

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary hyperparathyroidism (PHPT) is an endocrine disease characterized by the oversecretion of parathyroid hormone (PTH), resulting in increased serum calcium levels (1). The prevalence of the disease in the United States ranges from 0.1% to 0.45% (2). In a Korean study, Kim et al. (3) demonstrated an annual incidence of 0.007%–0.0014%. Treatment is required for symptomatic PHPT patients, but a study has also demonstrated that one-third of asymptomatic patients experience disease progression (4). Recent guidelines recommend clinical intervention in patients with elevated serum calcium levels (>1.0 mg/dL above the upper limit of normal), creatinine clearance <60 mL/min, T-score <−2.5, a history of fracture fragility, or if the patient is <50 years of age (56). Despite recent advances in medical therapy, surgical resection remains the only curative therapy for patients with PHPT (7). In cases of inadequate initial parathyroidectomy, persistent hyperparathyroidism (HPT) is indicated by increased serum calcium levels within 6 months of the initial surgery (8). Because 85% of all cases of PHPT arise from a single parathyroid adenoma, preoperative localization is required and the importance of conventional bilateral neck exploration (BNE) has been questioned (9). Recently, there has been a paradigm shift in parathyroid surgery from bilateral or unilateral neck exploration (UNE) towards the use of minimally invasive parathyroidectomy (MIP) as a study has demonstrated the superiority of this approach (1011). For MIP, precise preoperative localization is extremely important to determine the site of incision (12). Imaging approaches for localization include cervical ultrasonography (US), 99mTc-sestamibi SPECT/CT (SeS), 2- and 4-dimensional computed tomography (CT), US-guided biopsy and intraoperative US (13). The improvement in localizing imaging and the development of intraoperative PTH (IOPTH) measurement means that MIP has become a widely accepted approach (14).
Because of the rarity of the disease and recent rapid innovations in localization and surgical techniques, there were no standardized Korean guidelines for treating PHPT.
The aim of the current study was to evaluate changes over time in the use of preoperative localization and surgical techniques for the treatment of patients with PHPT in single tertiary center in Korea.
MATERIALS AND METHODS
1. Patients
Data from patients with parathyroid disease who had undergone parathyroidectomy between January 2000 and December 2016 were retrospectively reviewed. Patients were excluded if they had secondary or tertiary HPT, had undergone thyroidectomy due to a co-existing thyroid malignancy, or if their surgical records were unavailable. All the patients included were tested for US, sonographic marking, 99mTc sestamibi scan, CT, and IOPTH.
All demographics, biochemical values, preoperative imaging reports, surgical details, intraoperative findings and pathologic assessments were obtained in accordance with the requirements of the Institutional Review Board (No. 1909-044-1062) of Seoul National University Hospital (Seoul, Korea). Imaging data were reviewed independently by radiologists or nuclear medicine physicians.
2. US
US examinations were performed with a linear transducer at a frequency of 7.5–15 MHz. The device used were Accuvix XG, Medison, Seoul, Korea; or iU22, Philips Healthcare, Best, the Netherlands; or Aixplorer, SuperSonic Imagine, Aix-en-Provence, France. Longitudinal and transverse images were taken from the clavicles to the mandible in the neck extended position. Contrast enhancement was not performed. US was performed by multiple radiologists who specialize in endocrine/breast section. With guidance of US, some portion of patients received preoperative US marking above the suspected lesion with a marking pen was done and translucent film dressing was applied on it.
3. SeS
Device for scanning and SPECT/CT were Dong-A Pharmaceutical, Seoul, Korea; or Lantheus Medical Imaging, North Billerica, MA, USA. Dual phase acquisitions were obtained after 15 and 150 minutes of intravenous (IV) 99mTc-sestamibi (mean 740 MBq). Planar scans were obtained by a single detector with a low-energy, high-resolution parallel collimator. The SPECT/CT system, which was introduced in our center in 2011, generated 15 and 150 minutes planar scans and delayed SPECT/CT scans. The 99mTc window ranged from 133–147 keV. After SPECT scanning, CT acquisition was performed. After a scout scan (120 kVp, 30 mA, anterior view), an axial field of view was set from the neck to mid-chest. Helical CT scanning was performed in consecutive order (120 kVp, 80 mA; 3.75 mm slice thickness; 512×512 matrix).
4. CT
Before 4-dimensional CT was introduced at 2011, contrast-enhanced chest protocol or neck protocol or thyroid protocol CT was used. After 32-sliced or 64-sliced unenhanced image was taken, IV contrast was injected and image was retaken 60 seconds after IV injection. Parathyroid 4-dimensional CT was introduced at our center in 2011, and the device used was Brilliance 64, Philips Healthcare, Best, Netherlands. In parathyroid 4-dimensional CT, images were generated using a 64-slice multi-detector CT scanner. Craniocaudal coverage was from the superior (external auditory meatus) to inferior end (2 cm below the carina) with a 168×168 mm field of view. Image reconstruction was performed in 2 planes (axial and coronal) at 3 mm thickness and spacing. After the initial unenhanced scan had been obtained, 90 mL of IV contrast was injected. Parathyroid 4-dimensional CT involves repeated scanning at 30, 60, and 90 seconds after IV contrast administration. The mean CT dose index per imaging phase was 11.4 mGy.
5. Intraoperative PTH
IOPTH assay was routinely performed after 2011 in our center. Pre-incision, pre-excision, and post-excision at 5 minutes and 10 minutes PTH values were tested. Applying Miami criteria, procedures could be terminated when PTH level declines over 50% (15).
6. Surgery
All patients underwent planned bilateral or UNE MIP via an on the top incision or bilateral axillo-breast approach (BABA) incision. For patients who underwent BNE or UNE, a 6 cm-length low collar incision was made 2 finger-breadths above the sternal notch (16). For patients who underwent focused parathyroidectomy, 2–2.5 cm on the top incision was made above marked parathyroid lesion. BABA or posterior auricular approach was made for robot parathyroidectomy or endoscopic parathyroidectomy. Once surgery had been completed, pathologic review of the resected specimens was performed.
7. Statistical analysis
SPSS 22 (IBM SPSS statistics, Armonk, NY, USA) was used for statistical analysis. Student's t-test was used to compare the difference of operation time between the group of patients who underwent specific preoperative localization method and group of patients who did not. One-way analysis of variance was used to compare the operation time between each surgical methods. P value <0.05 was considered to be statistically significant.
RESULTS
1. Patients
A total of 246 patients were treated during the study period; following exclusion of subjects who did not meet the study criteria (Fig. 1), 157 patients (50 male, 107 female with a mean age of 54.1±13.0 years) were included in the analysis. The characteristics of these patients are shown in Table 1. Among the study group, 157 patients had biopsy-confirmed parathyroid adenoma (single n=156 [99.4%], double n=1 [0.64%]).

Table 1
Patient characteristics and preoperative localization

Tumors were located in the right superior parathyroid (n=11, 7.01%), right inferior parathyroid (n=61, 38.9%), left superior parathyroid (n=34, 21.7%), left inferior parathyroid (n=51, 32.5%), and ectopic (peri-SVC) parathyroid (n=1, 0.64%).
2. Preoperative localization
Of the enrolled patients, 134 underwent US for preoperative localization (85.4%), 110 with preoperative sonographic marking (70.1%). A total of 150 patients underwent 99mTc-sestamibi scan (95.5%), with 83 scan-only patients (52.9%) and 67 with SeS (42.7%); 148 patients underwent CT scan preoperatively (94.3%), 84 patients with 2-dimensional (53.5%), and 64 patients with 4-dimensional CT, including parathyroid 4-dimensional CT (40.8%).
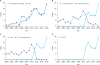
Fig. 2 shows the number of perioperative localizations performed per year from 2000 to 2016. The use of US increased over time, as did the use of sonographic marking, which was introduced in 2006. The 4-phase CT and SeS techniques were introduced in our center in 2011 and showed an increase in usage, replacing the use of 2-dimensional CT and 99mTc-sestamibi scan. IOPTH was also introduced in 2011 and was associated with increased use over time.
Fig. 2
Number of each perioperative localization method over time. (A) US and sonographic marking (B) 2-dimensional CT and 4-dimensional CT (C) 99mTc-sestamibi scan and SeS (D) IOPTH.
US = ultrasonography; CT = computed tomography; SeS = 99mTc-sestamibi SPECT/CT; IOPTH = intraoperative parathyroid hormone.
3. Surgery
Evaluated by Fisher's exact test, there were significant preferences in surgical technique among 4 different operators (P<0.001). One operator preferred UNE (93.8%), while other operator preferred focused parathyroidectomy (85.9%). Other 2 operators had similar rates of UNE and focused parathyroidectomy.
Surgical records showed that 65 patients (41.4%) underwent low collar incision; eleven patients (7.01%) underwent BNE, 54 (34.4%) underwent UNE. A total of 84 patients (53.5%) underwent on the top incision for focused parathyroidectomy 4 patients (2.55%) underwent BABA incision; 3 (1.91%) robot BABA parathyroidectomy and one (0.64%) endoscopic parathyroidectomy. Four patients (2.55%) underwent posterior auricular incision for endoscopic parathyroidectomy (Table 2).
Table 2
Surgical results in patients with parathyroid adenoma

Since its introduction in 2011, IOPTH had been performed in 80 patients (51.0%), all of which met the Miami criteria during surgery.
The surgical trends are shown in Fig. 3. The number of UNEs performed reduced over time; in contrast, the use of focused parathyroidectomy increased.
Fig. 3
Changing trend in operational methods in patients with parathyroid adenoma.
UNE = unilateral neck exploration; BNE = bilateral neck exploration; FP = focused parathyroidectomy.

Sonographic marking (P=0.018), SeS (P<0.001), 2-dimensional CT (P=0.018), 4-dimensional CT (P<0.001), IOPTH (P<0.001) significantly reduce operation time (Table 3).
Table 3
Operation time difference of each preoperative localization
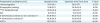
Comparison between operation time according to preoperative localization by t-test. Among preoperative localizations, sonographic marking, SeS, 2-dimensional CT, 4-dimensional CT, IOPTH significantly reduce operation time. Values are presented as mean±standard deviation.
SeS = 99mTc-sestamibi SPECT/CT; CT = computed tomography; IOPTH = intraoperative parathyroid hormone.
Operation time was significantly different among surgical methods (P<0.001). Mean operation time of focused parathyroidectomy was the lowest (71.1±35.0 minutes) followed by UNE (98.7±43.8 minutes), robotic parathyroidectomy (118.3±36.9 minutes), endoscopic parathyroidectomy (119±49.8 minutes), and BNE (128.7±55.9 minutes) (Table 4).
Table 4
Operation time of each surgical methods

| Surgical methods (min) | Operation time | P value |
|---|---|---|
| BNE | 128.7±55.9 | <0.001 |
| UNE | 98.7±43.8 | |
| Focused parathyroidectomy | 71.1±35.0 | |
| Endoscopic parathyroidectomy | 119.0±49.8 | |
| Robotic parathyroidectomy | 118.3±36.9 |
Comparison of operation time according to each surgical techniques by 1-way analysis of variance. Focused parathyroidectomy consumes less operation time than other surgical methods, followed by UNE, robotic parathyroidectomy, endoscopic parathyroidectomy, and BNE. Values are presented as mean±standard deviation.
BNE = bilateral neck exploration; UNE = unilateral neck exploration.
DISCUSSION
In this study, we can identify the usage of preoperative localization method US, sonographic marking, IOPTH assay increased, 4-dimensional CT and SeS replacing the use of 2-dimensional CT and 99mTc-sestamibi scan. In the surgical section, cases of UNE are replaced by focused parathyroidectomy. The ultrasonographic marking, SeS, 2-dimensional CT, 4-dimensional CT, IOPTH significantly reduce operation time. In this study. majority of patients underwent US (85.4%) and 99mTc-sestamibi scan (95.5%) since 2000, so the number of patients who did not underwent US and 99mTc-sestamibi scan were relatively too small for adequate statistical comparison. Nonetheless, all of the other perioperative localization had proven to reduce operation time. In conclusion, in order to reduce operation time, it may be essential to perform all of the perioperative localization done in our study.
Among all the other surgical methods done in this study, focused parathyroidectomy was proven to consume lower operation time than any other methods. Unless otherwise indicated, focused parathyroidectomy may be advised for the first choice of surgical method. Only 8 of 157 patients enrolled in this study who underwent endoscopic or robotic parathyroidectomy. So for adequate comparison of operation time, further study should retain more of endoscopic or robotic parathyroidectomy cases.
In a previous study, Slepavicius et al. (17) showed that when compared with conventional BNE, MIP was associated with significantly lower postoperative pain intensity at 4, 8, 16, 24, 36, and 48 hours, lower analgesic consumption, lower analgesia request rate, shorter length of scar and a higher postoperative cosmetic satisfaction rate at 2 days, 1 month and 6 months. Other studies show that MIP is associated with a reduced length of hospital stay, limited cervical dissection, and decreased cost (1819). MIP as a surgical intervention for the treatment of PHPT is an inevitable global trend, and accurate perioperative localization of parathyroid adenomas is of critical importance in surgical planning for MIP (20). Traditional preoperative localization includes US, preoperative sonographic marking, 2-phase CT, 99mTc-sestamibi scan, and more recently, SeS, and 4-dimensional CT (212223).
A meta-analysis of 43 studies performed by Cheung et al. (24) reported that the positive predictive value of US is comparable to both SeS (90.7%) and 4-dimensional CT (93.5%). Some studies show that US alone can reliably locate parathyroid tumors and facilitate MIP (25). In our study, US is proven to be an efficient preoperative localization method, and with US guidance, preoperative marking made it possible to perform on the top incision for focused parathyroidectomy.
In the current study, 99mTc-sestamibi scan was the most common method of preoperative localization, including SeS, which was introduced in 2011. In a 2005 meta-analysis of patients with PHPT, 99mTc-sestamibi scan showed an overall sensitivity of 88% for the detection of single adenomas, 45% for multigland hyperplasia and 30% for multiple adenomas (26). The current study enrolled only one patient with multiple adenoma and 7 with multigland hyperplasia, including 6 multiple endocrine neoplasia type 1 patients, and SeS resulted detecting multiple adenoma patients and 2 multigland hyperplasia patients, but 5 multigland hyperplasia patient resulted in detecting one or no abnormalities in 99mTc-sestamibi scan.
In 2011, 4-phase CT emerged as an alternative to CT and 4-dimensional CT provides rapid anatomic and functional information, even detecting some supernumerary (5%–13%) and ectopic parathyroid glands (4%–16%) (2728). In the current study, 4-phase CT was seen to gradually replace conventional CT over time. By observing the changing trends in diagnosing, localizing and the excising tumors, we believe that it will facilitate the development of Korean guidelines in the near future.
There are several limitations to our study. First, because of the retrospective study design, variables such as difference between each surgeon's preference and procedures were not controlled. Secondly, because of the limitations of diagnostic tools for PHPT, the number of patients in the early years is relatively small compared with more recent years, which may introduce bias. Thirdly, as there were no cases of recurrence or reoperation except cases who developed secondary or tertiary HPT after initial surgery, the analysis of surgical outcomes, particularly the recurrence and repeat surgery rate, was not possible.
CONCLUSION
Over a 16-year period, this study highlights changes in the use of preoperative localization and surgical techniques in a single tertiary center. In order to reduce operation time, sonographic marking, 99mTc-sestamibi scan, SeS, CT, IOPTH should be performed perioperatively, and focused parathyroidectomy could be the first choice of surgical methods.
 XML Download
XML Download