

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Robot-assisted gastrectomy to treat gastric cancer, first described in 2002 [1], is increasingly performed in Asian and Western countries. This method has overcome the limited maneuverability of conventional laparoscopic surgery and increases the accuracy of instrumental movements by filtering out tremors and wrist motions [2]. Moreover, robotic surgery provides better exposure and a wider operative field by 3-dimensional visualization, which is helpful for suturing and anastomosis. Totally robotic gastrectomy with intracorporeal robot-sewn anastomosis has been shown to provide satisfactory outcomes [34]. The benefits of totally minimal surgical procedure, including satisfactory cosmetic outcomes, reduced invasiveness, and safe anastomosis [56], have resulted in the gradual progression of robotic gastrectomy procedures from an assisted to a totally robotic approach. Moreover, alimentary tract restoration can be performed intracorporeally, maximizing the benefits of minimally invasive surgery.
Billroth I anastomosis is the most popular method of restoring the alimentary tract after conventional distal gastrectomy. It is the only anastomotic method that maintains physiological food passage. Moreover, this method allows the performance of gastroduodenoscopy, including endoscopic retrograde cholangiopancreatography, to check and treat duodenal and biliary tract diseases [7]. Furthermore, Billroth I anastomosis can prevent the development of internal hernia in the absence of any defects, which occurs more frequently in patients undergoing minimally invasive surgery [8]. However, Billroth I anastomosis after robotic distal gastrectomy is a challenging procedure because of anatomical limitations, including insufficient remnant stomach and limited duodenal stump. These limitations can result in anastomotic tension, along with a high rate of anastomotic leakage, thereby requiring initial assistance with a more experienced surgeon.
To overcome the technical challenges and achieve the clinical benefits of gastroduodenostomy, efforts have been made to improve the intracorporeal Billroth I anastomotic method after totally robotic distal gastrectomy (TRDG) or totally laparoscopic distal gastrectomy (TLDG). Although delta-shaped gastroduodenostomy has become the primary procedure for Billroth I anastomosis [9], it remains a complicated technique associated with a relatively high rate of anastomotic complications [61011]. Methods are therefore required to overcome the technical requirements of intracorporeal gastroduodenostomy during TRDG.
Few studies to date have described Billroth I reconstruction during TRDG [34121314]. Linear-shaped gastroduodenostomy (LSGD), which avoids duodenal rotation and overlapping reconstruction in the anterosuperior direction, has been reported to overcome the anatomical limitations of the delta-shaped method and facilitates digestive tract reconstruction [15]. In addition to being easily learned [16], LSGD was shown to be a safe and simple procedure, with a relatively low rate of bile reflux [17]. LSGD has become a routine procedure following TRDG or TLDG in our institution. However, because the application of LSGD in robotic surgery has not been investigated, this study analyzed the feasibility of LSGD in patients undergoing TRDG by comparing the outcomes of LSGD in patients undergoing TRDG or TLDG before and after adjusting for confounding factors by propensity score matching (PSM).
MATERIALS AND METHODS
Patients
This retrospective study analyzed patients who underwent laparoscopic or robotic radical distal gastrectomy with Billroth I reconstruction performed by a single surgeon between January 2009 and December 2017 at Ajou University Hospital, South Korea. Patients who underwent extracorporeal reconstruction, delta-shaped anastomosis, hand-sewn gastroduodenostomy, and other anastomotic methods were excluded from the analysis.
LSGD surgical technique in robotic procedure
All included patients underwent TRDG or TLDG with intracorporeal reconstruction using the LSGD approach [17]. Detailed information about trocar placement is shown in Fig. 1. The major procedure started with a V-shaped liver retraction [18] and perigastric lymphadenectomy, followed by the introduction of a linear endo-stapler through the left lower assistant port, transecting the duodenum in a craniocaudal direction without 90° duodenal rotation (Fig. 2A). A small entry hole was made on the superior edge of the duodenal transection line (Fig. 2B), and a small incision was made on the greater curvature of the remnant stomach 60 mm from the resection line (Fig. 2C). The cartridge jaw of the 60-mm endoscopic linear stapler was inserted into the remnant stomach, followed by the alignment of the greater curvature of the remnant stomach and the anterosuperior side of the duodenum and firing of the stapler (Fig. 2D). The common entry hole was closed using another 60-mm endo-stapler. Although three stay sutures are usually pulled to facilitate the closure of the common entry hole during laparoscopic procedures [17], this step was replaced by instrument holding during robotic procedures (Fig. 2E and F). Titanium clips were routinely applied to the everted stapler line to prevent bleeding. The final reconstruction view is shown in Fig. 2G. The perigastric lymph node stations were numbered according to the Japanese classification of gastric carcinoma (3rd English edition) [19]. The extent of the lymphadenectomy was determined using the 2010 Japanese gastric cancer treatment guidelines (version 3) [20].

 | Fig. 2Intraoperative photography of a linear-shaped gastroduodenostomy. (A) Transection of the duodenum through the left upper assistant port in a craniocaudal direction without 90° rotation. (B) Making a small incision (red solid arrow) on the superior edge of the duodenal transection line. (C) Making a small incision on the greater curvature of the remnant stomach 60 mm (red dotted line) from the resection line. (D) Insertion of the cartridge jaw of a 60-mm endoscopic linear stapler into the remnant stomach, followed by the alignment of the greater curvature of the remnant stomach and the anterosuperior side of the duodenum. The stapler was subsequently closed and fired. (E, F) Closing of the common entry hole by the articulated linear stapler in a tangential direction to the line of the duodenal transection, a step facilitated by the pulling up and alignment of the robotic instruments. (G) Final view after reconstruction. Bleeding was prevented by using the titanium clip to reinforce the everted stapler line.
|
Endoscopic surveillance and classification of endoscopic findings
All patients underwent endoscopic surveillance during the first, third, and fifth years after surgery. All procedures were performed by 1 of the 3 endoscopists who were highly specialized in gastric cancer at the Gastric Cancer Center. The entire procedure has been standardized at our institution and has been described in detail [17]. Endoscopic findings of the remnant stomach were evaluated using the Residual food, Gastritis, Bile reflux classification [21].
CUSUM and statistical analysis
The CUSUM method is a graphic approach to detecting small shifts in an overall process that can also indirectly detect data trends [16]. The CUSUM method was plotted using the Excel plugin, QI Macros, version 2018 student for Windows (KnowWare International Inc., Denver, CO, USA).
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 24.0 for Windows (SPSS Inc., Chicago, IL, USA). PSM was performed using the SPSS-R plugin (version 3.4.3 with MatchIt package). Quantitative data were expressed as mean±standard deviation and categorical data as number (%). Continuous variables were analyzed by Student's t-test and categorical variables by the χ2 test or Fisher's exact test. The Cochran–Mantel–Haenszel test was used to calculate the odds ratios (ORs) for complications and P-values for the interaction of approach group and baseline characteristics. Univariate and multivariate analyses of associations between postoperative complications and the clinicopathological features of gastric cancer were performed using binary logistic regression models to estimate the ORs and 95% confidence intervals. Clinicopathological features analyzed as binary variables included age (≤60 or >60 years), gender, body mass index (≤25 or >25 kg/m2), comorbidity (absent or present), American Society of Anesthesiologists (ASA) classification score (1 or 2–3), previous abdominal surgery (absent or present), tumor size (≤2 or >2 cm), tumor vertical location (middle or lower third), approach method, lymph node dissection (<D2 or ≥D2), combined resection (no or yes), operation time (≤150 or >150 minutes), estimated blood loss (≤50 or >50 mL), resection distal margin (≤2 or >2 cm), pathological T classification (T1 or T2–T4), pathological N classification (positive or negative), and pStage classification (I or II–III). The level for rejection of the null hypothesis was set at a P-value <0.05.
RESULTS
Of the 1163 patients who underwent TRDG or TLDG performed by a single surgeon during the time period, 414 were considered eligible for analysis, including 275 who underwent TLDG and 139 who underwent TRDG.
Comparison between TRDG and TLDG after LSGD
The demographic characteristics of all patients and of the PSM cohort are summarized in Table 1. Analysis of the full patient cohort showed that the robotic group was significantly younger than the laparoscopic group (52.6±11.3 years vs. 60.0±13.0 years, P<0.001), that comorbidities were more frequent in the laparoscopic group (P=0.003) than the robotic group, and that the two groups differed significantly in ASA score (P=0.002). To better match their characteristics, the two groups were subjected to 1:1 PSM, followed by analysis of the matched groups. PSM resulted in groups of 107 patients each, with no significant between-group differences in patient characteristics (Table 1).
Table 1
Baseline characteristics of patients in the original and propensity score-matched cohorts
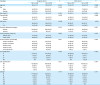
Data expressed as mean±standard deviation or number (%).
ASA = American Society of Anesthesiologists score; BMI = body mass index; RG = robotic group; LG = laparoscopic group; PSM = propensity score matching; NA = not applicable.
*Stages classified by the 7th Union for International Cancer Control/American Joint Committee on Cancer staging system.
![]()
The operative and postoperative outcomes of the two groups are compared in Table 2. Estimated operative blood loss was greater (90.3±96.0 mL vs. 72.0±73.2 mL, P=0.049) and postoperative hospital stay longer (7.5±4.7 days vs. 6.2±1.9 days, P<0.003) in the laparoscopic than that in the robotic group. However, operation time was significantly shorter in the laparoscopic group (132.1±37.8 minutes vs. 163.5±33.8 minutes, P<0.001) than that in the robotic group. Following PSM, the 2 groups no longer differed significantly in the estimated blood loss (P=0.879).
Table 2
Operative and postoperative outcomes of patients in the original and propensity score-matched cohorts after linear-shaped gastroduodenostomy

Data expressed as mean±standard deviation or number (%).
RG = robotic group; LG = laparoscopic group; PSM = propensity score matching; NA = not applicable.
*Major complications defined according to the Clavien-Dindo classification ≥III.
![]()
Endoscopic findings during the first, third, and fifth postoperative years are compared in Fig. 3. There were no significant differences in residual food, degree of gastritis, and bile reflux during the first and third years. However, during the fifth year, bile reflux was significantly better in the laparoscopic group compared to the robotic group (P=0.016; Fig. 3C).

Analysis between subgroup and of the risk factors of LSGD
The total postoperative complication of all the patients in subgroup between TRDG and TLDG was analyzed according to clinicopathological features (Fig. 4). There was no significant association between the distinctive approach and any of the variables studied.
 | Fig. 4Forest plot showing the ORs for total postoperative complications and P-values for the interaction of approach group and baseline characteristics.RG = robotic group; LG = laparoscopic group; OR = odds ratio; CI = confidence interval; BMI = body mass index; ASA = American Society of Anesthesiologists.
|
Table 3 lists the risk factors for total postoperative complications after LSGD analyzed by univariate and multivariate logistic analyses. Multivariate analysis showed that operation time more than 150 minutes was the independent risk factor (P=0.010).
Table 3
Univariate and multivariate analysis of risk factors for complication after intracorporeal gastroduodenostomy

Variables with P-values less than 0.1 on univariate analysis are considered for inclusion in the multivariate model. Univariate and multivariate data expressed as number and OR (95% CI).
OR = odds ratio; CI = confidence interval; BMI = body mass index; ASA = American Society of Anesthesiologists score
*According to the Japanese classification of gastric carcinoma: 3rd English edition; †According to the Japanese gastric cancer treatment guideline 2010; ‡Stages classified by the 8th Union for International Cancer Control/American Joint Committee on Cancer staging system.
![]()
Learning curve for LSGD in TRDG
C+ and C− are defined as the CUSUMs of the positive and negative differences, respectively, between individual and mean operation times. The upper CUSUM was defined as positive four times the standard deviation and the lower CUSUM as negative four times the standard deviation. The C+ curve fluctuated between the values of 0 and 135.49 (upper CUSUM), without a clear peak outside the upper CUSUM (Fig. 5A). The mean operation time and the moving averages of 20 patients were approximately 150 minutes (Fig. 5B). These findings indicated that there was no definitive learning curve for LSGD in TRDG.

DISCUSSION
Following robotic distal gastrectomy, the digestive tract can be reconstructed using either the intracorporeal or extracorporeal Billroth I method. Because minilaparotomy is required during the extracorporeal procedure, only intracorporeal reconstruction is minimally invasive and can maximize cosmetic benefits. Because no study to date has investigated the feasibility of LSGD in patients undergoing TRDG, this study was designed to evaluate this procedure. Patients who underwent TRDG and TLDG were subjected to 1:1 PSM, minimizing selection and the confounding effects of patients' characteristics. This study concluded that LSGD showed comparable operative and postoperative outcomes and endoscopic findings in patients who underwent TRDG and TLDG. Multivariate analysis revealed that the operation time was the only independent risk factor associated with postoperative complications for LSGD. We also found no learning curve for LSGD use in TRDG; rather, mastering the LSGD technique in TLDG was sufficient.
The present study also showed that operation time was significantly longer for TRDG than for TLDG, a finding associated with the inherent characteristics of robotic surgery. Additional time was required for docking, including the assembly of the manipulator arms and debugging the equipment, procedures that are both time-consuming and inherent to the robotic system [22]. Docking time has been estimated at approximately 30 minutes [2324], prolonging the operation time in TRDG. Moreover, prolonged operation time is the independent risk factor for LSGD; this is consistent with other reports [2526]. The increased operative duration could increase the opportunities for violations in sterile technique and the risks of coagulation, blood stasis, and surgical bleeding, indicating a more complex surgical procedure. Nevertheless, we should not sacrifice patient safety to hasten the surgical procedure. However, surgeons can positively impact patient outcomes with simple and practical improvements to reduce the operation time.
Although LSGD in TRDG is a more time-consuming procedure compared to that in TLDG, it is a horizontally comparable method compared to others. A retrospective cohort study assessing the feasibility of delta-shaped Billroth I anastomosis in TLDG found that the median total operation time was 346 minutes and the median hospital stay was 11 days [13], with both being considerably longer than in the present study. Moreover, a study of the feasibility and safety of intracorporeal robotic hand-sewn Billroth I anastomosis in TRDG found that the mean total operation time was 266.54±35.26 min, the mean estimated blood loss was 80.78±32.37 mL, and the mean hospital stay was 6.2±2.5 days [3]. The LSGD technique showed non-inferior surgical outcomes compared to the hand-sewn method in TRDG.
Robotic surgery can be performed safely with acceptable surgical outcomes by experts in open gastrectomy, with the learning curve for robotic gastrectomy being significantly overcome by a sufficient experience with laparoscopic gastrectomy [272829]. The shorter hospitalization time observed in patients who underwent TRDG may be due to the performance of a surgeon with extensive laparoscopic experience, including stable and proficient dissection techniques. Moreover, the 5-year rates of residual food, remnant gastritis, and bile reflux were generally similar in the TRDG and TLDG groups. Although the incidence of bile reflux was significantly lower in the laparoscopic than in the robotic group at 5 years, the difference may have been due to the small sample size at this follow-up time.
The present study had several limitations. First, this was a single institute, nonrandomized, retrospective cohort study, although the data were extracted prospectively. Second, all procedures were performed by a single surgeon with team members being relatively stable. Thus, there may have been some deviations in identifying the non-inferiority of LSGD in TRDG compared to TLDG. Third, to obtain the parallel alignment between the duodenal stump and the remnant stomach, the left lower trocar placement for assistant should be placed higher compared to that of conventional robotic procedure. This might cause the clashing between the assistant and robotic arms, leading to the assistant's difficulty in handling the laparoscopic instruments via the left lower trocar. Additionally, although this technique was performed during robotic distal gastrectomy, the reconstruction was not performed using robotic instruments but laparoscopic staplers. Hence, this technique still depends on the assistant's skill. Finally, despite the present study providing valuable information about LSGD in TRDG, the optimal method for Billroth I anastomosis in TRDG remains to be determined. Therefore, further prospective, multicenter studies are required.
In conclusion, LSGD was a feasible and easy-to-perform procedure in TRDG, with comparable short-term and long-term outcomes as in TLDG. LSGD may be a good option for intracorporeal Billroth I anastomosis in TRDG.
 XML Download
XML Download