

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pre-diabetes is a health status that means blood sugar level is higher than normal, but not yet high enough for a diagnosis of diabetes. The blood sugar range for pre-diabetes is 100~125 mg/dL and the hemoglobin A1c range is 5.7~6.4% [1]. In addition to an increasing prevalence of diabetes, the pre-diabetic population is expected to include more than 470 million people by 2030 [2]. The death rate associated with diabetes is increasing every year [3], and individuals who are pre-diabetic are at high risk for development of diabetes, with an annualized conversion rate of 5~10%[24]. Individuals with prediabetes are at high risk, not only for transit to Diabetes Mellitus (DM) but also for Cardiovascular Disease (CVD) in their later lives [3].
For women, physiological aging and changes begin at middle age, and decreased activity leads to a higher risk of diabetes because of increased insulin resistance [456]. Fasting insulin and blood glucose levels were higher in postmenopausal women than in premenopausal women. Menopause was also associated with the selective accumulation of fat in the abdominal cavity, resulting in increased abdominal obesity [456]. Obesity and central obesity are the most prominent risk factors in the prevalence of diabetes, which is more distinct in women. The increase in obesity after middle-age in women increases their incidence of diabetes. However, men have increased obesity and diabetes at a younger age but a lower incidence than women after middle age [7]. As the prevalence of diabetes is increasing, there is a need to explore determinants beyond the traditional risk factors, for example, sedentary behavior and obesity [8]. In particular, pre-diabetes is related to visceral obesity, high triglycerides, low level of High-Density Lipoprotein (HDL) cholesterol, and hypertension [9]. Therefore, specific health care is needed to prevent problems associated with pre-diabetes in middle-aged women.
In a prior study, risk factors linked with undiagnosed diabetes and pre-diabetes were investigated using multiple logistic regression, and the overall prevalence of diabetes and pre-diabetes was found to be 6.6% and 16.6%, respectively [10]. According to the World Health Organization's (WHO) STEPwise Approach to Risk Factor Surveillance (STEPS) study in Palau of 1,915 adults aged 25~64 years, middle-aged adult, hypertension, hypertriglyceridemia, and central obesity, which includes a large waist circumference or waist-hip ratio, were identified as predictors of diabetes [11].
Middle-aged women in particular undergo hormonal changes related to menopause [7] and display signs of aging, as well as a decline of physical functioning of all organs. This results in decreased opportunity for physical activity, excessive calorific intake, and loss of balance in energy consumption, and therefore they experience increased body weight and complications such as obesity [612]. In a systematic review, women were found to have a higher Body Mass Index (BMI) than men [13], and women with pre-diabetes are more likely than men to develop diabetes mellitus [7]. Additionally, in West Asia, women aged 40~55 years showed significantly higher BMI and Waist-to-Hip Ratio (WHtR) values than women aged < 40 years [14]. In Korean studies, 28.6% of women in their 50s were found to have metabolic syndrome [15], high blood pressure, high fasting blood glucose, hyperlipidemia, low HDL cholesterol, and low exercise levels [16171819]. In a cohort study that identified factors influencing pre-diabetes, obesity, low HDL cholesterol levels, low physical activity, and hypertension were found to be major causes of prediabetes and were identified as modifiable risk factors [17]. Thus, screening tests for health education in high-risk middle-aged adults with obesity and insufficient physical activity are urgently needed [1].
In most previous studies, which included adults of all ages [10111617], pre-diabetes was associated with physiological changes such as hormonal changes in women after middle age and a further increase in obesity and reduction in physical activity. In addition, the results of previous studies showed that predictors of pre-diabetes are modifiable factors. Therefore, this study aimed to determine whether these factors affected classification as prediabetic by analyzing national representative data. The results of this study will identify pre-diabetic risk factors for middle-aged women, contribute to reducing the prevalence of diabetes, and serve as the basis for a nursing intervention planning strategy to control risk factors.
METHODS
1. Research Design and Procedure
This study was a secondary analysis using data from the 6th National Health and Nutrition Examination Survey (KNHANES). The investigation was a descriptive correlation study comparing a normal group with a pre-diabetes risk group to identify risk factors for pre-diabetes in middle-aged women. The survey sampling design adopted was a complex, stratified, multi-stage, probability-clustered survey of a representative sample of the community-dwelling civilian population.
According to the 2014 KNHANES Report [18] by the Korea Centers for Disease Control and Prevention, the prevalence of chronic diseases such as obesity, hypertension, and diabetes from 2005 to 2014 markedly increased in 2014. Therefore, the analysis was conducted to identify pre-diabetic risk groups for middle-aged women in 2014.
2. Setting and Sample
This study was based on raw data extracted for the year 2014, the second year of the 6th National Health and Nutrition Examination Survey (2013~2015). The data extracted covered 7,550 respondents from infants to the elderly in a composite sample design, with 3,840 household residents of 129 survey sites nationwide, and was stratified based on the intrinsic layers [gender, age, residential area, household, education]. Among these subjects, 2,650 middle-aged people aged 40 to 64 were extracted. Next, from this group we extracted 1,275 middle-aged women who were not diagnosed or treated for diabetes, thereby excluding 846 men and 108 women with missing data.
3. Measurements
1) Socio-demographic and clinical characteristics
The individual components of the health interview questionnaire included information on cigarette smoking, alcohol use, activity limitation, physical activity, and perceived health status, all of which were collected via questionnaires. Disease-related characteristics including smoking, height, weight, and BMI were also collected.
Risk factors for pre-diabetes based on the American Diabetes Association guidelines of 2018 were used as the criteria for screening for diabetes [12]. With regard to the presence of diabetes mellitus, presence or absence of CVD, and physiological parameters, the hematological test items of the screening test included fasting blood glucose, HbA1c, total cholesterol, fat, HDL, low-density cholesterol (LDL), and blood pressure measured by a nurse.
2) Central obesity
WHtR is used as a parameter for measurement of central obesity [20]. To determine if the use of WHtR in addition to BMI or Waist Circumference (WC) could help identify those at an increased cardiometabolic risk, participants were categorized according to BMI (overweight or nonoverweight) and WC (with or without central obesity), and each of the BMI and WC groups was further stratified by WHtR (WHtR < 0.53 vs. WHtR ≥0.53) [21].
3) Physical activity
The levels of physical activity were scored using the International Physical Activity Questionnaire (IPAQ)[22]. Physical activity included activities such as vigorous-intensity physical activity during the last 7 days (running, climbing, biking, swimming, soccer, jumping rope, sports activities such as singles tennis, physical activity, and carrying heavy items), moderate physical activity except walking (including slow swimming, doubles tennis, volleyball, badminton, ping-pong, general physical activity, and light-weight cargo handling activities), and walking activities (including walking for commuting, moving, and exercising).
The results of the IPAQ were converted into minutes of exercise, and the amount of exercise was calculated as the Metabolic Equivalent of Task (MET-min/week, MET). The total physical activity score was calculated by adding walking MET (3.3 × min × day), moderate-intensive physical activity MET (4.0 × min × day), and vigorous-intensity physical activity MET (8.0 × min × day). According to the MET results, physical activity levels were classified as low, moderate, and high. Low-physical activity was classified as less than 500 MET, moderate-physical activity as 501 to 999 MET, and high-physical activity as more than 1000 MET [23].
4. Data Collection
Survey data for the second year of the 6th KNHANES (2013~2015) used in this investigation were collected from 129 sites from January to December 2014, after which a screening and health questionnaire was administered. Health questionnaires were administered by a professional survey team consisting of nurses, dietitians, and health professionals. The KNHANES collects data for several variables regarding participants' demographic, social, health, and nutritional status from three component surveys: the health interview, health examination, and nutrition survey.
5. Ethical Considerations
The original data describing the national health and nutrition utilized in this study were in compliance with the personal information protection law and the statistical law, for which only data were provided that cannot be estimated from survey data collected with the approval of the research ethics review committee of the disease management headquarters (2013-12EXP-03-5C). A separate ethics review of the present study was not needed because publicly available data were used. The researcher conducted the study in consideration of the advice provided on the homepage of the National Health and Nutrition Survey (https://knhanes.cdc.go.kr/) and the rules for disclosure and use of raw materials.
6. Statistical Analysis
The SPSS/WIN 23.0 program (IBM SPSS Statistics, Chicago, IL, USA) was used for the statistical data analysis. We added sample weights and adjusted the analyses for a complex sample design in order to represent the entire Korean population. To use a method of analysis allowing complex sample design elements, clusters (primary extraction units) are plots and stratified variables are variance estimates. To assign the appropriate weight to each variable of the analysis, the weights were calculated by applying the health questionnaire and the examination weight. In the χ2 test, missing values via mean imputation, which fills in missing values with the mean value for the variable, were used to prevent the exaggeration of the significance of the results.
The multivariate logistic model was applied to identify the risk factors for pre-diabetes using a backward variable selection method that puts significant variables in the univariate analysis and applies pre-diabetes risk factors to the parent group, leaving only the significant variables. In the multivariate logistic analysis, 173 (13.6%) of the 1,275 subjects were missing data. In the logistic regression analysis, missing values were treated with pairwise deletion, which removes only missing values of variables for individuals, to minimize information loss resulting from missing data, and uses the remaining variables to calculate confidence intervals and regression coefficients. A two-tailed p-value less than .005 was considered statistically significant.
RESULTS
1. Participants' General Characteristics
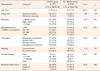
We analyzed data collected from women aged 40 to 65 after dividing them into two groups: 618 participants in the pre-diabetes group and 657 in the normal group. The results showed that age, education, monthly household income, and occupation were significantly different between two groups (p<.001). Alcohol consumption was higher in the pre-diabetes group, with significant differences between the two groups (t=10.23, p=.037). When asked about their health status, 21.2% of the pre-diabetic group gave a response of “good,” as did 30.6% of the normal group, which was a significant difference (t=10.33, p=.016). However, there was no difference between two groups as to whether they were living together or smoking (Table 1).
2. Risk Factors for Pre-Diabetes
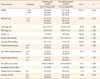
Overall, 19.7% of the individuals in the normal group and 33.2% in the pre-diabetic group had a WHtR of over 0.53 (t=287.11, p<.001), and 19.8% of individuals in the normal group and 34.8% in the pre-diabetic group had a BMI of over 25 kg/m2 (t=255.02, p<.001). Additionally, a significant difference was found between the pre-diabetic group and the normal group in participants who had hypercholesterolemia (total cholesterol > 240 mg/dL or taking cholesterol lowering medication) (t=31.33, p<.001), low levels of HDL cholesterol (HDL < 40 mg/dL) (t=12.76, p<.001), and hypertriglyceridemia (triglyceride > 200 mg/dL) (t=11.61, p<.001).
The amount of physical activity measured with IPAQ showed the physical activity of the subjects for the last 7 days, which was converted into MET (minute/week). There was a significant difference between the two groups: 820.6 MET for the normal group and 703.9 MET for the pre-diabetic group (t=25.15, p<.001). There were also differences in sedentary time, with 3.7 hours for those in the normal group and 6.5 hours in the pre-diabetic group (t=58.28, p<.001). The history of CVD was 26.4% in the pre-diabetic group and 13.2% in the normal group (t=6.01, p<.001) (Table 2).
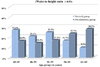
In the age-specific classifications of WHtR over 0.53, we found that the percentage of middle-aged women with WHtR above 0.53 in the pre-diabetes group increased as the age increased to 50 years or older (Figure 2).
3. Factors Influencing Pre-Diabetes
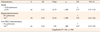
Table 3 shows the factors associated with pre-diabetes in middle-aged women based on multivariate logistic regression. First, in the analytical procedure, parental groups such as middle-aged women and the undiagnosed diabetic group were designated and their significant variables in Table 1 entered in the analytical program, followed by WHtR, BMI, hypertriglyceridemia, physical activity, sedentary time, and CVD history. Finally, age and monthly income, which are continuous covariates, were used as adjust variables.
Significant factors associated with the pre-diabetes were WHtR values, hypercholesterolemia, and low cholesterolemia. Middle-aged women with WHtR values over 0.53 were 1.7 times more likely (Odds Ratio [OR]=1.71, 95% Confidence Interval [CI]=1.27~2.29, p<.001) to develop pre-diabetes than those with WHtR values less than 0.53. Women with hypercholesterolemia were more likely to develop pre-diabetes (OR=2.02, 95% CI=1.42~2.86, p<.001). In addition, the likelihood of developing pre-diabetes was significantly higher in women with low HDL cholesterolemia than those without low HDL cholesterolemia (OR=1.89, 95% CI=1.18~3.02, p=.008).
DISCUSSION
This study was conducted to compare a pre-diabetes group and a normal group classified according to ADA criteria in order to identify the predictive factors for prediabetes in Korean middle-aged women.
The results showed that middle-aged women who had a WHtR of more than 0.53, a key predictor of metabolic syndrome [21], were 33.2% in the pre-diabetic group and 19.7% in the normal group. In addition, 34.8% of women in the pre-diabetes group had a BMI of more than 25 kg/m2, versus only 19.8% of women in the normal group. Additionally, the prevalence of women with WHtR ≥0.53 in the pre-diabetic group tended to increase with age, while tending to decrease in the normal group. In this study, middle-aged women with WHtR values of ≥0.53 were more likely to develop pre-diabetes than those with WHtR values less than 0.53. This result was similar to the finding of an increase in WHtR, a significant determinant of prediabetes, in 1,148 patients in a cohort study in Netherlands (NLCS) [24]. The finding is also consistent with that of a cohort study of 1,184 adults in Spain, which showed a strong relationship between abdominal obesity and prediabetes in both males and females [17]. Moreover, a survey to estimate the prevalence of pre-diabetes and diabetes with 1,915 subjects among adults 18 years or older in Palau found significant associations with pre-diabetes [11], and a cohort study of 816 pre-diabetic Korean adults over the age of 40 showed that increases in metabolic-syndrome-related factors and WHtR were predictive of pre-diabetes [21]. These results suggest that middle-aged women with pre-diabetes need to change their lifestyles to reduce abdominal obesity [1].
In order to reduce WHtR levels, regular physical activity along with lifestyle changes is important, as is reducing sedentary time [111724]. A review of the epidemiological evidence showed that women who had a moderate physical activity of about 30 minutes a day saw a lowered initiation and progression of the risk of CVD through beneficial effects, not only on adiposity but also on insulin sensitivity, glycemic control, type 2 diabetes, blood pressure, lipid, endothelial function, and inflammation defenses [14]. Despite these benefits, the measured amounts of physical activity using IPAQ in this study were 703.9 MET in the pre-diabetes group and 820.6 MET in the normal group, showing that both groups experienced more than the 600 MET of physical exercise recommended by the ADA [25]. However, the physical activity of the pre-diabetes group was lower than that of the normal group. This result is consistent with and supports the outcome of National Health and Nutrition Examination Survey (NHANES) in the United States of America, which showed that among 7,501 adults between the ages of 20 and 65, the physical activity of the 433 individuals in the pre-diabetes group was less than that of the 884 individuals in the normal group [26]. Moreover, this study showed sedentary time was 6.5 hours in the pre-diabetic group and 3.7 hours in the normal group-that is, the former spent 2.8 hours more than the latter in a sedentary state. The results of the current study also showed that the pre-diabetic group had fewer physical activities and longer sedentary time than the normal group, even though the former should act to promote their physical activities. These results supported the finding that the major causes of pre-diabetes in women were obesity, waist circumference, increase in sedentary lifestyle, and decrease of physical activities [11171927]. Middle-aged women known to have a high burden of Non-Communicable Diseases (NCD), including diabetes, who increased their physical activities have been shown to have decreased blood sugar, triglycerides, LDL levels, and central obesity, as well as increased HDL level [1123]. The American Diabetes Association (ADA) states that among asymptomatic pre-diabetic patients, those over 45 years of age with a BMI over 25 kg/m2 are likely to develop diabetes mellitus if they do not modify their lifestyle [121]. In addition, adults who are recognized earlier in the pre-diabetes stage are more likely to undertake physical activities and weight management, which may play a role in reducing the future morbidity rate of diabetes mellitus [1927]. Furthermore, the results of a study of 2,300 adults in Europe and globally are corroborated by the results of this study that increased physical activity and lower sedentary time were more closely connected with CVD, and physical activity was positively associated with improved waist circumference, blood pressure, mean arterial pressure, fasting insulin, 2 hr-glucose, Homeostasis Model Assessment of Insulin Resistance (HOMA-IR), triglycerides, C-Reactive Protein (CRP), and HDL levels [19]. Therefore, it is suggested that in order to reduce or prevent the prevalence of diabetes in the future, it is important to engage in physical activities, and proactive interventional strategies are required to promote such physical activities.
Evaluation of cholesterol in the pre-diabetes group revealed that 23.4% of participants had been diagnosed with hypercholesterolemia or were receiving treatment, 11.1% had HDL cholesterol levels < 40 mg/dL, and 14.1% had triglyceride levels >240 mg/dL, whereas only 11.2%, 5.5%, and 7.5% of participants in the normal group, respectively, were found to have these characteristics. This study also showed that lower HDL cholesterol or diagnosis of hypercholesterolemia was associated with a higher probability of being diagnosed with pre-diabetes.
Menopause-associated estrogen depression in middle-aged females is known to reduce the function of vascular endothelial, vascular reserve, and blood lipids [28], which causes a significant increase in BMI, fasting blood glucose, and blood pressure, accelerating the incidence of CVD, including the occurrence of dyslipidemia [29]. In addition, an investigation of 25,925 middle-aged women over 45 years of age without diabetes mellitus, adjusting for BMI, blood pressure, and lifestyle factors, showed that a higher lipoprotein insulin resistance score was associated with an increased likelihood of being diagnosed with diabetes [29], which supports the results of another study showing that lipoprotein insulin resistance is affected by dyslipoproteinemia [3031]. This insulin resistance is also related to obesity, and in cases where HDL is low and triglycerides are increasing, it influences pre-diabetes, suggesting that management and treatment of cholesterol and lifestyle modification are very important for middle-aged women [32]. In addition, high total cholesterol causes atherosclerosis and CVD [33]. In this study, univariate analysis revealed that significantly more individuals in the pre-diabetes group had prevalence of the CVD than in the normal group. The findings are supported by the Korean National Health Insurance Service-National Sample Cohort study, which revealed that the pre-diabetic group had a 1.3 times higher risk of cardiovascular morbidity in the 44.1% of patients with blood glucose levels of 100~125 mg/dL in a group of 13,829 adults observed for an average of 6.5 years [34].
This finding implies that an interventional strategy is needed to prevent middle-aged women with cardiovascular risk factors from progressing to pre-diabetes and highlights the need for improvement in lifestyle as well as proactive treatment to manage cholesterol in pre-diabetic women.
Our study has some limitations. One limitation is that the cross-sectional study design could not infer the causal relationship. Thus, in future studies a longitudinal design is required regarding the incidence of diabetes to infer causality. Another limitation is that although menopause is a time of important hormonal changes in middle-aged women, this study did not confirm the risk of prediabetes in women of menopausal and pre- and post-menopausal ages. Therefore, we suggest that future research address this point. Another limitation is that some of the sociodemographic characteristics were measured based on responses to a self-report questionnaire, so care must be taken when interpreting it. Despite these limitations, this study is meaningful in that it analyzes relatively large samples of the Korean population with a stratified multi-stage probability cluster questionnaire to identify the predictors of pre-diabetic morbidity in Korean middle-aged women. Previous studies conducted gender comparisons without limiting the age of onset of diabetes and pre-diabetes. However, very few studies have analyzed middle-aged women who have an increased prevalence of pre-diabetes and diabetes due to hormonal changes.
This study found that low HDL, high cholesterol levels, and a WHtR of more than 0.53 increased pre-diabetes incidence. Therefore, the contribution of this study is that cholesterol management and abdominal obesity management in middle-aged women can be important in preventing pre-diabetes.
CONCLUSION
This study was conducted to identify factors influencing pre-diabetes with a focus on middle-aged women, who are vulnerable to hormonal changes and physical changes, in accordance with the standards of diabetes diagnosis based on the National Health and Nutrition Survey. Significant factors for pre-diabetes were WHtR, hypercholesterolemia, and low HDL cholesterol. Additionally, the management of central obesity and cholesterol was found to be essential for middle-aged women with pre-diabetes.
To manage central obesity and cholesterol effectively, middle-aged women should receive education to increase their awareness of non-communicable diseases, such as diabetes, as this could facilitate healthy middle-aged menopause. Accordingly, further investigation of specific factors and characteristics influencing diabetes mellitus in middle-aged women is warranted, as is the development of intervention programs and the investigation of their effectiveness.

 XML Download
XML Download