

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Warfarin is an oral anticoagulant used for the prevention and treatment of thromboembolic events [1]. Because of its narrow therapeutic index and significant interindividual variation in dose requirements, individualized dose adjustment is important for patient management. The most important factors affecting warfarin dose are VKORC1 and CYP2C9 polymorphisms, which explain approximately one-third of interindividual variations [23]. Pharmacogenetic-guided dosing decreases the time-to-stable doses and increases the percent time in therapeutic range compared with standard dosing [4].
Although these algorithms predict dosing requirements accurately in most patients, underestimations have been frequently observed in patients with higher dose requirements [567]. The meta-analysis conducted by Saffian, et al. [7] showed that all 22 algorithms included in the study underpredicted the warfarin dose for patients with a higher dose requirement. This can result in insufficient anticoagulation, leading to thrombotic events. In addition, because these algorithms show different performance depending on ethnicity, an ethnicity-specific algorithm is more appropriate for accurate dose prediction [8].
The VKORC1 1173C>T (complete linkage disequilibrium with −1639G>A, D′=1 and r2=1) is a common variant in the Asian population (82–96%) [1910]. Because of its association with warfarin sensitivity, patients with 1173CT and 1173CC genotypes require higher warfarin doses than patients with the 1173TT genotype [11]. Likewise, the high frequency of VKORC1 1173C>T in Asian populations can explain the lower warfarin dose requirements in Asians compared with those in Caucasians and Africans [9]. In our previous study, we evaluated the performance of 16 previously published warfarin dosing algorithms [6]. The 16 algorithms worked well for VKORC1 1173C non-carriers. However, they showed poor prediction performance in VKORC1 1173C carriers. An algorithm more suitable for VKORC1 1173C carriers is required for proper warfarin treatment and may be more important in populations with a high proportion of VKORC1 1173C carriers. Therefore, we developed and validated a new warfarin dosing algorithm for VKORC1 1173C carriers and compared its performance with that of previously published algorithms. This is the first study to develop and validate a warfarin dosing algorithm based on data from VKORC1 1173C carriers.
METHODS
Patients
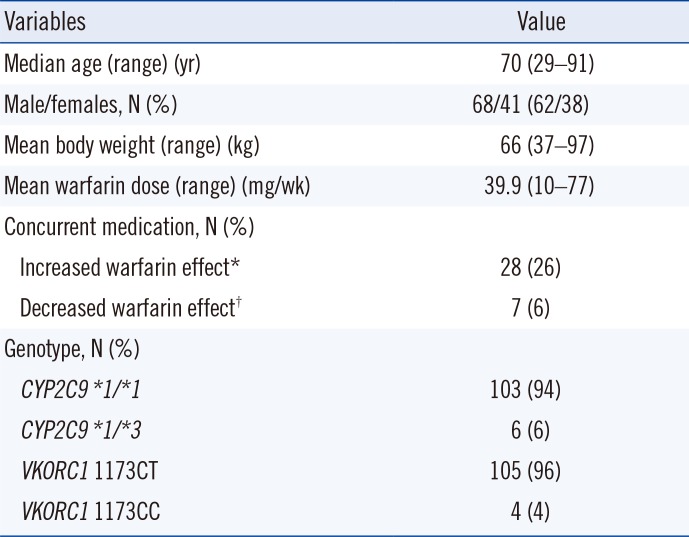
A total of 482 Korean patients with atrial fibrillation, cerebral infarction, or deep vein thrombosis/pulmonary embolism or patients undergoing valve replacement who were receiving warfarin treatment from 2006 to 2017 at the Samsung Medical Center, Seoul, Korea, were genotyped for CYP2C9 and VKORC1. After excluding 373 patients with the VKORC1 1173TT genotype, 109 patients with VKORC1 1173C were included. We retrospectively reviewed the clinical and laboratory data of these patients. Patient characteristics are presented in Table 1. High interindividual variation in actual dose was observed (median, 37 mg/week; range, 10–77 mg/week). For the VKORC1 genotypes, 96% of patients were heterozygous (VKORC1 1173CT) and 4% of patients were homozygous for the C allele (VKORC1 1173CC). For the CYP2C9 genotypes, 94% of patients had a *1/*1 genotype and 6% of patients had a *1/*3 genotype. All six patients with CYP2C9
*1/*3 had VKORC1 1173CT. None of the patients had CYP2C9
*1/*3 with VKORC1 1173CC. CYP2C9 and VKORC1 genotyping was performed using direct sequencing as described in our previous study [612]. This study was approved by the Institutional Review Board of Samsung Medical Center.
Development and validation of the new dosing algorithm
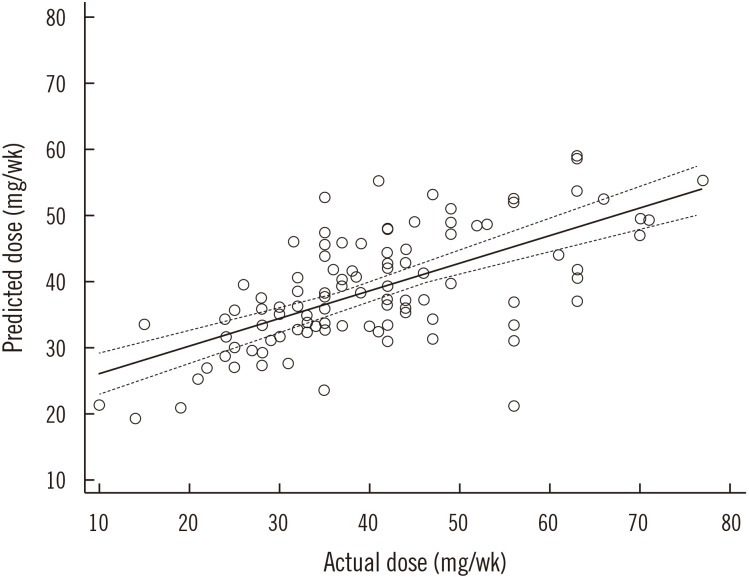
To develop the warfarin dosing algorithm, multiple linear regression analysis with backward variable selection was performed using the following clinical data and the genotyping results of the 109 patients: age, body surface area (BSA), sex, smoking, deep vein thrombosis, stroke, hypertension, diabetes mellitus, congestive heart failure, CYP2C9 genotype, and VKORC1 genotype. The distribution of warfarin dose was non-parametric, and warfarin dose was log-transformed for analysis. To evaluate the performance of our model, we used leave-one-out cross validation (LOOCV), which was deemed as the appropriate method because of the small study population. The i-th patient (i=1,…, 109) was divided from whole data as the test set and the remaining 108 patients as the training set [13]. Multiple linear regression analysis with backward variable selection was applied to the training set to fit a prediction model. A fitted prediction model was applied to the test set, and the predicted warfarin dose was calculated. This process was repeated for all patients. A scatter plot of the actual warfarin dose and predicted warfarin dose was generated after LOOCV, and its Spearman's correlation coefficient (ρ) was calculated. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Algorithm evaluation
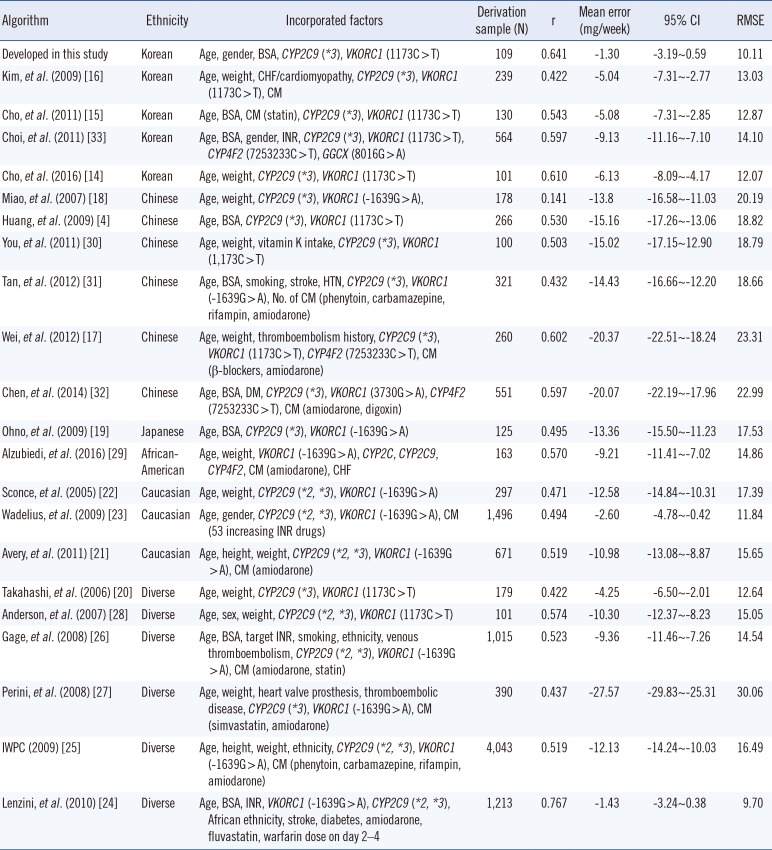
For performance evaluation, the developed algorithm was compared with previously suggested ones. A total of 21 algorithms [41415161718192021222324252627282930313233], including CYP2C9 and VKORC1 genotypes, were selected through literature searches of PubMed for genotype-guided warfarin dosing algorithms published in the 2007–2017 period. We used a combination of search terms including warfarin, CYP2C9, VKORC1, dosing, dose prediction, algorithm, genotype-guided, and pharmacogenetic. Of the identified algorithms, we selected those published in English and those derived using the data of more than 100 patients. The 109 patients used for algorithm development were also included in the evaluation. The predictive performance of each algorithm was compared using the ρ of actual dose and estimated dose, mean error with 95% confidence interval (CI), and root mean square error. The actual maintenance dose was determined based on the weekly prescribed dose at three consecutive clinic visits when the international normalized ratio (INR) measurements were within the target range. The estimated dose was calculated for all tested algorithms using the incorporating factors of each algorithm. The value of ρ was interpreted as follows: negligible correlation (0–0.3), low correlation (0.3–0.5), moderate correlation (0.5–0.7), high correlation (0.7–0.9), or very high correlation (0.9–1.0) [34]. Mean error was calculated by subtracting the actual dose from the estimated dose. In addition, the percentages of patients with underestimated, ideal, and overestimated doses were evaluated. Patients with underestimated, ideal, and overestimated doses were defined as patients whose estimated dose was >20% lower than the actual dose, within 20% of the actual dose, and >20% higher than the actual dose, respectively.
RESULTS
Using multiple linear regression analysis, age, BSA, sex, CYP2C9 genotype, and VKORC1 genotype were selected for developing a warfarin dosing algorithm. The developed equation is as follows:
maintenance dose (mg/week)=exp[3.223−0.0094×(age)+0.577×(BSA)+0.178×(sex)−0.481×(CYP2C9 genotype)+0.227×(VKORC1 genotype)]
where exp is the exponential function.
In the case of females, the CYP2C9
*1/*3 genotype, or the VKORC1 1173CC genotype, it was coded as 1, while in the case of males, the CYP2C9
*1/*1 genotype, or the VKORC1 1173CT genotype, it was coded as 0. The developed algorithm explained 44% of the interindividual variations in the maintenance dose (ρ=0.641, P<0.0001). The LOOCV result is presented in Fig. 1. The ρ value between the actual and leave-one-out predicted dose was 0.664 (95% CI=0.543–0.757, P<0.001).
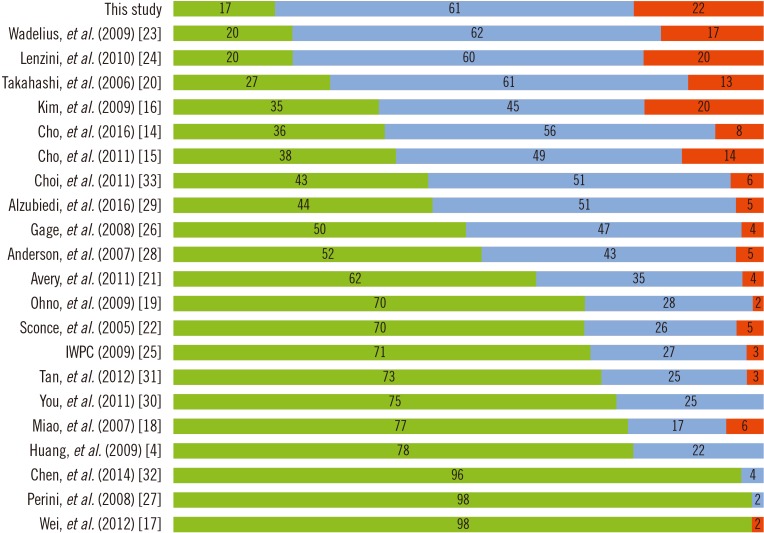
The ρ and mean error of the developed algorithm and the other 21 algorithms are presented in Table 2. The common factors included in all 22 algorithms were age, CYP2C9 genotype, and VKORC1 genotype. Ethnicity varied across the algorithms: five were derived from data of Koreans; six, from Chinese; one, from Japanese; three, from Caucasians; one, from African-Americans; and six, from diverse populations. The developed algorithm showed moderate correlation (ρ=0.641) and had the lowest mean error (−1.30 mg/week). The ρ and mean error of the other 21 algorithms ranged from 0.141 to 0.767 and from −1.43 to −20.37 mg/week, respectively. Of all 22 algorithms, the developed algorithm had the lowest proportion of underestimated groups (17%, Fig. 2). The algorithm by Lenzini, et al. [24] showed better correlation (ρ=0.767) than the developed algorithm; however, the performance, evaluated by the mean error and the proportion of underestimated groups was better for our algorithm.
DISCUSSION
Previously, we reported that warfarin dosing algorithms showed poor prediction performance in VKORC1 1173C carriers [6]. In that study, all 16 evaluated algorithms showed increased mean error in the VKORC1 1173C carrier group compared with that in the VKORC1 1173C noncarrier group. Here, we developed and validated a new warfarin dosing algorithm to predict maintenance doses for VKORC1 1173C carriers.
Previously, we developed a warfarin dosing algorithm with a derivation cohort that included 24.6% (32/130) VKORC1 1173C carriers [15]; by contrast, the present study included 100% VKORC1 1173C carriers. The derivation cohorts of the two studies were derived from the same hospital and showed very similar characteristics in terms of age, male:female ratio, body weight, and CYP2C9 genotype. Therefore, the different performance of the two algorithms could be caused by the different proportion of VKORC1 1173C carriers included in the derivation cohorts.
Considering the proportion of underestimated groups, the best-performing algorithm was the present algorithm, followed by those of Wadelius, et al. [23], Lenzini, et al. [24], and Takahashi, et al. [20]. The algorithms of Lenzini, et al. [24] and Wadelius, et al. [23] had the same proportion of underestimated groups (20%). The algorithm by Lenzini, et al. [24] had lower mean error, possibly due to the inclusion of Asian populations in the derivation cohort, and better correlation (ρ=0.767) compared with the present algorithm. However, the newly developed algorithm showed better performance, as estimated by mean error and the proportion of underestimated groups.
Although not the best, the algorithms derived from the data of Korean populations [14151633] showed relatively good performance even with low proportions of VKORC1 1173C carriers in the derivation cohort (Table 2; Fig. 2). In contrast, most of the algorithms derived from the data of different ethnic populations showed poor performance despite the high proportion of VKORC1 1173C carriers in the derivation cohort. These findings suggest that ethnicity is as important as VKORC1 genotype in predicting warfarin dose. Indeed, several studies have addressed the importance of developing ethnicity-specific warfarin dosing algorithms [568]. The current genotype-guided dosing algorithms were developed primarily based on the data from Caucasian populations and do not include genetic variants that are frequently found in non-Caucasian populations [2325]. The four algorithms derived from the data of Korean populations [14151633] were developed from derivation cohorts including 5.6–24.6% of VKORC1 1173C carriers. The proportion of VKORC1 1173C carriers was inevitably low in randomly selected derivation cohorts owing to the high frequency of VKORC1 1173C>T in the Asian population [1]. Because of the lower proportion of VKORC1 1173C carriers in the derivation cohort, these four algorithms showed a relatively higher mean error and higher proportion of underestimated groups than our algorithm. Therefore, the present algorithm developed for VKORC1 1173C carriers would be more helpful in Asian populations than in other ethnic populations.
Previous algorithms were developed mainly through multilinear regression analysis using clinical and genetic factors. A recent meta-analysis revealed that previous algorithms underestimated warfarin doses in patients requiring high doses, thus requiring the development of new algorithms for these patients [7]. To eliminate the bias effects caused by genetic factors, such as VKORC1 variants, developing ethnicity-specific algorithms similar to that by Limdi, et al. [8] could be a simpler approach. Therefore, the present algorithm, developed by regression analysis of clinical factors, is valuable because we targeted only specific genotype groups. We controlled the influence of VKORC1 1173C, which has significant effects on warfarin resistance in Koreans. However, these findings will require future validation in other ethnicities with VKORC1 1173C.
This study has several limitations. First, because of the small study population, we did not have an independent validation cohort. Therefore, performance evaluation was advantageous for our algorithm than for other algorithms developed using derivation cohorts with different characteristics. To overcome this limitation, we used LOOCV for performance evaluation. Further large-scale studies are required to validate our results. Second, we did not include the INR response in our analysis. According to Horne, et al. [35], incorporation of the INR response improves the performance of a warfarin dosing algorithm. However, as with our algorithm, most of the previous algorithms did not include the INR response. Third, our algorithm was not tested on other ethnic populations. Because ethnicity-specific algorithms are better than pan-ethnic algorithms, our algorithm may not work well in other ethnic populations. However, the primary goal of our study was to develop a more accurate algorithm for Korean VKORC1 1173C carriers. Fourth, although our algorithm had the lowest proportions of underestimated groups, 17% of patients were still underestimated. Therefore, our algorithm was not perfect and had a negative bias for some patients with higher dose requirements. Further studies are required to improve the performance of the algorithm for VKORC1 1173C carriers.
The algorithm developed in this study showed the best performance compared with 21 other algorithms. A warfarin dosing algorithm suitable for VKORC1 1173C carriers should be used to minimize the underestimation of warfarin dosing in these patients. It will enable proper treatment and reduce the risk of thromboembolism in VKORC1 1173C carriers.
 XML Download
XML Download