

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Breast cancer is one of the most common cancers in women worldwide and its incidence has been increasing rapidly. Mucinous breast carcinoma (MBC) is a relatively rare type of tumor accounting for only 1%–6% of all breast cancers [123]. MBCs are associated with a good prognosis and have a better prognosis than that for invasive ductal carcinoma (IDC). They usually occur in women aged above 60 years and in postmenopausal women. MBCs consist of small clusters of tumor cells with large amounts of extracellular and extra-luminal mucus in direct contact with the stroma [345]. However, the presence of the mucinous carcinoma pattern in a breast mass is not a guarantee of good prognosis. Attentive gross examination and generous histologic sampling are necessary to ensure that the histologic pattern is pure and, thus, of prognostic significance [4]. MBCs are mostly positive for estrogen and/or progesterone receptors (ER/PR-positive) and negative for human epidermal growth factor receptor 2 (HER-2). Additionally, MBCs are less likely to involve the axillary lymph nodes (ALN) than other types of breast cancer. As such, although they are a form of invasive breast cancer, MBCs tend to be less aggressive and respond well to adjuvant treatment and ultimately have a good prognosis [678]. Different guidelines have been established for adjuvant systemic therapy of MBCs [49]. The National Comprehensive Cancer Network (NCCN) guideline recommends treatment according to the hormone receptor status; patients who are hormone receptor-negative are recommended the same treatment as in other breast cancers with poor prognosis, while those who are hormone receptor-positive are recommended to consider chemotherapy only if they have node positivity. Early-stage MBC patients, such as those with N0 or N1mi stage, should receive endocrine therapy, while patients with node positivity (one or more metastases > 2 mm) could be administered adjuvant chemotherapy [10]. However, most treatment guidelines for adjuvant chemotherapy of MBC were derived from IDC treatment experiences. MBC is a relatively rare type of breast cancer; thus, most MBC studies included few patients and limited follow-up periods. Therefore, the treatment guidelines for MBC have not been rigorously validated [11]. Previous studies have shown that many MBC patients receive adjuvant chemotherapy [61213]. However, adjuvant chemotherapy results in increased side effects, including toxicity, and whether adjuvant chemotherapy benefits survival from MBC remains unclear [14]. Therefore, given the good prognosis of MBC, adjuvant chemotherapy may be overtreatment. Using the Korean Breast Cancer Registry (KBCR), this study aimed to verify whether adjuvant chemotherapy has any clinical benefits in ER-positive MBC and whether adjuvant chemotherapy can be omitted in these patients.
Methods
Data source
The KBCR is a prospectively maintained, online-based database of the Korean Breast Cancer Society established in 1996 [15]. More than 100 hospitals throughout the Republic of Korea have voluntarily participated in this program. In 2013, the registry was estimated to include more than 65% of all newly diagnosed breast cancer patients in Korea [16]. Patient data on sex, age, tumor and nodal stage according to the American Joint Committee on Cancer classification, and surgical method are registered as essential data, while pathological findings, laboratory findings, treatment modality (endocrine therapy, radiotherapy, and chemotherapy) are optional data. Data on survival, including dates and causes of death, were obtained from the Korean Central Cancer Registry, Ministry of Health and Welfare, Korea updated on December 31, 2016. The KBCR database does not include the types and dates of tumor recurrence.
Participant selection
Of the 3,076 patients recorded in the KBCR with a pathological diagnosis of MBC between January 1990 and August 2016, we excluded those who had a previous history of breast cancer, had not been treated for breast cancer, or were treated with neoadjuvant and palliative chemotherapy. We collected data on age at diagnosis, method of surgery, pathologic stage, histologic grade, lymphovascular invasion (LVI), ER/PR/HER-2 status, p53, and type of adjuvant treatment. This study protocol was approved by the Institutional Review Board (IRB) of Seoul St. Mary's Hospital (IRB number: KC17RESI0649) and was conducted in accordance with the tenets of the Declaration of Helsinki. Informed consent from the patients was not required in this study.
Study variables
The primary variables analyzed were breast cancer-specific survival (BCSS) and overall survival (OS) for all MBC and ER-positive MBC patients. The secondary variable was the survival benefit of adjuvant chemotherapy to ER-positive MBC. The BCSS and OS for MBC were calculated using data from the KBCR database. BCSS and OS were defined as the time from the first diagnosis of breast cancer to death from breast cancer and any other causes, respectively. Data were censored on December 31, 2016.
Statistical analysis
Univariate and multivariate analyses for BCCS and OS were performed using a Cox proportional hazard ratio (HR) model to estimate adjusted HRs and 95% confidence intervals (CIs) to adjust for prognostic factors. Multivariate analysis was used to investigate variables that were significant in the univariate analysis. The survival analysis was performed using the Kaplan-Meier method and the chemotherapy and no chemotherapy groups were compared using the log-rank test to evaluate the survival difference. The p-values < 0.05 were considered statistically significant. All analyses were performed using the SAS 9.4 (SAS Institute Inc., Cary, USA) and IBM SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, USA).
Results
Patient characteristics
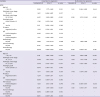
A total of 2,988 MBC patients with available medical records were enrolled in this study. The median follow-up time was 100 months (range, 2–324 months). The mean age of the patients was 49.6 years (range, 20–90 years). Most (63%) patients were aged less than 50 years. Most MBC cases (2,806 patients [93.9%]) had T1 or T2-stage disease. A total of 2,449 (82.0%) patients had ALN negativity. Of the 493 (16.5%) patients with ALN metastasis, 381 (77.3%) and 112 (22.7%) had 1–3 and more than 4 metastases, respectively. In total, 2,581 (86.4%) and 2,143 (71.7%) patients were ER-positive and HER-2 negative, respectively. Of the 2,581 ER-positive patients, 2,135 (82.7%) had no ALN metastasis and 413 (16.0%) had ALN metastasis. Furthermore, 1,416 (47.4%) patients had received chemotherapy, 1,252 (42.0%) patients had not received chemotherapy, and 317 (10.6%) patients had no information about chemotherapy in the database. Among the 1,416 patients who received chemotherapy, 1,182 were ER-positive. Of the 1,182 ER-positive patients who underwent chemotherapy, 348 (29.4%) had ALN metastasis and 826 (70.4%) did not. During the study period, 190 (6.4%) deaths occurred, 57 (1.9%) of which were breast cancer-related. The detailed clinicopathologic characteristics of the patients with MBC are described in Table 1.
Table 1
Clinicopathological characteristics of all MBC, ER(+) MBC, and ER(+) MBC with node(+) patients

Values are presented as number (%).
MBC = mucinous breast cancer; ER = estrogen receptor; LVI = lymphovascular invasion; BCS = breast conserving surgery; SLNB = sentinel lymph node biopsy; ALND = axillary lymph node dissection; PR = progesterone receptor; HER-2 = human epidermal growth factor receptor 2.
![]()
Prognostic factors in MBC
Univariate and multivariate analyses were performed to identify the prognostic factors influencing BCSS and OS in all MBC patients (Table 2). In univariate analysis, old age (> 50 years), pathologic tumor stage, pathologic nodal stage, p53, LVI, radiotherapy, hormone therapy, chemotherapy, and hormone receptor (ER and PR) negativity significantly influenced BCSS. In multivariate analysis, pathologic nodal stage and ER negativity were significant prognostic factors for BCSS. Meanwhile, univariate analysis showed that old age (> 50 years), pathologic tumor stage, pathologic nodal stage, LVI, radiotherapy, hormone therapy, HER-2 negativity, and ER and PR negativity significantly influenced OS. Of these, old age (> 50 years), pathologic tumor stage, and pathologic nodal stage were significant prognostic factors for OS in multivariate analysis. However, omission of adjuvant chemotherapy in multivariate analysis did not significantly improve the prognosis for BCSS (HR, 0.577; 95% CI, 0.101–3.286; p = 0.535) or OS (HR, 0.840; 95% CI, 0.602–1.172; p = 0.306).
Table 2
Univariate and multivariate Cox regression analyses for BCSS and OS in all mucinous breast cancer patients

BCSS = breast cancer-specific survival; OS = overall survival; HR = hazard ratio; CI = confidence interval; LVI = lymphovascular invasion; ER = estrogen receptor; PR = progesterone receptor; HER-2 = human epidermal growth factor receptor 2.
![]()
Prognostic factors in ER-positive MBC
We performed a subgroup analysis of 2,581 ER-positive patients. Univariate and multivariate analyses were performed to identify the prognostic factors affecting BCSS and OS in this subgroup (Table 3). In univariate analysis, old age (> 50 years), pathologic nodal stage, radiotherapy, and chemotherapy significantly influenced BCSS, but pathologic nodal stage was the only significant prognostic factor in multivariate analysis. Regarding OS, old age (> 50 years), pathologic tumor stage, pathologic nodal stage, LVI, HER-2 status, and radiotherapy were statistically significant in univariate analysis. However, in multivariate analysis, only old age (> 50 years), pathologic tumor stage, and pathologic nodal stage remained statistically significant prognostic factors for OS. Meanwhile, omission of adjuvant chemotherapy in multivariate analysis did not significantly improve the prognosis for either BCSS (HR, 0.393; 95% CI, 0.106–1.453; p = 0.162) or OS (HR, 0.818; 95% CI, 0.549–1.220; p = 0.326) in ER-positive MBC with ALN metastasis (Supplementary Table 1).
Table 3
Univariate and multivariate Cox regression analyses for BCSS and OS in estrogen receptor-positive mucinous breast cancer
BCSS = breast cancer-specific survival; OS = overall survival; HR = hazard ratio; CI = confidence interval; LVI = lymphovascular invasion; PR = progesterone receptor; HER-2 = human epidermal growth factor receptor 2.
![]()
Efficacy of chemotherapy for MBC
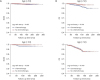
The efficacy of adjuvant chemotherapy for the 2,581 ER-positive MBC patients was analyzed according to pathologic tumor and nodal stage and age. The 5-year and 10-year BCSS of ER-positive MBC patients were 99.2% and 98.3%, respectively, while the 5-year and 10-year OS were 97.8% and 94.3%, respectively. The 5-year and 10-year BCSS of ER-positive MBC with ALN metastasis were 97.9% and 95.9%, respectively, while the 5-year and 10-year OS were 95.5% and 88.7%, respectively. The Kaplan-Meier curves for BCSS and OS based on pathologic tumor stage revealed that chemotherapy did not statistically significantly improve the prognosis (Figure 1). There were significant differences in BCSS in T1 stage disease depending on whether or not chemotherapy was performed, and the BCSS was longer in patients who did not receive chemotherapy. In the analysis for OS among patients with T3 disease, the adjuvant chemotherapy group showed a better OS than that of the group without adjuvant chemotherapy, but the difference was not statistically significant. Comparison of the chemotherapy efficacy was difficult in the analysis of BCSS and OS in patients with T3 and T4 stage disease due to the small number of patients in these groups. When stratified by pathologic nodal stage, the Kaplan-Meier curves for BCSS and OS also showed no statistically significant difference based on chemotherapy except for the N3 stage (Figure 2). It was difficult to obtain meaningful results for pathologic N2 and N3 stage disease because of the small number of patients. When stratified by age, the Kaplan-Meier curves of BCSS and OS showed no significant difference between younger (≤ 50 years) and older (> 50 years) patients. However, BCSS and OS differed significantly between older (> 50 years) and younger (≤ 50 years) patients. The results showed better survival when chemotherapy was omitted (Figure 3).
 | Figure 1Kaplan-Meier curve of (A) BCSS and (B) OS rates according to chemotherapy in estrogen-receptor-positive mucinous breast cancer patients, stratified by pathologic tumor stage.BCSS = breast cancer-specific survival; OS = overall survival.
|

Discussion
This study investigated the need for chemotherapy in the treatment of ER-positive MBC. Our findings showed that adjuvant chemotherapy did not significantly improve BCSS and OS in most MBC patients. We also found a good prognosis of MBC, similar to previous reports [69]. Among patients with ER-positive MBC, ALN metastasis was a significant prognostic factor for BCSS, while old age, pathologic tumor, and ALN metastasis were significant prognostic factors for OS.
MBC is a relatively rare histologic type of tumor that accounts for only 1%–6% of all breast cancers. MBC is characterized by a large amount of extracellular mucin [16]. Previous studies have shown that MBC has characteristics different from those of other invasive breast cancers, including high ER/PR expression, less ALN metastasis, and lower HER-2 expression [91718], which were also observed in our study. Due to these characteristics, MBC has a better prognosis than those of other invasive breast cancers. MBC can be divided into pure MBC (pMBC) and mixed MBC (mMBC) depending on the quantification of cellularity [19]. pMBC consists exclusively of tumor tissues with mucinous components above 90% while mMBC contains mucinous areas covering more than 50% but less than 90% of the total area, as well as admixing, usually with an infiltrating ductal epithelial component [20]. Recent studies have evaluated the differences in clinicopathological features and survival between pMBC and mMBC [132122]. Nodal positivity in pMBC ranges from 2%–14% [12123], compared to 46%–64% in mMBC [2721]. However, the KBCR does not provide data to distinguish between the histologic subtypes of MBC. Most patients in our study were thought to have pMBC because 16.5% had axillary nodal positivity.
The NCCN guidelines consider hormone receptors to play an important role in the treatment of MBC. Hormone receptor-positive patients are recommended to consider chemotherapy if they have ALN metastasis, whereas adjuvant chemotherapy is not recommended for patients without metastatic ALN. Meanwhile, because ER-negative MBC has a poor prognosis, the recommended treatment strategy is similar to that for other breast cancers [10]. Our results revealed that ER-negativity had a significant effect on BCSS. Due to the low prevalence, limited follow-up period, and good prognosis, few studies on MBC have been conducted, and most of the previous studies had a small sample size. The clinicopathologic factors affecting the prognosis of MBC are unclear. Furthermore, most treatment guidelines for adjuvant chemotherapy of MBC were derived from IDC treatment experiences [14] and have not been rigorously validated [11]. Therefore, the treatment guidelines should be validated to establish more appropriate guidelines for MBC.
Some studies have identified ALN metastasis as the strongest predictor of disease-specific survival because most patients presenting with LN metastases develop distant metastasis [1322]. In our study, ALN metastasis was also the most significant prognostic factor for BCSS and OS. Old age (> 50 years) and pathologic tumor stage were significant factors for OS. Previous studies revealed local or distant recurrence in some MBC patients. As such, many clinicians administer adjuvant chemotherapy similar to those for other breast tumors despite the good prognosis of MBC [61112]. This trend was consistent with our findings. In our study, 1,415 (47.4%) patients received adjuvant chemotherapy; of them, 1,181 patients were ER-positive. However, in contrast to the guidelines, 826 of 1,945 MBC (42.5%) patients with positive ER expression but without ALN metastasis received adjuvant chemotherapy. Current guidelines recommend adjuvant chemotherapy in MBC patients with ER positivity and ALN metastasis [10]. In our study, 348 of 384 (90.6%) patients were administered chemotherapy. These results show that, contrary to guideline recommendations, a large number of patients with MBC undergo chemotherapy in the real world.
Recent studies have reported that luminal breast cancer patients do not equally benefit from adjuvant chemotherapy [242526]. Furthermore, clinical trials have shown that adjuvant chemotherapy may not be necessary even in cases with ALN metastasis or large tumor size in luminal breast cancer [27]. Gene expression profiles have been developed to identify the individual risk of recurrence to avoid unnecessary adjuvant cytotoxic chemotherapy [28]. Chemotherapy is also less effective in MBC because of the higher ER and PR and lower HER-2 expression. These observations suggest that adjuvant chemotherapy can be omitted in MBC, which generally has a good prognosis. However, gene expression profiles cannot be used to predict recurrence risk in MBC due to the abundant mucinous content [11]. Therefore, we investigated the benefit of adjuvant chemotherapy in ER-positive MBC. Several clinical studies have already shown a good prognosis in MBC patients, even those with high-risk factors [71322].
When stratified by pathologic tumor stage, pathologic nodal stage, and age, our Kaplan–Meier curve analysis revealed that, except for N3 stage, adjuvant chemotherapy did not significantly improve BCSS and OS. We did not obtain significant results in pathologic T stage analysis for BCSS and OS due to the sample sizes of T3 and T4 patients. In our study, 94.5% of patients with ER-positive MBC had T1 and T2 stage disease. Pathologic N stage analysis showed differences in BCSS and OS between the chemotherapy and no chemotherapy groups for N2 and N3-stage disease. Only N3 stage showed a significant difference. However, the sample size was too small to interpret these results. N2 and N3-stage disease is also extremely rare among ER-positive MBC patients, accounting for only 3.3% of cases. Further studies are warranted to determine the efficacy of chemotherapy in a larger number of patients with other stages of disease. Our study found that most ER-positive MBC patients had T1 or T2 or N1-stage disease and that chemotherapy did not improve survival in most of these patients. The results of our multivariate analysis also indicated that the omission of adjuvant chemotherapy did not have a significant effect on BCCS and OS, despite the presence of ALN metastasis. Analysis of BCSS and OS for N1 stage showed a lower OS than BCSS in the no chemotherapy group, but the difference was not statistically significant. These results suggest that the patients who did not receive chemotherapy had a higher rate of other-cause deaths because of underlying disease or old age.
Our study had several limitations. First, the KBCR does not record the type of MBC as pure or mixed and provides no detailed information about recurrence. Second, because of the retrospective and voluntary nature of the KBCR, a large portion of data were missing, particularly regarding pathologic details and treatment. These missing data may have affected our results. Furthermore, it is difficult to reach a definitive conclusion due to the retrospective study design. Despite these limitations, our study is valuable in that, to the best of our knowledge, it is the first to investigate the efficacy of adjuvant chemotherapy in ER-positive MBC patients. Our study was also among the few large-scale MBC studies with a relatively long-term follow-up. Further, the KBCR is a nationwide database that prospectively collects data from more than 65% of patients undergoing breast cancer surgery in Korea; thus, our findings may be representative of all women with breast cancer in Korea.
In conclusion, the results of this large retrospective analysis revealed that adjuvant chemotherapy does not improve the prognosis in most ER-positive MBC patients, regardless of ALN metastasis. The good prognosis of patients with MBC was also confirmed. Furthermore, the pathologic nodal stage was the most important factor influencing patient prognosis. Ultimately, adjuvant chemotherapy can be omitted in the treatment of most ER-positive MBC.
 XML Download
XML Download