

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite the decreasing global incidence, gastric cancer is one of the most common malignancies and a common cause of cancer-related mortality in Eastern countries [1]. Curative surgery, including gastric resection and regional lymph node dissection, is the only effective treatment for gastric cancer [2]. Laparoscopic surgery was initially introduced for gastric cancer in 1994 [3] and has been widely accepted as a good alternative to open surgery in Korea [4] because of faster postoperative recovery, shorter hospital stay, lower morbidity, and better patient satisfaction [5]. More recently, large multicenter randomized trials in Korea (KLASS-01) [6] and China (CLASS-01) [7] have demonstrated the long-term oncological outcomes of laparoscopic gastrectomy for both early- and advanced-stage gastric cancer.
The incidence of surgical site infection (SSI) after gastric surgery was approximately 5%–9% in previous studies [8910]. The prophylactic use of antibiotics has long been the mainstay of preventing SSIs after abdominal surgeries [11]. However, most studies suggesting the efficacy of prophylactic antibiotics were conducted decades ago and included only patients undergoing open surgery [1213]. Laparoscopic surgery is associated with a lower incidence rate of SSIs due to minimal skin incision, non-exposure of the visceral organs, and less inflammatory response postoperatively. Previous studies have reported an SSI incidence of <5% after laparoscopic gastrectomy, which was significantly lower than that after open surgery [141516]. This may make the role of routine prophylactic antibiotics debatable in minimally invasive procedure. However, the efficacy of prophylactic antibiotic use has rarely been investigated in patients undergoing laparoscopic gastrectomy for early gastric carcinoma [17]. In this study, we investigated the risk of postoperative SSIs with and without prophylactic antibiotic use in total laparoscopic distal gastrectomy (TLDG) for gastric carcinoma.
MATERIALS AND METHODS
Patients and data
We retrospectively enrolled 71 patients with gastric carcinoma who underwent TLDG between 2014 and 2016 at our institution without antibiotic prophylactic use (non-prophylactic group). The inclusion criteria were as follows: clinical stage cT1N0, age of 18–65 years, European Cooperative Oncology Group performance status 0 to 1, and no preoperative malnutrition (body mass index [BMI] ≥18 kg/m2 and no preoperative weight loss). Patients who underwent combined organ resection other than cholecystectomy or emergency operation due to bleeding or perforation or had previous upper abdominal operation history were excluded. We also identified 393 patients who met the same inclusion and exclusion criteria and underwent TLDG during the same period with antibiotic prophylactic use (prophylactic group) (Fig. 1). This study was approved by the Institutional Review Board of Chonnam National University Hwasun Hospital. The board waived the requirement for patient informed consent (CNUHH-2018-043).
Fig. 1
Flow diagram of the study.
TLDG = total laparoscopic distal gastrectomy; BMI = body mass index; ASA = American Society of Anesthesiologists.

The patients in the non-prophylactic group did not receive prophylactic antibiotics during the surgery. Instead, non-pharmacological SSI preventive measures, such as preoperative whole-body bathing using an antimicrobial soap, maintenance of intraoperative normothermia, and postoperative high oxygen supplementation, were strictly performed in these patients. The patients in the prophylactic group received cefazoline 1 g before skin incision, and an additional dose was administered when the surgery was prolonged >3 hours. There was no extended postoperative antibiotic use in these patients.
The operative procedures, including gastric resection and lymph node dissection, were performed as described in the Korean gastric cancer treatment guideline [2]. All patients underwent TLDG with an intracorporeal anastomosis, and the choice of reconstruction type was at the surgeons' discretion. Briefly, we used four to 5 abdominal ports, including an umbilical port for the laparoscope. During anastomosis, intra-abdominal spillage of bowel contents was strictly avoided. At the end of surgery, intra-abdominal irrigation of 500–1,000 mL was routinely performed. Gastric specimen was extracted via 2–3-cm extension of the umbilical port site. Both groups received perioperative management using the same Enhanced Recovery After Surgery (ERAS) protocol, which included avoidance of preoperative fasting, no routine use of a nasogastric tube or abdominal drainage, early postoperative oral nutrition, restrictive intravenous fluid administration, and early active ambulation.[18]
Data on patients' clinicopathological characteristics, operative procedures, and postoperative outcomes were retrospectively collected from the medical records and gastric cancer database. Postoperative complications were defined as any complications that developed within 30 postoperative days and divided into local and systemic complications according to their development site. The severity of complications was graded based on the Clavien-Dindo classification of surgical complications [19]. SSI was defined according to the diagnostic criteria of the National Nosocomial Infections Surveillance system by the Centers for Disease Control and Prevention (CDC) and classified as superficial incisional, deep incisional, and organ/space infection [20].
Propensity score matching
We matched the two patient groups using the propensity score matching method (Fig. 1). The patient's demographic and clinical characteristics, such as age, sex, BMI, comorbidities, American Society of Anesthesiologists (ASA) physical status score, previous cholecystectomy, reconstruction type, lymph node dissection type, omentectomy type, operative time, and operative bleeding, were included in the binary logistic regression model to generate the propensity score. Using the propensity score, the patients were matched in a 1:1 ratio by the nearest neighboring method (caliper of 0.2). After the matching, the quality of the matching result was examined by the distribution of the propensity score and standardized difference.
Statistical analysis
The Student's t-test was used to compare the continuous variables, and the chi-square or Fisher's exact test was used to compare the categorical variables, as appropriate. In the matched sample, the continuous variables were compared using the paired t-test, and the categorical variables were compared using McNemar's test, considering the nature of the matched data [21]. All statistical analyses, including the propensity score matching, were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Two-sided P-values <0.05 were considered statistically significant.
RESULTS
The study subjects comprised 300 men and 164 women with a mean age of 53.2±7.8 years. The mean BMI was 23.5±3.2 kg/m2. Of the 464 patients, 263 (56.7%) had underlying comorbidities. D1+ and D2 lymphadenectomy were performed in 364 (78.5%) and 100 (21.5%) patients, respectively, and combined cholecystectomy was performed in 20 (4.3%) patients. Before the matching, the two groups showed a significant difference in age, comorbidities, ASA physical status score, previous cholecystectomy, reconstruction type, lymphadenectomy type, operative time, and operative bleeding. The patients in the non-prophylactic group were younger and had fewer comorbidities, and D2 lymphadenectomy was less frequently performed in this group. The final pathological stage was not significantly different between the two groups. After the matching, the two groups showed well-balanced baseline characteristics without significant intergroup differences in the matching variables (Table 1).
Table 1
Patient characteristics before and after propensity score matching

Data are expressed as mean±standard deviation or number (%).
BMI = body mass index; ASA = American Society of Anesthesiologists; TNM = tumor, node, and metastasis; AJCC = American Joint Committee on Cancer; UICC = Union for International Cancer Control.
*The seventh edition of AJCC/UICC TNM classification.
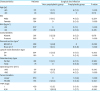
Table 2 shows the short-term surgical outcomes in the matched group. There was no significant increase in the postoperative morbidity in the non-prophylactic group compared with the prophylactic group (18.5% vs. 15.4%, P=0.640), and there were no ≥grade 3 complications (1.4% vs. 0%, respectively; P=1.000). The SSI rates in the non-prophylactic and prophylactic groups were 3.1% and 1.5%, respectively (P=0.559). Based on the CDC classification of SSI, there were 2 superficial incisional infections in the non-prophylactic group and one organ/space infection in the prophylactic group. The time to gas passage, diet initiation, and mean hospital stay were not significantly different between the two groups. However, the incidence of postoperative fever was significantly higher (27.7% vs. 12.3%, P=0.028) in the non-prophylactic group.
Table 2
Short-term surgical outcomes in the propensity score-matched sample
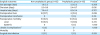
Table 3 shows the SSI rates in the non-prophylactic and prophylactic groups by subgroups, according to various clinicopathological factors. The SSI rates did not significantly increase in the non-prophylactic group in the different subgroups by age, sex, BMI, comorbidities, operative techniques, and pathological stage.
Table 3
Subgroup analysis of surgical site infections in the 2 groups
DISCUSSION
Antibiotic prophylaxis is one of the most effective tools in preventing SSIs in patients undergoing surgery; however, the widespread use of antibiotics is believed to be associated with an emerging antibiotic resistance [22]. Recently, the routine use of prophylactic antibiotics has become questionable in some abdominal procedures, such as laparoscopic cholecystectomy, due to the lower SSI rates after laparoscopic surgery [23]. In our study, we have demonstrated that postoperative morbidity, including SSI rate, did not significantly increase in patients who did not use prophylactic antibiotics after TLDG for gastric carcinoma. Despite the inherent bias of this study due to its retrospective nature, our results suggest that TLDG may be safely performed in selected patients without prophylactic antibiotic use.
The current guidelines on antimicrobial prophylaxis recommend the routine use of prophylactic antibiotics for major abdominal surgeries [11]. However, most evidence supporting the efficacy of prophylactic antibiotics in the guidelines is obtained from old studies that were performed decades ago. Additionally, the evidence for gastric cancer surgery is extremely limited, focusing only on open surgery [1213]. With the significant advances in the operating environment, such as the use of aseptic surgical techniques, use of disposable devices, and minimally invasive surgery, the incidence of SSIs after gastric cancer surgery has gradually decreased over the past decades [141516]. More importantly, the efficacy of prophylactic antibiotic use has never been investigated in the field of laparoscopic gastrectomy. Recently, a large body of evidence suggests that low-risk patients undergoing laparoscopic cholecystectomy do not require prophylactic antibiotics to prevent SSIs [23]. Therefore, future studies should be directed to guiding the optimal use of prophylactic antibiotics depending on the operative approach and patient's condition.
The indiscriminate use of prophylactic antibiotics is a challenging problem in our surgical society [24]. Although the current evidence recommends a single intraoperative use of prophylactic antibiotics for gastric cancer surgery [89], many gastric surgeons are still prescribing antibiotics to be used for up to 1–3 postoperative days due to the concerns related to the use of drains and extended lymph node dissection [25]. A recent Korean nationwide survey showed that only 19% of gastric surgeons adhered to the guidelines for intraoperative use of prophylactic antibiotics during gastric cancer surgery [26]. The proper use of prophylactic antibiotics, according to the standard guidelines, will be the first resort to reduce antibiotic use in patients undergoing surgery. The efforts to reduce antibiotic use by conforming to the standard guidelines are of great importance considering the imminent threat of antibiotic resistance.
Although antibiotics are the most effective tool to prevent SSIs in patients undergoing surgery, the importance of non-pharmacological prevention measures should also be emphasized [27]. Strict compliance with basic precautionary measures, such as the use of aseptic surgical techniques, surgical site preparation, and hand scrubbing, is essential in preventing SSIs. Previous studies have suggested that proper preoperative nutrition support for malnourished patients [28], maintenance of intraoperative normothermia [29], and improvement of tissue oxygenation by high perioperative oxygen supplementation [30] can contribute to reducing the incidence of SSIs in patients undergoing surgery. In our study, we strictly applied these strategies in all patients undergoing gastric cancer surgery.
In this study, the incidence of postoperative fever was significantly higher in patients who did not use prophylactic antibiotics. The exact cause of this is uncertain, but it may suggest that postoperative inflammatory reaction is more severe if prophylactic antibiotics are not used. Although the incidence of clinically apparent infectious complications did not significantly increase in patients who did not prophylactic antibiotics, this may require further investigation in future studies.
There are some limitations in this study. First, the non-prophylactic group in this study comprised selected patients who had a lower operative risk due to younger age (≤65 years), good performance status, and absence of malnutrition. The indication for not using prophylactic antibiotics during TLDG should be confined to this low-risk patient group. Second, the sample size of this study was relatively small to detect a small difference in the SSI rates with adequate power. Although no statistically significant difference was found, the SSI rate in the non-prophylactic group was slightly higher (2.8% vs. 1.5%) in this study. Therefore, a large multi-institutional study or randomized controlled trial will be required to further investigate the feasibility of undergoing TLDG without prophylactic antibiotic use.
Therefore, despite the limitations of a small sample size and retrospective design, this study showed that the risk of SSIs did not significantly increase in patients undergoing TLDG for gastric carcinoma who did not use prophylactic antibiotics. Prophylactic antibiotics may not be necessary for patients undergoing TLDG for early gastric carcinoma. Finally, a large randomized controlled trial is warranted to reappraise the role of prophylactic antibiotics in low-risk patients undergoing TLDG for gastric carcinoma.
 XML Download
XML Download