

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Staphylococcus aureus is a common pathogen of skin and soft tissue infection (SSTI) and bone and joint infection in children and also one of the most common organisms in hospital-acquired infections.1 History of recent hospitalization, recent surgery, older age, and possession of central catheter are known as major risk factors associated with S. aureus bacteremia.2 Thus, empiric antibiotic therapy of these clinical syndromes should consider risk factors and should be based on local antibiotic susceptibility patterns.
In many countries, community acquired-methicillin resistant S. aureus (CA-MRSA) has shown an increase in prevalence since the early 2000s.3 A number of studies from the US suggested that this lead not only to an increase in antibiotic resistance, but also an actual increase in the incidence of SSTI and hospitalization due to methicillin resistant S. aureus (MRSA) in children.456 The increase in MRSA infection was reported to be attributed by the increase in the clone USA300, otherwise classified as multilocus sequence type (ST), ST8-SCCmec IV which almost always has the Panton-Valentine leukocidin (PVL) toxin.7
The increase in virulence and spread of CA-MRSA strains contributes largely to the presence of PVL, a cytotoxin which leads to formation of pores and causes neutrophil lysis and cell death.8 PVL strains have been reported to be more strongly associated with SSTIs than other forms of invasive diseases, such as pneumonia, musculoskeletal diseases, and bacteremia.9
Major CA-MRSA clones have been reported worldwide including ST1 in Asia, Europe, US, ST8 in Europe and US and ST30 in Australia, Europe and South America.1011 PVL-positive ST30-SCCmec IV has been reported as an important CA-MRSA in Singapore, Japan and Latin America.12 Although the first report of PVL-positive-ST30 MRSA infection was reported in 2013,13 reports of the distribution of strains in Korean children are limited. The molecular distribution of strains is important as they are closely related with changes in the antibiotic susceptibility and also changes in clinical epidemiology such as incidence of SSTI.14
Therefore, in this study, we investigated the antimicrobial resistance and molecular characteristics of S. aureus among children in Korea in two important clinical entities, SSTI and bone and joint infection which are common forms of S. aureus infections.
METHODS
Study design
S. aureus previously isolated from children under 18 years of age diagnosed with SSTI and bone and joint infection at Seoul National University Bundang Hospital from August 2010 to November 2016 were included in the analysis. Demographic information of the patients and details of their underlying diseases and clinical diagnoses were collected from medical records. Electronic medical records were reviewed for clinical data and antibiotic susceptibility results. Cases were classified as health care-associated community-onset (HACO) infections when culture was obtained ≤ 3 days after admission and/or prior year hospitalization, surgery, or central vascular catheter presence ≤ 2 days before culture. Hospital-onset (HO) infections were designated when culture was obtained > 3 days after admission, and cases were defined as community-acquired (CA) infections if no other criteria were met.
Bacterial isolation, identification and antimicrobial susceptibility tests
Isolates from children with SSTI and bone and joint infection due to S. aureus were collected during the study period and stored at −80°C until analysis. Isolates related to outbreaks were excluded. Isolation of S. aureus and antimicrobial susceptibility tests were performed in the clinical microbiology laboratory using an automatic system (MicroScan Walk-Away; Siemens Healthcare Diagnostics, Deerfield, MA, USA). Antimicrobial susceptibility testing data of 9 antimicrobial agents were obtained: oxacillin, penicillin, gentamicin, ciprofloxacin, clindamycin, erythromycin, rifampicin, trimethoprim/sulfamethoxazole, and vancomycin. Confirmatory tests for MRSA isolates were done by mecA gene polymerase chain reaction (PCR) during SCCmec typing.15 Resistance to antibiotics for each isolate was defined according to the Clinical and Laboratory Standards Institute guidelines published in 2019.
Multiplex PCR assays for MRSA and molecular typing
Multilocus sequence typing (MLST) was done by PCR amplification and sequencing of seven housekeeping genes (arcC, aroE, glpF, gmk, pta, tpi, yqiL) using the primer pairs as described previously.16 Each sequence was submitted to the MLST database website (https://pubmlst.org/) for assignment of an allelic profile and ST. The molecular features of the MRSA strains were analyzed by SCCmec typing and subtyping.15 PCR was done for the PVL gene,17 qac A/B,18 smr,19 and mupA20 genes.
RESULTS
Patient characteristics
A total of 67 S. aureus clones isolated from SSTI (41/67, 61.2%) and bone and joint infection (26/67, 38.8%) were included in the study. The median age of the subjects was 18 months (range 3 days–18 years). Male subjects accounted for 50.7% (34/67). There were 15 children (22.4%) with underlying diseases and recent use of hospital care, including prematurity (n = 3), post-operation infection (n = 5), neurologic disease (n = 2), malignancy (n = 2) and others (n = 3).
Antibiotic resistant rate
Among the 67 isolates from children with SSTI or bone and joint infection, 20 (29.9%) were MRSA (Table 1). According to diagnosis, MRSA rate was 34.1% (14/41) in SSTI and 23.1% (6/26) in children with bone and joint infection. Among all isolates, 74.6% (50/67) were CA, 16.4% (11/67) were HACO infections and 9.0% (6/67) were HO infections. Among MRSA isolates, 70% (14/20) were CA, 20% (4/20) were HACO and 10.0% were HO infections (Table 1). Regardless of SSTI or bone and joint infection, 53.3% (8/15) of the children with underlying disease were MRSA. After excluding these cases, among children < 1 month of age, 100.0% (5/5) were MRSA whereas in children ≥ 1 months of age, 15.4% (4/26) of SSTI, and 14.3% (3/21) of bone and joint infection were MRSA.
Table 1
Methicillin-resistant Staphylococcus aureus rate according to clinical diagnosis

Data are presented as number (%).
SSTI = skin and soft tissue infection, BJI = bone and joint infection, MSSA = methicillin-susceptible Staphylococcus aureus, MRSA = methicillin-resistant S. aureus.
![]()
As for other antibiotics, the resistant rate among all strains was 9.0% (6/67) for clindamycin, 4.5% (3/67) for ciprofloxacin, 52.2% (35/67) for erythromycin and none of the isolates had resistance against trimethoprim/sulfamethoxazole (Table 2). Among the 20 MRSA strains, 15.0% (3/20) were resistant to clindamycin, and 20.0% (4/20) were clindamycin susceptible and also erythromycin resistant suggesting inducible clindamycin resistance.
Table 2
Antibiotic resistance rate according to clinical diagnosis
Data are presented as number (%). Among MRSA strains (n = 20): clindamycin-R (n = 3, 15%), TMP/SMX-R (n = 0, 0%), clindamycin-R/erythromycin-R (n = 3, 15%), clindamycin-S/erythromycin-R (n = 4, 20%).
SSTI = skin and soft tissue infection, BJI = bone and joint infection, TMP/SMX = trimethoprim/sulfamethoxazole, MRSA = methicillin resistant Staphylococcus aureus.
![]()
Molecular analysis
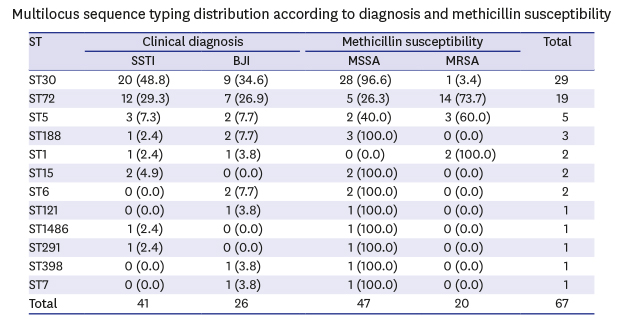
Among all isolates, ST30 was the most common clone among SSTI and bone and joint infection, followed by ST72 and ST5 (Table 3). Among methicillin-susceptible Staphylococcus aureus (MSSA) strains, ST30 (28/47, 59.6%) was the predominant clone and among all ST30, 96.6% (28/29) were MSSA. MRSA strains included ST72-SCCmec IV (14/20, 70.0%), ST5-SCCmec II (3/20, 15.0%), ST1-SCCmec IV (2/20, 10.0%) and ST30-SCCmec IV (1/20, 5.0%). PVL was detected in 3 strains which were all ST30 (3.8%, ST30-SCCmec IV N=1, MSSA ST30 n = 2). qac A/B was detected in 3 strains (MRSA = 3), smr in 3 strains (MSSA = 1, MRSA = 2) and mupA in 7 strains (MSSA = 2, MRSA = 5).
Table 3
Multilocus sequence typing distribution according to diagnosis and methicillin susceptibility
Data are presented as number (%).
ST = sequence type, SSTI = skin and soft tissue infection, BJI = bone and joint infection, MSSA = methicillin-susceptible Staphylococcus aureus, MRSA = methicillin-resistant S. aureus.
![]()
DISCUSSION
In this study, we analyzed the antibiotic resistant rate and molecular epidemiology of SSTI and bone and joint infection due to S. aureus among children in Korea. MRSA accounted for 34.1% in SSTI and 23.1% in bone and joint infection in children. When excluding children with underlying diseases, all cases in children under 1 month of age were MRSA and among children 1 month and older, 15.4% in SSTI and 14.3% in bone and joint infection were found to be MRSA. Although there is no definite cutoff as to what percentage of CA-MRSA should include coverage of MRSA for empirical antibiotics, neonates and children with underlying diseases may need coverage for MRSA in SSTI or bone and joint infection pending microbiologic culture results. Children over 1 month of age with no underlying diseases need judicious antibiotic choice based on the clinical manifestations, age, other risk factors and antibiotic resistant rates.
The MRSA rate of 23.1% in this study might suggest an increase in MRSA on bone and joint infection in children, compared to a previous report in Korea during 2003–2009, which showed that among cases due to S. aureus, 12.7% were MRSA.21 In this study, 70% (14/20) of the MRSA strains were CA which may suggest an increase of MRSA in the community. Increase in MRSA has been seen recently in many countries. In studies done at a large children's hospital in the US, by 2004, more than 70% of all CA S. aureus (CA-S) infections, almost 60% of invasive CA-S infections were MRSA, of which > 90% were USA300.2223 However, interestingly, recent reports showed that the CA-MRSA rate is decreasing again. Compared with 2007, invasive CA-MRSA infections decreased from 61.0% to 33.8% in 2014.24 Such changes in epidemiology emphasize the importance of continuous monitoring on antibiotic resistance rates in the community.
Clindamycin and trimethoprim/sulfamethoxazole are feasible options for treatment in SSTI or in limited cases of bone and joint infection. Clindamycin may be considered for empirical treatment in children with SSTI or bone and joint infection when clindamycin resistance rate is < 10%.25 Thus, considering the overall resistant rate for clindamycin in this study of 9.0%, clindamycin may be an option in empirical treatment in Korean children. The clindamycin resistance rate is higher compared with a previous study of children with MRSA nasal carriage, where clindamycin resistance was 2.5%.26 Direct comparison between the studies is difficult, however continuous monitoring on clindamycin resistance is warranted. Trimethoprim/sulfamethoxazole also showed to be comparable in a randomized controlled trial to clindamycin in uncomplicated SSTIs.27 None of the strains in this study was resistant to trimethroprim/sulfamethoxazole.
Among children with SSTI and bone and joint infection, ST30 was the most common type and the majority was MSSA (96.6%). PVL toxin was found in 3 strains (4.8%) which were all ST30 and among them, one strain was MRSA. Among MRSA isolates in this study, ST72-SCCmec type IV was most common. These results coincide with previous reports in Korea where ST72-SCCmec type IV strains have been reported as the most prevalent molecular type in CA-MRSA.2829 A study among adults reported ST72-SCCmec type IV the most prevalent strain in 2005 and another study in children during 2006–2010 with MRSA infection showed ST72-SCCmec type IV to be most common.29 In that study, 10% (4/40) of the CA-MRSA strains were PVL positive, including three strains ST8-SCCmec type IV-related (2 ST and 1 isolate ST931, a SLV of ST8) and 1 ST30-SCCmec type IV. Overall, the molecular distribution of CA-MRSA in Korea does not seem to have changed greatly since 2005.
In this study, qac A/B, smr and mupA genes were included in the analysis. qac A/B and smr genes encode multidrug efflux pumps which are associated with higher minimum bactericidal concentrations of chlorhexidine and various antiseptics used in hospital settings.19 mupA gene is known to be related with mupirocin resistance,20 a widely used topical antimicrobial agent used for skin infections due to gram-positive pathogens, including S. aureus. This majority of isolates were community-associated, and qac A/B, smr and mupA genes were detected in a limited number of isolates in this study. A need for further wide-scale studies on healthcare-associated infections is essential.
Data in this report may not be applied to other regions in the country, as strains were obtained from subjects of a single tertiary hospital. Park et al.30 reported the molecular characteristics of CA-MRSA from children with skin infections in Busan, Korea. Among S. aureus isolates, 40.6% (28/69) were MRSA and among 28 CA-MRSA isolates, two major clones were identified as staphylocoagulase (SC) type Vb ST72 SCCmecIV and SC type 1 ST89 SCCmecII variant. The results of these studies will give us a glimpse into the antibiotic resistance and molecular epidemiology of S. aureus isolated from SSTI and bone and joint infection in children in Korea.
Although many CA-MRSA strains have been reported to be disseminating worldwide, ST72 has not been widely reported. Interestingly, ST72 does not contain the PVL gene and Chen et al.31 reported that the whole genome analysis of PVL-negative ST72 showed no additional virulence determinants, such as other leukotoxins, to substitute the absence of PVL. This finding suggests that the virulence of such strain may be dependent on the gene regulatory adaptations that enhance the expression of core-encoded virulence determinants, rather than the acquisition of other virulence factors such as PVL.31
Among CA-MRSA strains, ST30 has been reported to be a dominant strain in many countries.323334 However, although ST30 was the most prevalent in this study, the majority of the strains were MSSA. Continuous monitoring on the molecular distribution and antimicrobial resistance patterns of this strain in Korea might be warranted. In conclusion, S. aureus is a major pathogen in SSTI and bone and joint infection in children. In children ≥ 1 month with no underlying diseases, MRSA accounted for approximately 15% in SSTI and bone and joint infection; whereas, MRSA was the dominant strain in children < 1 month of age. Among children with SSTI and bone and joint infection, ST30 was the predominant strain, and the majority was MSSA. Among MRSA isolates, ST72-SCCmec type IV was the most common in SSTI and bone and joint infection. No strains of the USA300 trait were found in this study, and PVL toxin was found in limited cases. The antibiotic resistance rate and molecular epidemiology among staphylococcal infections in Korean children should be monitored continuously for guidance on appropriate empirical antibiotics.
 XML Download
XML Download