

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
β-Lactam antibiotics, including penicillin and cephalosporin, are highly effective against bacteria and are among the most widely prescribed drugs globally. Unfortunately, they can provoke hypersensitivity reactions. Cephalosporins, which are now most widely used β-lactam antibiotics, can also cause hypersensitivity.12 However, there is no standard method of predicting hypersensitivity to cephalosporins; in contrast, penicillin skin tests are useful for patients with a history of hypersensitivity to penicillins.34 Provocation tests are usually recommended to predict the risk of β-lactam hypersensitivity only for those with a history of hypersensitivity to β-lactams.56 However, the relationship between hypersensitivity to cephalosporins and a history of hypersensitivity to β-lactams is unclear.278 Only 30% of subjects with a history of hypersensitivity to β-lactams are indeed allergic based on diagnostic test results.9 Also, many patients have a history of hypersensitivity to unknown medications.
In most hospitals in Korea, screening intradermal cephalosporin skin tests are performed routinely for all patients who need cephalosporins, irrespective of any history of β-lactam hypersensitivity.10 Such intradermal skin screening tests typically involve one fixed concentration and no negative control.10 Antibiotics are the most common triggers of drug-induced anaphylaxis in European countries,111213 but antibiotic-related anaphylaxis is less frequent in Korea, where radiocontrast medium is the leading cause of drug-induced anaphylaxis.14 Could routine screening intradermal cephalosporin skin tests explain the lower frequency of antibiotic-induced anaphylaxis in Korea?
This retrospective study evaluated the usefulness of routine intradermal cefazolin skin screening tests without negative controls in Korea. We also evaluated the relationship between skin test positivity and a history of suspected β-lactam hypersensitivity. We applied cefazolin, a first-generation cephalosporin commonly recommended for prophylactic use before surgery.8
METHODS
Subjects
The medical records of patients who underwent cefazolin skin testing between January 2010 and January 2011 at Seoul National University Bundang Hospital, Korea were evaluated.
Study design
Cefazolin skin tests were performed by regular ward nurses. Cefazolin was diluted to 0.3 mg/mL in normal saline and 0.02 mL was injected intradermally; the results were interpreted after 15–20 minutes. A positive skin test result was defined as a flare ≥ 15 mm or wheal ≥ 5 mm.1015
Cefazolin skin testing was performed without a negative control, as described previously.1016 However, in some patients with a positive cefazolin skin test result, normal saline skin tests were performed as negative controls, as done for cefazolin. Also, graded challenges, i.e., slow administration of cefazolin mixed with 50–100 mL of normal saline, were conducted for some patients.
Nurses inquired regarding the history of drug hypersensitivity reaction in all patients and the causative medications were recorded as accurately as possible based on the statements of the patients. The history of drug hypersensitivity reactions was re-evaluated by the allergy specialist; ‘allergy to β-lactam’ included ‘penicillin allergy,’ ‘cephalosporin allergy,’ and cases in which the patient could only remember the name ‘β-lactam.’ ‘Allergy to suspected antibiotics’ indicated that antibiotics could not be ruled out as causative agents (e.g., ‘pyrine allergy,’ ‘sulfa allergy,’ ‘mycin allergy,’ ‘unknown drug,’ ‘drug for common cold,’ and ‘unknown antibiotics’), and included cases in which patients could remember the name of non-β-lactam antibiotics. Cases involving ‘anti-epileptics,’ ‘anti-pyretics,’ and ‘pain killers,’ and those in which the patients could remember the name of drugs other than antibiotics, were excluded.
To detect cases with immediate adverse reactions after cefazolin injection, key words including urticaria, itching, hypersensitivity, and anaphylaxis (within 3 days of initiation of cefazolin usage) were searched for in the electronic medical records and the consultation documents of allergy specialists or dermatologists. Cases with immediate adverse reactions after cefazolin injection were identified by an allergist through review of the medical records. Hypersensitivity reactions were diagnosed based on the temporal relationship between cefazolin injection and typical symptoms such as urticaria, rash, itching, and anaphylaxis; cases involving factors that could mimic hypersensitivity, such as use of radiocontrast dye or transfusion, were excluded.
RESULTS
Baseline characteristics
Over the 13-month study period, 13,153 cefazolin skin tests were performed (Table 1) on 11,857 patients (1,153 patients underwent cefazolin skin testing twice or more over the 13 months). There were 4,939 men patients (41.7%). The mean (range) age was 48.75 years (range, 3–99 years). The number of patients with a history of allergy to β-lactams (n = 40) and suspected antibiotics (n = 69) was 109 (0.8%) (Table 2). Four of those patients had a history of prior positive responses to antibiotic skin tests (three to cephalosporin, one to an unknown antibiotic) but had not used those antibiotics.
Table 1
Baseline characteristics of the patients

![]()
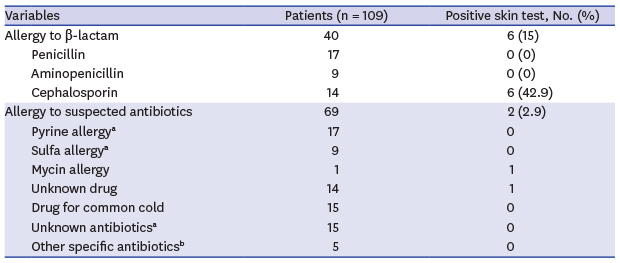
Table 2
History of adverse drug reactions based on the statements of patients
aIncluding patients with a history of multiple drug adverse reactions; bAntibiotics other than β-lactams.
![]()
Negative cefazolin skin test
Among the 12,969 cases with a negative skin test result, 8 showed immediate hypersensitivity to cefazolin (0.06%) according to a retrospective review of the electronic medical records using key words, and the nursing chart and consultation documents for allergic reactions. Those eight cases showed urticaria, rash, and itching. The negative predictive value of cefazolin skin testing alone was 99.94%.
Positive cefazolin skin test
The number of cases with a positive skin test result was 184 (1.4%). Of the cases with a history of allergy to β-lactams, 15% (6/40) had a positive skin test result; 5 had a history of cefazolin allergy and 1 a history of cephalosporin allergy (Table 2). Of the cases with a history of allergy to cephalosporin, 42.9% (6/14) showed a positive skin test result, while none (0/26) of the cases with a history of allergy to penicillin or amino-penicillin showed a positive skin test result. All five cases with a history of cefazolin hypersensitivity showed positive results in routine skin tests. In contrast, 1.35% (178/13,113) of the cases without a history of allergy to β-lactam antibiotics showed positive results (P < 0.001).
Among the 1,153 cases who underwent cefazolin skin testing more than twice over the 13 months, none showed a consistently positive response to cefazolin, but 21 cases (1.8%) showed inconsistent positive responses; none had a history of allergy to antibiotics. Of the cases, 98.2% showed consistently negative results in multiple cefazolin skin tests. Furthermore, among the cases with a positive cefazolin skin test, 19 also underwent normal saline skin tests; 14 (73.4%) showed a false-positive skin test to normal saline.
The management approach applied to patients with positive cefazolin skin tests is detailed in Table 3. Graded challenges with cefazolin were performed in 10 patients; none exhibited a hypersensitivity reaction. Table 4 shows the alternative antibiotics administered to patients with positive cefazolin skin test results. Among the 17 patients who received other β-lactams, there were no hypersensitivity reactions to the alternative β-lactams. The most common alternative antibiotics were quinolones (123 cases, 72.8%). All of the patients with a history of suspected hypersensitivity to antibiotics used quinolones.
Table 3
Management of cases with a positive cefazolin skin test

| Variables | Positive cefazolin skin test (n = 184) |
|---|---|
| Alternative antibiotics | 169 (89.1) |
| Graded challenge with cefazolin | 10 (5.4) |
| No use of antibiotics | 5 (2.7) |
![]()
Table 4
Alternative antibiotics for patients with a positive cefazolin skin test

![]()
DISCUSSION
We identified 13,153 cefazolin skin tests performed over the 13-month study period. Among the 12,969 cases with negative results, 8 had immediate hypersensitivity to cefazolin (0.06%). The overall positivity rate of cefazolin skin tests was 1.4%. Among the 40 cases with a history of allergy to β-lactam antibiotics, 15% (6/40) showed positive results.
The negative predictive value of the intradermal cefazolin skin screening test was 99.94%. There were no reports of severe anaphylactic reactions among 12,969 cases of cefazolin usage, with the exception of 8 cases of urticaria or rash with itching. However, the overall incidence of anaphylactic reactions from cephalosporins is low (0.0001%–0.1%).2171819 A large prospective study is needed to evaluate the ability of routine cephalosporin skin screening tests to prevent severe anaphylaxis in the general population. However, the efficacy of such a program would likely be insufficient based on the low incidence of cephalosporin-induced anaphylaxis. Because severe cefazolin hypersensitivity is rare in the general population, the positive predictive value is more important than the high negative predictive value of intradermal cefazolin skin screening tests.
A positive formal cefazolin skin test, using controls and appropriate drug concentrations, should be considered a risk factor for cefazolin hypersensitivity. However, many false-positive routine intradermal cefazolin skin tests (without negative controls) were identified. Graded challenge tests with cefazolin were negative in 10 patients with a positive cefazolin skin test while 21 patients who underwent cefazolin skin testing more than twice during study period showed inconsistent positive response. Furthermore, 14 (73.4%) of the 19 patients who had positive saline skin test results (negative control) were shown to have dermographism. The high frequency of dermographism (6.7%) in Korea,20 and the lack of a negative control, suggest that there could be many false-positives due to dermographism. Additionally, false-positive routine cefazolin skin tests not only cause unnecessary pain and waste medical resources, but also increase the usage of alternative antibiotics and the number of patients with a false history of allergy to antibiotics based only on skin tests. Therefore, routine skin tests that lack negative controls are not predictive of severe allergic reaction to cefazolin, consistent with previous reports. In individuals with a history of β-lactam allergy, attempts to develop a skin test for allergy to cephalosporins have been unsuccessful and skin testing with the native drug alone has little predictive value.1921 For those without a history of β-lactam allergy, Yoon et al.22 reported that a routine cephalosporin skin screening test is not predictive of immediate hypersensitivity because of the extremely low sensitivity and positive predictive value. Recently, Yang et al.16 reported that routine intradermal skin screening tests for the general population showed no clinical efficacy for cephalosporin-induced anaphylaxis, irrespective of any history of β-lactam allergy.
The incidence of a positive skin cefazolin test was sevenfold higher in subjects with a history of β-lactam hypersensitivity than in those with no such history. This finding suggests that that a routine cefazolin skin screening test may predict the risk of immediate hypersensitivity in some patients with a history of hypersensitivity to β-lactams. Although neither provocation tests nor negative controls were used in the analysis of patients with a history of β-lactam hypersensitivity who showed positive skin test results, there may be many false-positives among them based on the findings of the patients with no such history. Therefore, cefazolin skin testing using controls and appropriate drug concentrations should be considered. The sensitivity of formal cephalosporin skin testing was 31%–70% in patients with immediate reactions to cephalosporins.232425 Therefore, a provocation test is needed to confirm the diagnosis of β-lactam allergy and is a requirement in patients with a suspected drug allergy.26
Among the patients with a history of allergy to β-lactams, cefazolin skin tests were positive in patients with a history of hypersensitivity to cephalosporin, but not penicillin. Although the history of hypersensitivity to β-lactams has been regarded as a risk factor for cephalosporin hypersensitivity due to possible cross-reactivity between them, actually there have been little evidence to do screening tests for cephalosporin hypersensitivity based on the history of hypersensitivity to penicillin.278 Post-marketing studies of second- and third-generation cephalosporins showed no increase in allergic reactions in patients with a history of penicillin allergy.2 In contrast, Lin reported in 1992 that 8.1% of patients with a history of penicillin allergy had reactions to cephalosporin, compared to 1.9% of those with no such history.7 Moreover, as various antibiotics are used clinically, it is difficult to evaluate the history of hypersensitivity to specific drugs. It is reported that 80%–95% of patients with a history of penicillin allergy will have a negative penicillin skin test result.8 Our data suggest that selecting candidates for cefazolin hypersensitivity screening tests based on the history of cefazolin or cephalosporin allergy might be useful in clinical practice.
This retrospective study had some limitations that should be considered. First, the concentration of cefazolin and criteria for a positive skin test result were based on real practice in one hospital in Korea. This study used a cefazolin concentration of 0.3 mg/mL, which was low enough to avoid non-specific irritant reactions; Empedrad et al.27 reported that 33 mg/mL cefazolin does not irritate the skin and the ENDA/EAACI Drug Allergy Interest Group recommended 2 mg/mL for cephalosporin skin tests.21 A positive skin test in this study was defined as a flare ≥ 15 mm or wheal ≥ 5 mm, in contrast to a wheal > 5 mm with surrounding erythema in the prior study21; this could explain the false-positive cefazolin skin test results. The routine screening skin test protocol was based on that used in most hospitals in Korea.10 Second, it is possible that the incidence of allergic reaction was underestimated because the data were obtained by searching the electronic medical records for key words. Also, we did not include a validation set in the search protocol. However, severe anaphylactic reactions are unlikely to be missed during screening of electronic medical records. Third, a confirmative case-control study is needed because of the different numbers of cases with (n = 40) and without (n = 13,113) a history of allergy to β-lactams; the positivity rate was around 1% in one group. A well-designed confirmative study was not possible due to the limitations of retrospective studies, such as the limited quantity of clinical information for potential matching variables.
In conclusion, the negative predictive value of the intradermal cefazolin skin screening test (0.3 mg/mL) was 99.94%, while the positivity rate was 1.4% overall but 42.9% for patients with a history of cephalosporin use. Considering the low incidence of cefazolin anaphylaxis and the possibility of false-positive results, it is doubtful whether routine screening skin tests without a negative control are useful for predicting severe cefazolin hypersensitivity. However, the high incidence of positive results among patients with a history of cephalosporin hypersensitivity suggests that careful evaluation of the history of drug allergy is important, as well as a role for routine cefazolin screening skin tests for such patients (although a large prospective study is needed to confirm this). Considering the possible false-positive results and limited sensitivity of skin tests, graded cefazolin challenge may be needed for patients with a history of cephalosporin hypersensitivity.
 XML Download
XML Download