

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The worldwide increase in the incidence of adenocarcinomas of the esophageal gastric junction (AEG) may be attributed to increasing age, gastroesophageal reflux, and Barrett esophagus [1234]. In 1998, depending upon the anatomical lesion located in the cardiac region of the stomach, Siewert and Stein [5] proposed a classification consisting of 3 different cancer types. This classification has been adopted for AEG type I–III tumors [5]. AEG type II tumors, so-called the true carcinomas of the cardia, are often associated with Barrett esophagus [6]. They are localized in the metaplastic area, about 1 cm proximal to and 2 cm distal from the esophagogastric junction [6]. Standardized surgical therapy for AEG type II tumors requires extended gastrectomy and distal esophagectomy [57].
Extended gastrectomy is oncologically safe for the surgical treatment of AEG type II tumors [6]. The transhiatal approach presents an adequate alternative to the transthoracic access for distal esophagectomy and esophageal reconstruction. While the favorable choice for AEG II between transthoracic esophagectomy with gastric tube formation and intra-thoracic anastomosis (IvorLewis esophagectomy) and transhiatal extended gastrectomy remains controversial [8], the latter may be preferable with respect to postoperative morbidity and quality of life, provided that it is technically feasible and fulfills oncological principles [9].
To fulfill the requirements of minimum oral safety margins and satisfactory lymphadenectomy of the distal mediastinum, transhiatal management of the distal esophagus is crucial [101112]. Technically, it is mandatory to avoid the retraction of the esophageal stump toward the mediastinum. Furthermore, it is important to ensure minimal manipulation of the remaining esophageal stump by preventing trauma in the anastomosis region, in order to preserve the mucosal integrity for optimal perfusion. These are prerequisites for minimizing the risks of anastomotic dehiscence, leakage, and stenosis [1213].
Numerous different approaches have been developed and evaluated to improve the technical simplicity and safety of laparoscopic approaches for esophagojejunostomy in gastrectomy and extended gastrectomy. However, despite of laparoscopic evolution and its increasing acceptance, an open extended gastrectomy is still preferred as the most applicable technical approach, and to date, is still considered as the gold standard [14], especially with the limited involvement of the distal segment of the esophagus [15]. Particularly for AEG II, the open approach remains the preferred technique, because the extent of resection cannot be determined safely prior to surgery [9].
Here, we describe an easy and safe technical variant of handling the distal esophagus in the course of an open extended gastrectomy, entitled as the ‘dorsal track control (DTC)’ maneuver.
MATERIALS AND METHODS
Patients
Between January 2014 and October 2017, 21 patients with either AEG type II (n=8) or gastric carcinoma (n=13) underwent a surgical resection with curative intent at the Department of Surgery, Heinrich-Heine-University Hospital Duesseldorf, and the Department of General and Visceral Surgery, Protestant Hospital of Bethel Foundation, Germany. All 21 patients were operated with our modified DTC technique. The data collection procedure for this study was in compliance with the guidelines established by the Declaration of Helsinki and the study protocol was approved by the local ethics committee. AEG type II tumors were defined as adenocarcinomas located 1 cm proximal to and 2 cm distal from the esophagogastric region. The tumors were classified as AEG type II on the basis of radiological findings, endoscopical orthograde and retroflexed views of the esophagogastric junction, and intraoperative findings.
The clinical data of these patients, collected from their medical records, were compiled into an Excel®-file database and analyzed retrospectively. The following data was collected: demographic parameters including the age, sex, American Society of Anesthesiologists (ASA) score, and diagnosis; oncological characteristics including the tumor node metastasis (TNM) stage, R-status, and neoadjuvant chemotherapy; and surgical characteristics including the operation time, intensive care unit (ICU) stay, hospital stay, morbidity, and mortality and survival rates. Depending upon the diagnosis, the patients were divided into 2 groups: group I: gastric cancer with distal esophagojejunostomy and group II: AEG II with high esophagojejunostomy.
Surgical approach
All patients with AEG type II received a radical extended total gastrectomy with transhiatal resection of the distal esophagus, along with standard D2 and lower mediastinal en-bloc lymphadenectomies [16]. Reconstruction was accomplished by high esophagojejunostomy (Roux-en-Y). All patients with gastric carcinomas were operated by total gastrectomy with distal esophagojejunostomy (Roux-en-Y).
Description of the DTC
The novel DTC technique was developed to achieve non-traumatic handling of the distal esophagus in preparation for a circular-stapled esophagojejunostomy. It was based on a ventral semi-circular incision in the esophagus, at a level that provided a minimum safety margin of 3 cm cranial to the tumor margin, leaving the dorsal esophageal wall mechanically untouched, which in turn facilitated the traction control of the esophagus (naso-gastric tube in place) (Figs. 1A and 2A). Mechanical protection of the upper esophagus was achieved by redundancy of any maneuver that would directly interfere with the supra-anastomotic region, such as the fixation of the oral esophagus by clamping or securing it with temporary sutures; this provided tension towards the abdomen. Next, the purse-string suture was correctly positioned by holding the distal esophagus in one hand (for stabilization) in order to avoid any manipulation of the remaining intrathoracic esophagus (Fig. 1B and C, Fig. 2B). The dorsally-exposed epithelialized inner wall surface of the ventrally-opened esophagus served as a guiding chute that eased the insertion of the anvil into the upper esophageal lumen. This step was useful in preventing the retraction of the esophageal end towards the upper mediastinum (Fig. 1D). In most cases, this maneuver brought about a careful dilatation of the oral semi-circular opening of the esophagus, prior to anvil insertion (e.g. by utilizing Maier sponge forceps). Following the insertion of the circular stapler anvil into the upper esophageal lumen, the purse string-suture was tightly applied (Fig. 1E). The integrity and sufficiency of the purse-string tie was ensured prior to the completion of the esophagectomy by cutting the remaining dorsal wall of the esophagus just below the tie (Fig. 1F). In one case, we had to further resect the oral stump of the esophagus due to a positive resection margin. In preparation for the second DTC maneuver, we cut the ventral esophagus hemi-circularly, a few millimeters oral of the anvil and then cut the initial purse-string suture. Subsequently, we extracted the anvil and placed it on the side. Next, we flattened the distal esophagus stump horizontally and grasped the ventral and dorsal margins simultaneously with a strong angled overholt clamp; the latter served as a handle for applying an equable and continuous traction to the distal esophagus in the second DTC maneuver.
Fig. 1
Description of the DTC maneuver. (A) Transhiatal approach with lower mediastinal en-bloc lymphadenectomy. Ventral semi-circular incision in the esophagus at a level that provides a safety margin of minimum 5 cm cranial to the oral tumor. The posterior esophageal wall remains intact for traction control of the esophagus (naso-gastric tube in place). (B and C) Controlled positioning of the purse-string suture avoiding any manipulation of the remaining intrathoracic esophagus. One hand gently pulls down the esophagus by the posterior wall with DTC. (D) The dorsally-exposed epithelialized inner wall surface of the ventrally-opened esophagus serves as a guiding chute to ease the insertion of the anvil into the upper esophageal lumen; this is paralleled by preventing the retraction of the esophageal end towards the upper mediastinum. (E) Following the insertion of the circular stapler anvil into the upper esophageal lumen, the anvil attachment is tied by the purse string-suture. (F) Following the purse-string suture tie around the anvil attachment, the distal esophagus is cut just below.
DTC = dorsal track control.

Fig. 2
Intraoperative pictures for extended gastrectomy. (A) Semi-circular opening of the ventral esophagus with a safety margin of minimum 5 cm cranial to the oral tumor (naso-gastric tube in place). (B) The purse-string suture is carefully placed, under observation, by avoiding any manipulation of the esophagus stump. (C) The anastomosis will be placed up to 10 cm intrathoracic in the mid mediastinum.

Statistics
Statistical analysis and graphing were performed using MS Excel from Microsoft (Redmond, Washington, D.C., USA) and JMP 14.1 from SAS Institute Inc. (Cary, NC, USA). All results were expressed as mean±standard deviation. Statistical significance was determined by the Student's t-test and the χ2 test. The Kaplan-Meier method and log rank test were used to evaluate survival. Significance was defined as P<0.05.
RESULTS
We applied this novel DTC technique in 21 cases, in order to enable a safe anastomosis of 6–10 cm proximal to the Z-line, with en-bloc lymphadenectomy of the lower mediastinum. Eight patients were operated with DTC for AEG type II or gastric carcinomas involving the esophagogastric junction. Furthermore, DTC was performed without the neoplastic involvement of the Z-line in 13 gastric cancer patients. In one case, due to a positive oral resection margin (as observed on frozen section), an additional esophageal resection of 3 cm was required during the initial surgery (as described under material and methods). During the median observation time of 30.4 months (range: 16.3–61.1), there were no differences in the overall survival or disease-free survival rates between the 2 groups, as demonstrated by the log rank analyses, visualized by the Kaplan–Meier curves (Fig. 3A and B).
Fig. 3
Kaplan–Meier survival curve demonstrates similar OS and DFS rates in groups I (gastrectomy only, n=12) and II (gastrectomy + distal esophagectomy, n=8).
OS = overall survival; DFS = disease free survival.

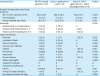
The patients' characteristics, according to the 2 groups (I: gastrectomy only; II: gastrectomy + distal esophagectomy) are presented in Table 1. Our 21-patient cohort consisted of 9 (43%) females and 12 (57%) males. The median age was 70 years (range: 44–88 years). Around 52% of the group I patients presented with an ASA score of 3, while 63% of the group II patients were scored as 2. However, the patients' characteristics did differ significantly between the 2 groups (P=0.13; Table 1). Furthermore, no intergroup differences in the TNM stage were observed (P=0.43). While patients with AEG II tumors were significantly treated more often with neoadjuvant chemotherapy than those with gastric carcinomas (75% vs. 31%; P=0.049), no difference was found in the adjuvant chemotherapy between the 2 groups (63% vs. 63%; P=0.097). Complete tumor resection (R0) was achieved in all 21 DTC-treated patients. Although the median operation time was longer in patients of group II than of group I (357±74 minutes vs. 298±56 minutes), the difference was not significant (P=0.08; Table 2). A non-significant trend of longer ICU stay was observed in the AEG II patients (5.9±3.2 days), as compared to that of group II (3.5±3.5 days; P=0.13). Gastrectomy patients were hospitalized for a median of 23 days, while extended gastrectomy patients had a median hospital stay of 15 days (P=0.13).
Table 1
Comparison of patient and oncological characteristics between groups I (gastrectomy only) and II (gastrectomy + distal esophagectomy)

Table 2
Comparison of surgical characteristics, morbidity, and outcomes between groups I (gastrectomy only) and II (gastrectomy + distal esophagectomy)
The complications were classified according to the Dindo–Clavien Score. No anastomotic leakage or stenosis was observed. Three patients (14.3%) showed an uneventful postoperative course without any complications (Table 2).
Minor complications (grades I–II) occurred in 15 patients (71%), while major complications (grades III–V) occurred in 3 patients (group I 15% vs. group II 13%; Table 2).
AEG II patients experienced an overall, more favorable complication rate (P=0.04, Table 2). Specific complications such as intestinal atony, delirium, lymphatic fistula, wound infection, urinary tract infection, anemia, pulmonary complications, or reflux esophagitis did not have a significant occurrence within the 2 groups. Four patients developed reflux esophagitis. Around 48% of the patients demonstrated other complications such as mesenteric ischemia, pancreatic fistula, clostridium difficile colitis, and heart insufficiency. We observed one case postoperative 30 day-mortality (4.7% overall) in the AEG II group. The multimorbid patient, child A, with liver cirrhosis, hypertension, lung emphysema, fibrosis, and infrarenal aortic aneurysm, developed fulminant mesenteric ischemia (unrelated to the surgery) on the 7th postoperative day.
DISCUSSION
Esophagojejunostomy is known to be quite challenging even under good visibility, especially in obese patients with a thick abdominal wall, which makes for a difficult and narrow exposure of the lower mediastinum [1718]. Even though mechanical circular-stapled anastomosis is the standard and widely-used technique for esophagojejunostomy, this procedure remains challenging, due to the risk of anastomotic leakage, with often fatal outcomes [13]. Although the postoperative morbidity rate in a transhiatal approach is lower than in transthoracic Ivor-Lewis-esophagectomy, the complication rate has been reported to be about 30% [81920212223]. In order to perform a safe esophagojejunostomy, the correct placement of the purse-string suture for fixing the anvil and facilitating its insertion into the oral stump of the esophagus is critical [1724]. The quality of these 2 steps are risk factors for anastomosis leakage or fistula [112526]. Both steps need to be performed with little-to-no manipulation of the oral esophagus adjoining the anastomosis. The latter is challenging, as purse-string suture placement followed by anvil insertion are paralleled by the tendency of the remaining esophagus stump to retract into the mediastinum [101112], which needs to be prevented during the procedure.
The DTC method was developed in order to fulfill the prerequisites of maintaining the tension on the oral esophagus (without manipulating it during purse-string suture placement and anvil insertion), tying the suture (including a proper option of securing the suture tie), and—if appropriate—correcting or improving the purse-string suture prior to the completion of the esophageal transection. Furthermore, while performing a lymphadenectomy of the lower esophagus, the surrounding upper esophageal tissue must be as minimally disrupted as possible, in order to avoid the unnecessary opening of the mediastinum.
Several approaches have been proposed to improve the purse-string suture placement [1125272829] and anvil insertion into the esophagus [3031]. For open gastrectomy in gastric cancer patients, Guerra et al. [11] proposed a technical modification for stapled transabdominal esophagojejunostomy, which involved opening the ventral wall of the esophagus, close to the esophagogastric junction, to precisely locate the purse-string suture under direct vision for preventing the retraction of the mucosa. However, compared to this approach, our DTC technique for AEG II may have several advantages. Guerra et al. [11] described a clockwise repetitive rotation with a right-angled clamp for continuous suturing of the purse-string suture, with the intention to improve the visibility of the posterior wall. In our opinion, a rotational maneuver of the esophagus, aboral to the prospective level of dissection, is technically not practical in the lower mediastinal cavity. This seems especially relevant for oncological en-bloc distal esophago-gastrectomy, which is required for AEG II. Furthermore, the repetitive turning of the lower esophagus may be unfavorable, as it may cause additional trauma to the proximal esophagus due to severe manipulation. In our experience, a gentle lifting of the dorsal part of the esophagus for consistent monitoring of the purse-string suture needle, without twisting the lower esophagus, is sufficient.
Another advantage of the DTC technique is the easy insertion of the anvil into the proximal esophagus. By gentle pulling the esophagus down and maintaining an unmanipulated tension on it, the posterior wall transforms into a guiding chute for the anvil. As the anvil can easily slide over the dorsal esophagus wall into the lumen, no additional traction or manipulation is needed, which otherwise may cause muscular contraction, mucosal tears, or anastomotic leaks [1213].
Instead of dissecting the dorsal part of the esophagus right after anvil insertion (prior to purse-string suture tying), as performed by others [11], our technique kept the integrity of the dorsal esophagus wall up to the point of tying and verifying the quality of the purse-string suture. In our experience, the latter improves the training of the surgical procedure, as the trainee has more time to safely perform the mandatory steps and the trainer has the opportunity to control these steps; he is in the position, if necessary, to improve the anvil position and purse-string suture prior to releasing the manipulation-free tension from the upper esophagus. The DTC technique may increase the safety of the surgical training for total or extended gastrectomy for performing a safe and leakproof anastomosis. In this study, no anastomotic leakage or stenosis was observed. Another advantage of DTC is the possibility of safely redoing the anastomosis without any additional risk, in case of damage or tumor infiltration in the resection margin. By grasping the stump of the oral esophagus with a curved or angled clamp, the surgeon can provide tension to the upper esophagus in an unrestricted manner in the first approach, with the option to retrace the same sequence of steps, as described for the initial DTC-maneuver.
This surgical technique supports the prospects of avoiding the transthoracic approach for intra-thoracic anastomosis in selected cases of esophagojejunostomy for AEG II patients. Furthermore, by applying the DTC technique, it is possible to perform an anastomosis in the mid mediastinum, 8–10 cm above the Z-line, as demonstrated in the intraoperative image and in a representative CT scan (Figs. 2C and 4). This is extremely important for tumors located in the lower mediastinum; transthoracic esophagectomy with proximal gastric resection, which is known to carry an increased morbidity risk, can be avoided [632].
Fig. 4
Pre-(left panels) and post-(right panels) operative thoraco-abdominal computed tomography-scans of 1 patient operated with the dorsal track control technique (blue ovals—localization of the adenocarcinoma of the esophagogastric junction II; yellow arrows—position of the intrathoracic esophagojejunostomy after transhiatal extended gastrectomy).
Pre-op = pre-operative; Post-op = post-operative.

One limitation of our study is the low number of patients. Furthermore, we did not evaluate the long-term outcomes with respect to anastomotic stenosis. Although the DTC approach seems to safely improve the preparation for esophageal anastomosis, this technique needs to be validated in a larger number of patients.
 XML Download
XML Download