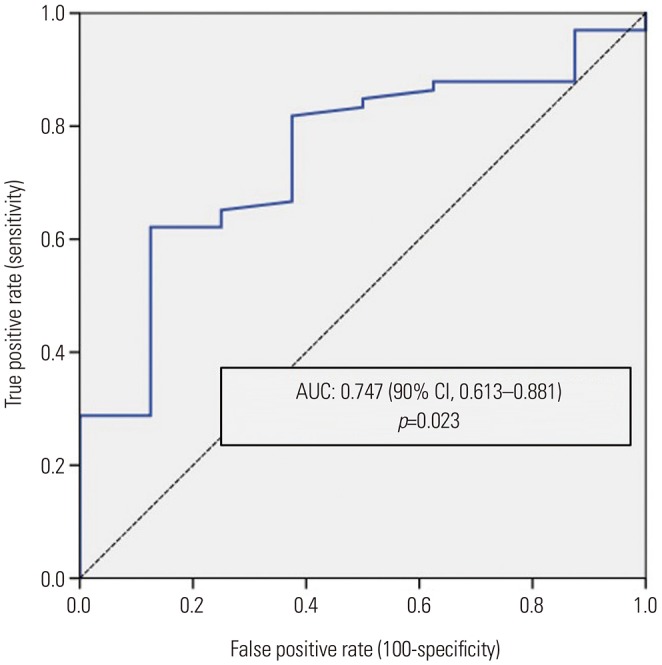
In the ROC curve showing the diagnostic performance of the ascending aorta diameter for re-dilation, and its area under the curve was 0.747, with a 90% confidence interval of 0.613–0.881 (p=0.023) (Fig. 3). An ascending aorta diameter of 46.95 mm could be regarded as the optimal cut-off value for predicted re-dilation of the proximal arch. Overall, freedom from redilation of the proximal aortic arch was 100% and 97.9% after 5 and 10 years, respectively (Fig. 4).
Late outcomes
The maximum follow-up time was 19.5 years, with a median of 9.1 years (mean 8.7±2.1 years). The rate of echocardiogram or CT follow-up was 95.9%. The mean interval period between initial and final follow-up was 7.2±4.6 years. During the follow-up period, aortic root rupture occurred in one patient who underwent aortic wrapping. One patient required aorta-related re-operation (total arch replacement) due to proximal arch dilatation, and transcatheter aortic valve implantation was performed to correct aortic valve dysfunction in one patient at 13 years after AVR surgery.
A total of nine patients (9.4%) died during follow-up, with known cardiac causes in two cases (2.1%). One 53-year-old female patient underwent wrapping, as well as AVR with a mechanical valve. A PTFE felt graft had been used. In this case, redilation occurred 7.8 months after surgery, which developed to aortic root rupture at 7.1 years after surgery. The patient died due to hypovolemic shock caused by mediastinal bleeding. Another patient, a 50-year-old female with underlying lung cancer, died from heart failure due to atrioventricular node dysfunction. During follow-up, the causes of non-cardiac death were as follows: gastrointestinal bleeding in one patient (1.0%), sepsis in two patients (2.1%), and metastatic cancer in four patients (4.2%). Overall survival is illustrated in Fig. 4.
DISCUSSION
In the present study, we found the occurrence of adverse aortic events during long-term follow-up to be rare (2.1%) following ascending aorta wrapping during AVR. The standard treatment for dilated ascending aorta is ascending aorta replacement; nonetheless, surgeons may consider a less invasive alternative of aortic wrapping or no aortic procedure for high-risk patients.
Our results demonstrate that aortic wrapping results in decreased ascending aortic diameter with long-term stability. Over time, dilation of both the ST junction and mid-ascending aorta did increase, although the changes were not statistically significant (p=0.524 and 0.124, respectively). The rate of reoperation of the aorta was therefore very low (2.1%). These results agree with the meta-analysis performed by Plonek11, which reported that significant dilatation of any aortic segment was only observed during follow-up of 12 (1.7%) of the 722 patients and that only 13 (1.8%) required reoperation or reintervention for residual or recurrent aortic pathologies.1213
Ascending aortic wrapping contributed to stabilization of the aortic root with excellent long-term durability, consistent with earlier studies from another institution.141516 Zhang, et al.17 reported that aortic root dilation was slightly increased after replacement, compared with that observed following aortic wrapping. Redilation occurred in areas which were not reinforced or where reinforcement was insufficient, most notably in the noncoronary sinus of Valsalva. In one patient of the present study, significant redilation was observed in the proximal areas of wrapping, including the sinus of Valsalva (p=0.524). Plonek's systematic review supports these results, as the authors found no aortic root enlargement when the external prosthesis was secured by proximal and distal fixation.11
However, aortic wrapping led to a significant increase in the rate of enlargement of the proximal arch (0.343 mm/year, p=0.006). Failure to stabilize the proximal arch may lead to the risk of dilation over time, potentially requiring additional surgery. This risk is particularly high in young patients with a long life expectancy. For this reason, most surgeons prefer to perform ascending aortic wrapping in patients who are over 70 years old or who have a limited life expectancy.14 The enlargement may result from different hemodynamic stresses placed on the proximal arch by the aortic root or ascending aorta. Hemodynamic turbulence is the most common cause of aortic dilation, and aortic valve disease and intrinsic aortopathy are major causes of hemodynamic stress.18 Thus, the present study demonstrates that further expansion at the proximal arch level after correction of the aortic valve may be attributable to intrinsic aortopathy.
We found initial ascending aortic diameter to be a significant risk factor for aortic arch dilatation by multivariable LMM analysis. These results imply that native aneurysmal size is an important index for surgical therapy. Thus, the cut-off value of 47 mm in this study reinforced the current size-based guidelines, in that moderate dilation of the ascending aorta (>45 mm) is a risk factor for redilation.
The wrapping material that is used for ascending aortic wrapping is an important consideration for surgeons. During this study period, we performed concomitant aortic wrapping in 58 patients with PTFE felt and in 38 patients with double-velour vascular grafts. Proximal aortic expansion was significantly correlated with the use of PTFE felt (p=0.008). This result is supported by a study by Randall, et al.,19 who reported a study in which joined carotid arteries were anastomosed to PTFE or double-velour grafts in a canine model. The PTFE grafts showed increased calcification and intimal fibrin deposition microscopically. Therefore, we suggest that double-velour grafts have more acceptable outcomes for wrapping in terms of stabilization of the aorta.
In subgroup analysis, bicuspid aortic valve (n=54, 56.3%) was not found to affect the aortic arch diameter. Although this aortopathy is well known to influence the incidence of aneurysm, it was not found to be a risk factor for aortic redilation after wrapping. In line with this result, the guidelines for repair of bicuspid aortic valve-associated ascending thoracic aortic aneurysms have recently been changed to use the same criteria as for repair of tricuspid aortic valve-associated ascending thoracic aortic aneurysms.20
The present study has several limitations. Firstly, the study population did not include a control group. Secondly, this study was a retrospective analysis of observational data. Thirdly, procedures were selected by the surgeons, and 12 patients with aortic diameters of less than 4.5 cm underwent aortic wrapping owing to aortic wall enforcement. Recent changes in the guidelines with respect to American College of Cardiology/American Heart Association (AHA) criteria currently specify that the indication for ascending aortic aneurysm associated with bicuspid valve is 5.5 cm. Therefore, this study may differ from current recommendations. Lastly, there was a lack of quantitative data concerning the phenotype of the ascending aorta, such as fusiform or saccular aneurysms. Not all patients were able to be assessed with CT at the final follow-up. Some aortic size measurements were carried out using transthoracic echocardiographic assessment, which is not the gold standard method for aortic evaluation. The limited modality of echocardiographic and CT follow-up is therefore an important limitation of this study.
The number of mortalities or patients with redilation was too small to evaluate the surgical risks with appropriate statistical power. Therefore, the safety and durability of aortic wrapping should be addressed in further studies using larger populations over longer durations.
Aortic wrapping led to stabilization of the dilated aorta, with excellent long-term durability. In this study, the diameter of the proximal arch increased over time in patients with an ascending aortic diameter of over 47 mm. Therefore, the results of this study suggest that redilation of the proximal arch should be carefully observed during long-term follow-up after aortic wrapping surgery. Further large-scale prospective trials are required to define appropriate indications for concomitant aorta wrapping during AVR.



 XML Download
XML Download