

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The surgical treatment of breast cancer has undergone a paradigm shift from lifesaving surgery to balancing the consideration of aesthetics and oncologic outcomes [12]. Skin-sparing mastectomy (SSM) has become popular for the treatment of oncologic breast surgery, since it ensures better patient satisfaction and quality of life and exhibits similar oncologic outcomes to conventional mastectomy [34].
Owing to the nipple's aesthetic value and restoration difficulty, nipple-sparing mastectomy (NSM) has gained popularity in the last decade, with better aesthetic and psychological outcomes [5]. Consequently, the eligibility of patients for NSM has been an important question. However, there exist no clear criteria for optimal patient selection for NSM. Factors such as tumor size (greater than 3.0 cm), histopathologic type, inflammatory breast cancer, direct skin or nipple involvement, tumor–nipple distance (TND; less than 2.0 cm), and clinically positive axillary lymph nodes have been suggested to reduce the oncologic safety of the procedure [678].
Although the indications for NSM are expanding, there remains a debate regarding TND. In a previous study with a 25.6-month follow-up period [9], the oncologic outcomes of NSM followed by immediate breast reconstruction (IBR) did not significantly differ according to TND. Here, we conducted a retrospective observational study using the same cohort to investigate the long-term outcomes of NSM with IBR according to TND.
Methods
Study design
In total, 266 patients who underwent NSM with IBR between January 2008 and December 2014 at Samsung Medical Center, Seoul, Korea were enrolled in this retrospective study. Of these patients, 21 were excluded because of a loss to follow-up, so 245 patients were ultimately included in this study. The “short TND (STND) group” comprised patients with a TND < 2.0 cm, and the “long TND (LTND) group” comprised patients with a TND ≥ 2.0 cm. The primary endpoint was local recurrence-free survival (LRFS), and the secondary endpoint was disease-free survival (DFS), which included locoregional recurrence (LRR), distant metastasis (DM), and contralateral recurrence. Detailed information on patient enrollment can be found in a previous report [9]. The need for informed consent was waived because of the low risk posed by this investigation. This study adhered to the ethical tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Samsung Medical Center in Seoul, Korea (IRB No. 2018-07-102).
Preoperative evaluation
Patients were evaluated clinically to detect any signs of skin, nipple-areola complex (NAC), or nipple involvement that was clinically obvious by the presentation of a retracted nipple. Preoperative breast magnetic resonance imaging (MRI) was used to measure the TND of all eligible patients. Here, TND was measured as the shortest distance between the tumor and the base of the nipple in centimeters. The scans of the patients were reviewed by an expert and dedicated breast radiologist. The measurement of TND by preoperative MRI in patients who had undergone neoadjuvant chemotherapy (CTx) was conducted after completion of CTx. Patients with evidence of pathological complete response after neoadjuvant CTx were ultimately excluded from the study.
Intraoperative pathologic diagnosis
Intraoperative frozen biopsy was performed to confirm that the margin of resection at the nipple base was negative for tumor cells. The same frozen biopsy sections were sectioned perpendicularly for permanent biopsy. Intraoperative frozen sections were reviewed by dedicated breast pathologists. Patients whose intraoperative frozen sections were positive for invasive ductal or lobular carcinoma, ductal carcinoma in situ (DCIS), atypical ductal hyperplasia with necrosis, or lobular neoplasia underwent NAC removal and were excluded from this study.
Perioperative protocol
All patients underwent IBR following tumor removal. However, the choice of reconstructive option depended on the breast characteristics and desires of the patient, which were determined during preoperative consultations with the plastic surgeons. Neoadjuvant and adjuvant CTx, radiotherapy (RTx), and hormonal treatment (HTx) were decided by a multidisciplinary team including an expert breast medical oncologist. All specimens that underwent pathological examination were evaluated for tumor size, histopathology, nuclear grade (NG), lymphovascular invasion (LVI), hormone receptor (HR) status, and human epidermal growth factor receptor-2 (HER-2) expression.
Surgical technique
A 7.0 cm long radial incision was performed, which had the advantages of good exposure and bleeding control. The upper and lower flaps were raised and reached medially around the NAC. Retractors were applied superior and inferior to the NAC, and the nipple tissue was left hanging from the skin of the NAC. Using the blade, the nipple tissue just behind the dermis was sharply dissected at the nipple–dermal junction. The nipple tissue attached to the remaining glandular tissue was marked with ink and dissected for frozen nipple margin analysis. Using electrocautery, the glandular tissue was removed by subcutaneous dissection.
Follow-up
Postoperative follow-up visits typically occurred every 6 months (2 times per year) for a total of 5 years and then annually thereafter. During each visit, patients were examined clinically for evidence of LRR or DM and underwent both radiological and laboratory investigations. Radiological surveillance for LRR was conducted every 6 months by breast sonography and/or mammogram. Surveillance for DM was conducted annually by computed tomography of the chest and abdomen, and/or a bone scan. After 5 years of follow-up, patients were followed annually with breast sonography and/or mammogram.
Data collection
The demographic data and clinicopathological characteristics of the patients were collected from electronic medical records and comprised patient age, family history of breast cancer, genetic risk, body mass index (BMI), types of IBR and axillary surgery, neoadjuvant CTx, adjuvant CTx/radiation therapy, LRR, DM, and death. For patients with bilateral breast cancer, each breast was considered separately.
Statistical analysis
Patient characteristics were compared using independent t-tests for continuous variables and the χ2 or Fisher's exact test for categorical variables. Values are reported as mean ± standard deviation. Kaplan-Meier curves, with the corresponding results of log-rank tests, were constructed for DFS and LRFS. For all analyses, a p-value < 0.05 was considered statistically significant. All statistical analyses were executed using SAS version 9 (SAS Institute, Cary, USA) and R3.0.3 (http://www.R-project.org; R Foundation for Statistical Computing, Vienna, Austria).
Results
Overall, 245 patients who underwent NSM were included in this study. Of those, the LTND group comprised 117 patients, and the STND group comprised 128 patients. The proportion of the groups varied by year, as shown in Figure 1. The overall follow-up period ranged from 15 to 109 months, with a mean of 60.5 (± 19.9) months. The mean follow-up period in the LTND and STND groups was 63.9 (± 20.1) months and 56.9 (± 19.2) months, respectively.
Figure 1
The annual proportions of patients in the LTND and STND groups.
LTND = long tumor–nipple distance; STND = short tumor–nipple distance.

Patient characteristics
The clinicopathological features of both groups are shown in Table 1. The mean age of the STND and LTND groups was 41.7 (± 8.0) years and 43.1 (± 7.2) years, respectively. Additionally, the mean BMI of the STND and LTND groups was 21.9 (16.9–29.6) kg/m2 and 21.6 (16.6–31.3) kg/m2, respectively. A positive family history of breast cancer was noted in 16 patients (12.5%) in the STND group, and 13 patients (11.1%) in the LTND group. There were no significant differences between the 2 groups with respect to LVI, NG, multiplicity, nodal status, HR status, or HER-2 status. The median TND of all patients, the STND group, and the LTND group was 1.7 cm (range: 0.0–7.0 cm), 0.7 cm, and 3.0 cm, respectively. The STND group had significantly smaller tumors than the LTND group (p = 0.005). However, there was no significant difference in lymph node involvement between the 2 groups (p = 0.950). No lymph node involvement was found in 97 patients (75.8%) in the STND group and 87 patients (74.4%) in the LTND group.
Table 1
Clinicopathological characteristics of the STND and LTND groups

Values are presented as number (%), mean ± standard deviation or number (range).
STND = short tumor–nipple distance; LTND = long tumor–nipple distance; BMI = body mass index; LVI = lymphovascular invasion; NG = nuclear grade; TND = tumor–nipple distance; IDC = invasive ductal carcinoma; ILC = invasive lobular carcinoma; DCIS = ductal carcinoma in situ; ER = estrogen receptor; PR = progesterone receptor; HER-2 = human epidermal growth factor receptor-2; TNBC = triple negative breast cancer.
Medical treatment
The medical treatments administered to the patients are shown in Table 1. The administration of neoadjuvant CTx, adjuvant RTx, and adjuvant HTx was not clinically different between the 2 groups. A significantly smaller percentage of patients underwent adjuvant CTx in the STND group (39 patients; 30.5%) compared to the LTND group (62 patients; 53.0%) (p < 0.005).
Surgical characteristics
The types of axillary surgeries and IBR performed are shown in Table 2. In total, 194 patients (79.2%) underwent sentinel lymph node biopsy—103 patients (80.5%) and 91 patients (77.8%) in the STND and LTND groups, respectively. Furthermore, permanent implant following tissue expander insertion was the most used reconstructive option in both the STND and LTND groups, with 83 patients (64.8%) and 86 patients (73.5%), respectively, choosing this procedure.
Table 2
Surgical treatment characteristics of the STND and LTND groups

Values are presented as number (%).
STND = short tumor–nipple distance; LTND = long tumor–nipple distance; SLNB = sentinel lymph node biopsy; ALND = axillary lymph node dissection; IBR = immediate breast reconstruction; LD = latissimus dorsi; TRAM = transverse rectus abdominis myocutaneous; DEIP = deep inferior epigastric perforator artery.
Oncologic outcomes
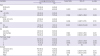
The description of events is shown in Table 3. There were 4 cases of LRR in the STND group—one case in the NAC and 3 cases in the skin and chest. In the LTND group, there were 6 cases of LRR—3 involving the NAC, 2 in the skin and chest wall, and one case of regional recurrence. Among these 10 patients with LRR, no patient exhibited DM and death with respect to recurrence in the contralateral breast, 2 cases were recorded in the STND group and one case was noted in the LTND group. Furthermore, DM was observed in 3 cases in the STND group (2 in the liver and one in the lymph nodes) and 6 cases in the LTND group (2 in the liver, one in the lung, one in the brain, and 2 in the lymph nodes). Mortality occurred in 3 cases in the study—2 STND group patients and one LTND group patient. Table 4 shows the LRR sites—4 patients experienced nipple recurrence, 5 patients experienced skin or chest wall recurrence, and only one patient showed regional recurrence. There were no significant differences between the 2 groups with respect to DFS or LRFS (log-rank test, p = 0.333 and p = 0.475, respectively) (Figure 2). There were also no significant differences with respect to DFS or LRFS stratified by DCIS and invasive cancer (log-rank test, p = 0.360 and 0.475 for DCIS and p = 0.374 and 0.420 for invasive cancer) (Figure 3). The univariate analysis for LRR did not exhibit a significant difference according to TND (p = 0.919, hazard ratio, 1.5420; 95% confidence interval, 0.4661–5.1009) (Table 5).
Table 3
Description of events
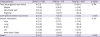
Table 4
Locoregional recurrence sites

| Characteristics | Frequency | Percent | Cumulative percent |
|---|---|---|---|
| Nipple | 4 | 1.6 | 1.6 |
| Skin or chest wall | 5 | 2.0 | 3.7 |
| Regional recurrence | 1 | 0.4 | 4.1 |
| No recurrence | 235 | 95.9 | 100.0 |
| Total | 245 | 100.0 |
Figure 2
Kaplan-Meier analysis of DFS and LRFS in the STND and LTND groups.
DFS = disease-free survival; LRFS = local recurrence-free survival; STND = short tumor–nipple distance; LTND = long tumor–nipple distance.

Figure 3
Kaplan-Meier analysis of DFS and LRFS in the STND and LTND stratified by ductal carcinoma in situ (A, B) and invasive cancer (C, D).
DFS = disease-free survival; LRFS = local recurrence-free survival; STND = short tumor–nipple distance; LTND = long tumor–nipple distance.
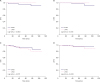
Table 5
Univariate analysis of locoregional recurrence
Discussion
In the related previous study, no significant differences in complications, DFS, or LRFS were noted between patients with a TND < 2.0 cm and those with a TND ≥ 2.0 cm. However, that study was limited by its short follow-up period [10]. In this study, which included the same cohort of 245 patients who underwent NSM, our aim was to investigate the differences in long-term outcomes between the STND group, comprising 52.2% of patients, and the LTND group, comprising the remaining 47.8% of patients. This study reported 3 cases of mortality, 9 cases of DM, and ten cases of LRR. The current study analyzed the long-term follow-up data of patients who underwent NSM. The incidence of LRR involving the nipple, skin, or chest wall was 4.1%, with nipple recurrence occurring in 1.6% of patients; there was no significant difference between the 2 groups. These results lie within the average rate of previous studies (0.0%–25.7%), including those that specified STND as an exclusionary factor [111121314].
The United States National Comprehensive Cancer Network 2018 guidelines support the use of NSM in patients with breast cancer provided that it is to treat early-stage, biologically favorable, invasive cancers, and/or DCIS > 2.0 cm from the nipple, without any evidence of nipple involvement such as Paget's disease or nipple discharge associated with malignancy and/or without evidence of malignant involvement of subareolar tissues on preoperative imaging [15]. However, our study suggests that NSM is oncologically safe even when a patient's TND is < 2.0 cm. With the increased rate of NSM use in breast cancer, several studies have compared the oncologic safety profile of this technique with that of others [1617]. Gerber et al. [1] reported no significant differences in complications between NSM, SSM, and modified radical mastectomy. Similarly, a 2011 meta-analysis by De La Cruz et al. [18] exhibited no differences among the aforementioned 3 techniques with regards to survival or local recurrence.
Regarding NSM eligibility, TND was initially considered to be a critical criterion for patient selection, with some studies correlating NAC involvement and tumor distance from the NAC. Subsequently, several studies into NSM excluded patients according to TND, many considering 2.0 cm as the safe cutoff point [19202122]. Conversely, other authors have considered expanding the inclusion criteria, though still imposing a minimum distance restriction. For instance, Jensen et al. [12], Sacchini et al. [23], and D'Alonzo et al. [24] suggested that a TND of 1 cm is an appropriate minimum distance for NSM. Separately, in a study of 112 patients, Ponzone et al. [25] suggested that a TND of 5 mm on MRI is sufficient for NSM eligibility. Other studies pointed out the sensitivity of MRI in detecting NAC involvement; Mariscotti et al. [26] conducted a study using MRI and suggested a TND cutoff value of 10 mm.
The risk of involvement of the NAC increases as TND decreases [252728]. The primary oncological concern of NSM is the risk of occult involvement of the NAC. However, Dent et al. [29] conducted a study of 195 patients who met the inclusion criteria for NSM. These patients were classified by NSM candidacy using a TND cutoff of 2.0 cm as seen in sonography and/or MRI, and were then reclassified using a TND cutoff of 1.0 cm. There was no significant difference in the rate of pathologically confirmed NAC involvement between candidates and non-candidates using a cutoff of either 2.0 cm or 1.0 cm, indicating that a TND of 1.0 cm should be safe for NSM.
Ultimately, a TND cutoff value of 2.0 cm is recommended for NSM, though this is less important than evidence of disease on the mandatory intraoperative nipple margin biopsy. In addition, the recurrence rates in the NAC after NSM are acceptably low (0.0%–3.7%), as reported by Galimberti et al. [30]. In our study, the NAC recurrence rate was 1.6%, affecting one case in the STND group and 3 cases in the LTND group, with no statistically significant difference noted between groups (log-rank test, p = 0.714).
There are a few limitations of the current study. The retrospective nature of this study may have given rise to selection bias. Furthermore, a greater number of patients in the STND and LTND groups had DCIS and underwent CTx, respectively, and these differences may have affected prognosis. However, the main strength of this investigation is that it is the first to compare long-term follow-up outcomes between STND and LTND patients who underwent NSM followed by IBR. Taken together, the long-term follow-up of patients treated with NSM revealed that oncological safety is not affected by TND. This suggests that patient eligibility for NSM for the treatment of breast cancer could be expanded to include more patients with tumors closely positioned to the nipple in preoperative MRI, if the intraoperative frozen biopsy of the nipple margin is free of tumor cells.
 XML Download
XML Download