

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular diseases (CVDs) are the leading cause of death (about 30% of deaths)1 worldwide. In Korea, CVDs carry the second highest death rate following cancer, and the recent trend is increasing.2 Most countries have surveillance systems and annually investigate current death statistics owing to its importance. However, data on the incidence of CVDs other than that from mortality rates are lacking because it is more difficult to detect incidence of CVDs than to assess the death rate due to CVD among the total population, and the cost for investigation is also high.
Many countries, including the Asian countries, have reported on recent trends (since 2010) in the incidence rate of CVDs.3456789 However, there has been little research on the incidence of CVDs in Korea since 2010.10 Therefore, there is a lack of accurate data on the recently increased CVD mortality in Korea and limitations in establishing and evaluating policy strategies for CVDs.
In Korea, the entire population is covered by the National Health Insurance Service (NHIS), which manages all medical utilization and claims data. Recently, the NHIS disclosed medical insurance claims data of the Korean population for research purposes, which can help identify the disease name, type of examination, and treatment, as well as the medical institution where treatment was obtained. Therefore, these data can be used to confirm the incidence of CVDs, especially acute myocardial infarction (AMI). Furthermore, as data from the year 2002 have been released, the trend in the long-term AMI incidence can be evaluated.
In this study, using medical insurance claims data, we investigated the 10-year trend between 2007 and 2016 in the incidence of AMI in patients who received in-hospital treatment and analyzed the regional AMI incidence to explain the regional AMI mortality disparity. Additionally, the AMI case-fatality after hospitalization was determined.
METHODS
Data sources
Data used were from the NHIS claims data. This data is a cohort from 2002 of the medical utilization of all Koreans, which is about 50 million. Data include information such as the type of medical institutions, date of visit, duration of admission, International Classification of Diseases (ICD)-10 code for treated diseases, and type of treatment including procedures and medications. Socio-demographic information such as gender, age, and residence province are also included. In case of death of the insured, the date and cause of death are included by using linked Statistical Office mortality data. The NHIS data usage procedures are shown in Supplementary Table 1.
In this analysis, we used 15 years of medical utilization data from 01 January 2002 to 31 December 2016. Data from 2002 to 2006 (5 years) were used as a washout period to define newly diagnosed patients and to exclude these patients in subsequent years for identification of new cases from 2007 to 2016.
Identification of newly diagnosed AMI
In the NHIS claims data, there are no records of symptoms, electrocardiogram (ECG) findings, or results of cardiac biomarker tests. Therefore, we identified patients with newly diagnosed AMI based on the following steps.
First, for the period from 2007 to 2016, patients diagnosed with AMI (ICD-10 code: I21.0–I21.9) in the main diagnosis code or in the four sub-diagnosis codes were identified by each year. Second, among the identified patients, those diagnosed with AMI between 2002 and the previous year of the year diagnosed were excluded from the incidence cases. For example, a 2007 incidence patient was never diagnosed between 2002 and 2006, and incident patients at 2013 were never diagnosed between 2002 and 2012. In addition, patients with 1-day duration of admission were excluded. Third, among patients who met the first and second conditions, those who fulfilled two or more of the following three conditions were analyzed for the incidence of AMI: 1) Patients who underwent a MB fraction of creatine kinase or troponin tests at admission; 2) those who underwent a coronary artery angiography or percutaneous coronary intervention (PCI) or thrombolysis or coronary artery bypass grafting (CABG); and 3) those prescribed antiplatelet agents such as aspirin or clopidogrel.
In the NHIS claims data, all tests, procedures, treatments, and drugs are coded. Therefore, the corresponding code was checked and retrieved to extract the patient data, and the detailed code has been summarized in Supplementary Tables 2 and 3.
Analysis of outcomes
From 2007 to 2016, the crude incidence rate was calculated by dividing the number of patients in each year by the mid-year population. Also, we calculated the incidence rate by gender, age groups (0–29, 30–39, 40–49, 50–59, 60–69,70–79, and over 80 years), and 17 regions (8 metropolitan cities and 9 provinces) of Korea based on the patient residence. The age standardization incidence rate was calculated to compensate for the difference in the proportion of the population between the age groups by year. At this juncture, we set the standard population to the mid-year population in 2011, and the calculation formula used was as follows.
Age-standardized incidence rate (per 100,000 person-years) for each year = Σ (incidence rate by age groups at each year × number of standard population by age groups) × 100,000/total number of standard population.
To summarize the incidence over the entire period and to compare the incidence rates between the 17 regions easily, we calculated the average incidence rate (per 100,000 person-years) during the study period by the following formula.
Average age-standardized incidence rate (per 100,000 person-years) during 10 years = Σ (incidence rate by age groups during 10 years × number of standard population by age groups) × 100,000/total number of standard population.
In the case of the Sejong province which is a new administrative region in 2012, we calculated the average age-standardized incidence rate during four-years.
We calculated the 7-days, 30-days, 90-days, 1-year, and 3-years all-cause case-fatality (%) from the date of admission for AMI by dividing the cumulated number of deaths for each period by the total number of AMI patients for each year. The 3-years case-fatality of 2014, 2015, and 2016, and the 1-year case-fatality of 2016 were not calculated to avoid misleading values due to underestimation.
We used SAS version 9.4 (SAS Institute, Cary, NC, USA) for all analyses, and we did not use any statistical testing method because data of the entire population was used instead of a sample data. The figures in this study were plotted by using R software version 3.5.2 (R Foundation for Statistical Computing, Vienna, Austria) with package ‘ggplot2.’ The map geometric shape file was downloaded from the website of GIS developer (http://www.gisdeveloper.co.kr/?p=2332).
Ethics statement
This study was an analysis of secondary data from the NHIS. The data set did not include any personal information such as patient name, social security number, address, or phone number. Only non-identifiable aggregate results that were openly available for public research purposes were released and informed consent could not be obtained. The present study protocol was reviewed and approved by the Institutional Review Board of Gyeongsang National University Hospital (approval No. GNUH 2018-05-017).
RESULTS
Incidence rate of hospitalized AMI
We identified 214,646 patients who were newly hospitalized with AMI enrolled from the Korean NHIS data for the period between 2007 and 2016. Of the total patients, 67.8% were men, and the proportion of men patients was seen to steadily increase from 62.4% (2007) to 70.5% (2016) (Table 1).
Table 1
Annual incident cases and incidence rate of hospitalized acute myocardial infarction
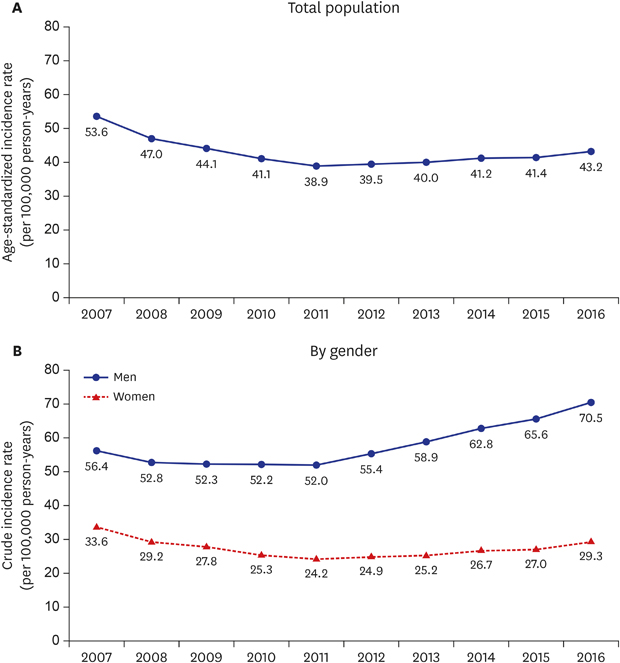
The age-standardized incidence rate of hospitalized AMI decreased from 53.6 cases per 100,000 person-years in 2007 to a lowest of 38.9 cases per 100,000 person-years in 2011 (relative decrease between 2007 and 2011, 27.4%). Following this, the age-standardized incidence increased steadily to 43.2 in 2016 (relative increase between 2011 and 2016, 11.1%) (Table 1 and Fig. 1). This trend of AMI incidence which showed a decrease until 2011 and then increased till 2016 was similar in both the genders and all age groups. The age group with the highest incidence was 80+ years during the whole period (Table 1).
Fig. 1
Trend in incidence rate of hospitalized acute myocardial infarction between 2007 and 2016. (A) Age-standardized incidence rate of total population. (B) Crude incidence rate by gender.

We found a marked difference in the average age-standardized incidence rate of hospitalized AMI over 10 years among the 17 administrative regions in Korea (Fig. 2). Daegu, Jeju, and Gwangju Province showed the highest average AMI incidence rates of 50.3, 47.3, and 47.1 per 100,000 person-years, respectively. On the other hand, Sejong, Chungnam, and Incheon Province showed low average incidence rates of 30.2, 37.9, and 38.4 per 100,000 person-years, respectively. The highest incidence rate of Daegu city was relatively 66.6% higher than that of the lowest Sejong city. The annual age-standardized incidence rates of the 17 regions from 2007 to 2016 are shown in Supplementary Table 4.
Fig. 2
Average age-standardized incidence rate (per 100,000 persons-year) of hospitalized acute myocardial infarction by 17 regions of Korea during 10 years. The color of the map was represented by gradations from blue to green. The regions with higher incidence rates were painted in blue, while those with lower were painted in green.
SE = Seoul, BS = Busan, DG = Daegu, IC= Incheon, GJ = Gwangju, DJ = Daejeon, US = Ulsan, SJ = Sejong, GG = Gyeonggi, GW = Gangwon, CB = Chungbuk, CN = Chungnam, JB = Jeonbuk, JN = Jeonnam, GB = Gyeongbuk, GN = Gyeongnam, JJ = Jeju.

Case-fatality of AMI patients
Over 10 years, the 7-days, 30-days, 90-days, 1-year, and 3-years cumulated average case-fatality of all the hospitalized AMI patients was 3.2%, 6.9%, 9.9%, 14.7%, and 22.4%, respectively (Fig. 3). In 2007, the 7-days, 30-days, 90-days, 1-year, and 3-years cumulated case-fatality of all the hospitalized AMI patients was 3.5%, 8.0%, 11.6%, 17.3%, and 25.0%, respectively. Since then, the all-period cumulated case-fatality has decreased gradually, and in 2016 the case-fatality was 2.8%, 6.2%, 8.8%, 13.1% (in 2015), and 19.7% (in 2013), respectively (Fig. 3). The all-period case-fatality of women was relatively higher by about 72% to 92% than that of men (Table 2). However, the decreasing trend of case-fatality from 2007 to 2016 was similar in both the genders (Table 2). The annual case-fatality by age groups has been shown in Supplementary Table 5.
Fig. 3
Case-fatality of hospitalized acute myocardial infarction by period from admission between 2007 and 2016. The 1-year or 3-years case-fatality of 2014, 2015, or 2016 patients could not be calculated or may be underestimated. We did not represent this data to avoid confusion and misleading.
Table 2
Annual case-fatality after diagnosis of acute myocardial infarction by gender
DISCUSSION
Although mortality and case-fatality of AMI has been reported from several registries and monitoring data, this study is the first to report on the incidence of hospitalized AMI in Korea using the entire population medical utilization cohort data from 2007 to 2016. The average total annual incidence was 21,465 cases. The average crude incidence rate during the whole period was 42.8 per 100,000 person-years (men 57.9 and women 27.3). The age-standardized incidence rate for AMI showed a decreasing trend from 2007 to 2011 and a slightly increasing trend from 2011 to 2016. However, all-period case-fatality in hospitalized AMI patients showed a decreasing trend between 2007 and 2016. We also found that the region with high age-standardized mortality due to ischemic heart disease was highly associated with the region with high age-standardized AMI incidence in Korea.
Although the pattern of decrease and increase in the incidence rate of AMI over the last 10 years may reflect the actual AMI incidence, careful consideration should be exercised in interpreting these data.
First, the diagnosis of AMI diagnosis was influenced to a large extent by the sensitivity of cardiac markers such as troponin I and T. Following the development of radioimmunoassays to detect serum troponin in the 1990s,11 cardiac troponin (cTn) assays have been used to diagnose myocardial infarction. However, since 2010, highly sensitive cTn (hs-cTn) assays have been developed and widely used.1213 In fact, among patients with suspected AMI, those tested by the hs-cTn assay were diagnosed to have AMI more often (22% higher) than those tested by the cTn assay.14 Particularly, the hs-cTn assay had a higher sensitivity than that of the cTn assay and contributed to the increasing diagnostic rate of type I AMI and to the decreasing diagnostic rate of unstable angina.14 In addition, the development of rapid diagnostic kits in the middle of the decade 2001–2010 helped in a quick diagnosis in the emergency room rather than in the laboratory1516 and may have contributed to the increase in the incidence rate of AMI.
Second, the definition and the diagnostic criteria of AMI have been changed in the 1950s.17 Thus, the incidence of AMI may be affected by the changed diagnostic criteria. The main points of change in the diagnostic criteria of AMI occurred in 2000, 2007, and 2012. In 2000, the task force of the European Society of Cardiology and the American College of Cardiology changed the definition of AMI using a biochemical and clinical approach that demanded an elevation of cardiac biomarkers before myocardial infarction could be diagnosed rather than the traditional epidemiological approach.18 After the new definition of AMI was introduced, the numbers of AMI patients increased.19 In 2007, the same task force redefined AMI, with less emphasis on ECG and symptoms and more meaningful implications for cTn than that in the 2000 definition.192021 They also introduced the new AMI diagnostic classification system with five subcategories.20 According to the study which analyzed the incidence difference between the diagnostic criteria in the same patient data, the incidence based on the 2007 criteria was about 11% lower than that based on the 2000 criteria.21 Therefore, it can be explained to some extent that the incidence rate has been continuously decreasing from 2007 as seen in our results. In 2012, a third definition for AMI was published. The most prominent changes in the third definition cover the distinction between myocardial ischemia and myocardial injury (or cardiac others) and the third criteria define AMI in the setting of cardiac interventions such as PCI and CABG.1922 Because of this change, the patients who were actually diagnosed to have other cardiac conditions such as myocarditis, Takotsubo cardiomyopathy, or tachyarrhythmias were classified as type 2 AMI according to the 2012 definition, which resulted in a 6% incidence increase than that by the 2007 definition.23
Therefore, it can be inferred that the improvement in the analytic performance of troponin assays and the change of definition for AMI are among the causes for the trend seen in the incidence rate. Our inference is convincing because recent trends in the incidence of AMI in other countries6782425 tend to be similar to that seen in this study. Some studies have shown a large decrease in the incidence rate before 2010 or 2011; however, thereafter the incidence rate has shown a relatively small decrease or has remained steady.345 Studies from Singapore,6 Poland25 and Japan8 have reported a slight increase in the rates again from 2011, like in this study. Despite the effect of introduction of hs-cTn and the new definition of AMI, Korean health providers should change the preventive strategies to decrease the incidence of AMI as it has remained steady since 2011.
Statistics Korea death data26 showed marked disparity in CVD mortality by regions in Korea, with the south-eastern areas of Korea such as Daegu, Gyeongbuk, Gyeongnam, and Busan showing a remarkably high mortality for CVD. We first found the disparity in the average age-standardized incidence rates (lowest 30.2 to highest 50.3 per 100,000 person-years) between regions. On comparing these results with the Statistics Korea death data,26 in general except on Jeju, the regions of high AMI incidence tended to have higher ischemic heart disease mortality and the regions of low AMI incidence tended to have lower ischemic heart disease mortality. In Jeju, the reason for the low ischemic heart disease mortality compared to the high AMI incidence cannot be known exactly. However, based on Statistics Korea data (http://kosis.kr/index/index.do), we assume that generally in Jeju compared to other regions, the higher public ambulance utilization and faster emergency room visits after AMI symptoms may be the reason (Supplementary Table 6 and Supplementary Fig. 1).
These results suggest that the high mortality rates in the region are not a consequence of the regional hospital care system, but of the incidence of the disease per se. Therefore, it is necessary to first prevent the incidence of myocardial infarction in order to reduce the mortality rate.
The trend for all-period case-fatality in hospitalized AMI patients showed a decrease from 2007 to 2016. This declining trend was the same shown in other recent studies.272829 This decrease can be explained by improvements in healthcare facilities and therapeutic technologies such as medical devices and medicines. Additionally, since 2011, the cardiovascular intervention institute/specialist certification system has been implemented to provide prompt and appropriate treatment for AMI patients in Korea. As a result, the proportion of initial PCI procedures has increased steadily (99.1% in 2018) till recent years, and the door-to-balloon time has been relatively reduced, about 60 minutes.29 Moreover, because the government has promoted awareness and education about the early symptoms of AMI from the late 2000s, the symptoms-to-door time has also shown a gradual decrease.29 The proportion of ST-elevation myocardial infarction (STEMI) patients is markedly continuing to decrease compared to that of non-STEMI (NSTEMI) patients. These factors may contribute to the decrease in the case-fatality of hospitalized AMI patients over 10 years. The case-fatality was much lower in men than in women, because women patients were older than the men patients, and the higher the age, the higher the case-fatality in patients.
This study has several limitations as we have used NHIS data which include medical utilization cohort data for 15 years. The insurance claims data do not have information on symptoms, ECG records, and laboratory results, and the diagnostic accuracy is also low. In a study comparing hospital clinical data with NHIS data, the diagnostic accuracy for all diseases was 69.7%.30 However, the diagnosis of an acute phase disease such as AMI is more accurate. We believe that the diagnostic accuracy was not a significant limitation in our study, because we considered the duration of admission, type of diagnostic test, procedures for treatment, and the use of antiplatelet drugs besides the AMI diagnostic code. Second, there is the limitation that the incidence of AMI at a population level may be underestimated because AMI cases who did not visit hospitals and died directly on the site are not included in the NHIS data. Also, the incidence and case-fatality may be underestimated because those who died within a day after arriving at the emergency room were excluded. However, this study focused on the incidence of hospitalized AMI, and not on the total population incidence of AMI. In addition, when calculating the AMI incidence rate in NHIS data, the results may vary under different conditions. That is, depending on how a combination of conditions, such as diagnosis code, laboratory code, procedure code, and medication code, the result may vary. Therefore, when interpreting this study, it is necessary to focus on the 10-years trend rather than on the absolute values of AMI incidence. Third, in this study, differences in incidence rates by region were calculated. Among the causes of regional differences, there may be a difference in incidence due to differences in diagnostic criteria of medical doctors in different regions. However, in this study, the analysis was made on the assumption that the diagnostic criteria of medical doctors in Korea are similar. Finally, we did not analyze the AMI by subgroups into STEMI and NSTEMI, and did not separate all-cause fatality and cardiovascular fatality. Because it was difficult to distinguish the type of AMI and cause of death from the NHIS claims data. Therefore, it is necessary to pay attention to the interpretation of data results, and it is necessary for further research to separate the types of AMI and the causes of death.
Despite these limitations, the strength of this study was confirmation of the relatively long-term trends in the AMI incidence rate for the entire population of Korea. Another strong point of this study was the analysis of the difference in the AMI incidence rate by regions to reveal the causes for the difference in AMI mortality in Korea. In addition, it is meaningful that this study analyzed not only the 7-days and 30-days case-fatality of AMI, but also the case-fatality for the extended period of 90 days, 1 year, and 3 years.
In conclusion, the incidence rate of hospitalized AMI in Korea decreased from 2007 to 2011 and then tended to increase gradually until 2016. Moreover, there was a difference in the incidence rate of AMI between the 17 regions of Korea. Finally, the all-period case-fatality of AMI patients has shown a steady decrease from 2007 to 2016.
 XML Download
XML Download