

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Despite continuing efforts on the part of hospitals to improve the quality of care, mistakes that occur during the administration of intravenous (IV) medications remain the most common type of hospital error.1 These errors reflect the complexity of delivering IV medications via infusion and syringe pumps, as this multistep process provides numerous opportunities for error, especially related to the IV pump.2 From 2005 through 2009, the U.S. Food and Drug Administration received about 56,000 reports of adverse events associated with the use of infusion pumps, many of which led to injury and death.3 Because high-risk medications tend to be administered via IV pumps to seriously ill patients, IV-pump-related errors are more likely to lead to harm, and the severity of that harm is greater.
Generally, a syringe pump is preferentially used in the operating room due to its small size, precise control of the infused volume, enhanced mobility, and zero risk of free flow.4 However, as the limited syringe capacity requires frequent changeovers to ensure a continuous supply of the medication, syringe pumps are usually replaced by infusion pumps following the arrival of the surgical patient in the intensive care unit (ICU). This relay process may transiently interrupt drug administration and cause medication errors, especially when multiple IV pumps are in use. Difficulties in maintaining hemodynamics during and after the changeover in patients receiving vasoactive drugs are also likely.56
A Korean company developed and commercialized a new infusion device (Anyfusion®) which combines a syringe and an infusion pump into a single pump unit for the first time in the world. This dual-function unit has a lower purchase price and maintenance costs and requires less space than the separate syringe and infusion pumps. We hypothesized that the changeover performed using the Anyfusion® is also less time-consuming and easier for the operator, thereby reducing the potential for errors. We therefore conducted a simulation study to compare the clinical workload of operators using the Anyfusion® pump and using the conventional method consisting of two infusion devices, a syringe pump and an infusion pump.
METHODS
This was a prospective, randomized, crossover-designed simulation study using an imitation arm with an IV line. Written informed consent for study participation was obtained from 22 recovery room or anesthesia nurses. In Korea, only physicians are legally allowed to administer anesthesia; thus, the anesthesia nurse's role is limited to supporting and assisting anesthesiologists throughout the perioperative period. The study protocol was registered at the Clinical Research Information Service (CRIS: https://cris.nih.go.kr/cris/en/; ref: KCT0004172).
Each participant performed two consecutive infusion mode changes: the conventional method using two infusion devices (a syringe pump and an infusion pump) and the new method using the single infusion device (Anyfusion®). The order in which each changeover techniques was used was assigned randomly according to a computer-generated randomization table of sequences. Allocation was concealed by the use of sealed envelopes and was not made known until the actual start of the experiment.
Infusion devices
The Anyfusion H-100 (MEINNTECH, Anyang, Korea) is a newly developed and recently commercialized infusion device that combines an infusion pump and a syringe pump into a single-unit pump. Its core technology is based on the capacity of a disposable cylinder cartilage in which the parallel motion of a syringe is converted to a rotary motion by two internal pistons (Fig. 1). Detailed information is available at https://www.youtube.com/watch?v=Kp_4AUb36d8.
 | Fig. 1Core technology of Anyfusion®. Its disposable cylinder cartilage converts the parallel motion of a syringe to a rotary motion using two internal pistons. The first piston rotates inside the cylinder cartilage and draws in the medication. The second piston then rotates and pushes out the medication.
|
The infusion devices used in the conventional method were the Medfusion 3500 syringe pump (Smith Medical, Kent, UK) and the Terufusion volumetric infusion pump (TE-135; TERUMO, Tokyo, Japan).
Before the study, all participants received a 2-hour practical demonstration of the relevant devices and their operation, followed by a 4-week training course that included practical work.
Procedures
A simulated patient room was set up in which an imitation arm with an IV line was placed on a bed and an IV pole equipped with the infusion device next to the bed. To limit the comparison to the workload during a changeover, a 50-mL syringe and a 250-mL bottle with premixed medication were prepared.
In the conventional method, the nurses were asked to administer the IV medication to the simulated patient by connecting new IV tubing into the injection port of a 3-way stopcock and then to start the syringe pump at a delivery rate of 6 mL/hr (phase 1). They were then asked to stop the syringe pump and administer the medication by connecting new IV tubing and a bottle to an injection port and start the infusion pump at 60 mL/hr (phase 2) (Fig. 2A).
 | Fig. 2Simulated change from a syringe pump to an infusion pump in the delivery of a continuous intravenous infusion. (A) Conventional changeover method using two infusion devices (a syringe pump and an infusion pump), (B) Changeover using the Anyfusion® method.
|
After a brief break, the nurses were asked to perform the same task using the Anyfusion® (Fig. 2B). This involved connecting a syringe and a bottle to the disposable line of the Anyfusion® via a 3-way stopcock. After self-priming of the IV components to remove air bubbles, the syringe pump was started at a delivery rate of 6 mL/hr by turning the 3-way stopcock to the respective infusion setting. A change in the administration mode was accomplished by pressing a button to set the new infusion rate (60 mL/hr) and turning the 3-way stopcock to deliver the new infusion (Fig. 2B).
The nurses were instructed to perform all of these operations at the same speed used during actual work. Each procedure was judged as complete when a drop of the medication appeared at the end of the IV line, at which point, the timer was stopped. Changing the infusion rate during the changeover of the infusion mode was conducted to reflect our hospital's policy of administering two different vasopressin concentrations, which are delivered by the two different pump types, in the operating room and ICU: via a syringe pump at a concentration of 1 IU/mL and via an infusion pump at a concentration of 0.1 IU/mL, respectively.
Outcomes
All evaluations and data recording were performed by the same two anesthesiologists; one evaluated the time-related variables, and the other monitored the number of button clicks. For the conventional method, the total execution time, the phase 1 and 2 execution times (i.e., the time spent during the syringe pump-related procedure and during the infusion pump-related procedure), and the total number of clicks were recorded. For the Anyfusion® method, the total execution time and total number of button clicks were recorded. The nurses were instructed to perform the both tasks with the minimum number of button clicks necessary for each changeover techniques (e.g., buttons for basic pump functionalities such as power on, start/stop, administration rate, volume to be infused, or purge). All of the relevant devices are operated only by pressing the buttons because of no implementation of operating knobs, handles, or dials. A task attempt lasting > 5 minutes was defined as a failed procedure.
After the completion of both methods, the nurses were asked to subjectively rate the difficulty of the tasks associated with each method using a numerical rating scale with a score from 0 (extremely easy) to 10 (extremely difficult).
Statistical analysis
The primary outcome was the total execution time, defined as the time from the setup with the syringe pump or Anyfusion® to the delivery of the medication via the changed infusion pump mode. In a pilot study, the total execution time of the conventional method was 87.7 ± 23.2 seconds. An a priori power analysis indicated that a sample size of 10 participants in each group was sufficient to detect a clinically relevant 20% difference in the total execution time between the conventional and Anyfusion® methods, with a type I error of 0.05 and power of 90%. To compensate for a possible dropout rate of 10%, 11 participants were enrolled in each group.
To control for a carryover effect (i.e., the effect of being tested in one condition on the participant's behavior in later conditions), the total execution time required for the two methods was compared across the two sequence groups using a t-test.7 Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed variables were analyzed using a paired t-test, and non-normally distributed continuous variables using a Wilcoxon signed rank test. A Spearman correlation test was used to evaluate the relationships between operator experience (overall experience as a nurse and specific experience as a as a post-anesthesia care unit [PACU], anesthesia, or ICU nurse) and task performance.
SPSS v20.0 (IBM SPSS Statistics, New York, NY, USA) was used in all statistical analyses. Statistical significance was defined as a P value < 0.05.
RESULTS
Twenty-two participants performed the two interventions according to the allocated sequence. Neither group had a failed task. They had a broad range of clinical experience levels as a nurse with 36.0–216.0 months (mean ± standard deviation [SD], 118.2 ± 55.0) and specific experience as a PACU, anesthesia, or ICU nurse with 36.0–204.0 months (mean ± SD, 108.0 ± 51.9) (Table 1). The overall and specific experience levels were not significantly correlated with the total execution times and total number of clicks of the two methods (P > 0.05) (Table 2).
Table 1
Comparison of the clinical experiences of the operators in the sequence-related performance of the two tasks

Values are expressed as the median (interquartile range).
PACU = post-anesthesia care unit, ICU = intensive care unit.
![]()
Table 2
Relationship between operator experience (overall experience as a nurse and specific experience as a post-anesthesia care unit, anesthesia, or intensive care unit nurse) and task performance

![]()
The differential carryover effect of a preceding task on the subsequent task was statistically insignificant (P = 0.272, 0.306, and 0.931 for the total execution time, total click number, and difficulty score, respectively).
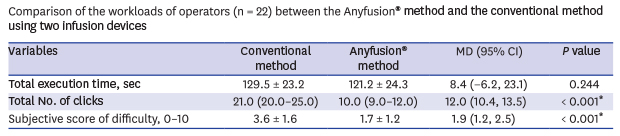
The total execution time did not differ between the two groups (129.5 ± 23.2 seconds in the conventional method group vs. 121.2 ± 24.3 seconds in the Anyfusion® group; P = 0.244). However, in terms of the total number of button clicks, significantly fewer clicks were needed for the Anyfusion® method than for the conventional method (median [interquartile range], 10.0 [9.0–12.0] vs. 21.0 [20.0–25.0], respectively; mean difference, 12.0; 95% confidence interval [CI], 10.4–13.5; P < 0.001) (Table 3). For the conventional method, the time spent during phases 1 and 2 was 59.5 ± 14.7 seconds and 70.0 ± 14.9 seconds, respectively.
Table 3
Comparison of the workloads of operators (n = 22) between the Anyfusion® method and the conventional method using two infusion devices

Values are expressed as the mean ± standard deviation or median (interquartile range).
Subjectively perceived difficulty was measured using a numerical rating scale ranging from 0 (extremely easy) to 10 (extremely difficult).
MD = mean difference, CI = confidence interval.
*Statistically significant at P < 0.05.
![]()
The subjective difficulty scores for the conventional and Anyfusion® methods were 3.6 ± 1.6 and 1.7 ± 1.2, respectively. Thus, the new method was rated as easier than the conventional method (mean difference, 1.9; 95% CI, 1.2–2.5; P < 0.001) (Table 3).
DISCUSSION
This study showed that the changeover associated with the Anyfusion® pump required significantly fewer button clicks than that required for the conventional method, although the total execution times of the two methods were similar. In rating the ease of use, operators rated the Anyfusion® method as easier than the conventional method.
Although syringe pumps are preferentially used in the operating room, their sustained use in the ICU requires frequent syringe substitutions due to the limited syringe capacity. These changeovers can increase the nursing staff's workload and may lead to human errors, including those resulting in adverse incidents.68 Thus, when the patient is transferred to the ICU, the syringe pump is generally replaced by an infusion pump. However, this relay process inevitably results in a transient interruption of drug administration and increases the risk of medication errors. A previous ICU study from the UK showed that > 35% of adverse effects on patient blood pressure occurred during epinephrine or norepinephrine infusion pump changeovers.8 As vital or potent drugs are mostly delivered to seriously ill patients via infusion devices, even minor adverse events during a relay process can have significant consequences in terms of patient safety.56 Furthermore, in the busy and stressful setting of the ICU, there is a high risk of medication errors, even for highly experienced clinicians.9
We hypothesized that, as a single infusion device with a dual function (syringe and infusion pump modes), the Anyfusion® could significantly reduce operator workload during the changeover process. If the concentration of the IV infusion medication has been standardized and the syringe containing the pre-mixed drug is already connected to the device, then a mode change would be possible in the Anyfusion® simply by turning the 3-way stopcock to the new infusion setting, without the need to press any buttons.
However, in the present study, the Anyfusion® method did not significantly reduce the total execution time compared to the conventional method. Despite the inherently simple task involved in a mode change, the initial setup process for the dual-mode device and the process of removing air bubbles (priming of the tubing set) were identified as the major time-consuming processes associated with the Anyfusion®. Whereas in the conventional method, air bubble elimination is achieved by free running prior to installation, the Anyfusion® has an automatic air-removal process initiated via a purge button. Because the Anyfusion® delivers the medications by a suction process involving piston pumps in a cylinder cartilage, this mechanical shortcoming may be difficult to overcome. The incorporation of fine-bore lines with a small priming volume into disposable accessory tubing may offer a solution. However, it should be noted that the initial setup process for the Anyfusion® is a preparatory measure performed under less stressful conditions and is not part of the therapeutic process. Thus, air bubble elimination might not increase the perceived workload of practitioners significantly. By contrast, the pump change (phase 2) in the conventional method is generally performed under time pressure and stressful conditions, and in our study, it required 70.0 ± 14.9 seconds.
Use of the Anyfusion® reduced the number of button clicks by almost half compared to the conventional method. A consistent finding in all medical-device-related accident research is that the main cause of adverse incidents is user error.10 Similarly, most adverse drug events associated with IV infusion device error result from nurses manually inputting incorrect settings into the pump.1112 Thus, the use of fewer button clicks can be expected to reduce medication errors by reducing the number of “slip-of-the-finger” errors during the manipulation of multiple infusion devices.
Collectively, operators rated the Anyfusion® method as easier than the conventional method (mean difference in subjective difficulty score [1–10], 1.9; 95% CI, 1.2–2.5; P < 0.001). Because changeovers of infusion devices are mostly performed under time pressure and in stressful situations, this finding may be especially important. In addition to the physical workload, the cognitive workload and time pressure are major sources of job stress among ICU nurses, which may ultimately have negative consequences for the patients they care for.1314 The implementation of a strategy to reduce unnecessary complexity and eliminate performance obstacles in clinical practice can be expected to improve patient safety.1015
For the clinical use of a new infusion device, its safety and efficacy must be proven in accordance with the requirements of the international standard International Electrotechnical Commission (IEC) 60601-2-24.16 Anyfusion® satisfied all of the items of the IEC 60601-2-24. In the infusion performance evaluation, Anyfusion® satisfied the criterion of ± 2.0% at flow rates of 0.1, 5.0, and 25.0 mL/hr. Notably, the merits of Anyfusion® are due to its technology, which enables a syringe pump and an infusion pump to be combined into a single unit. Besides its ease of use, occupies less space and is potentially less expensive than two separate infusion devices. Moreover, its single-interface strategy simplifies staff training, reduces programming complexity, and improves communication among practitioners, leading to a potentially significant reduction in infusion-related medication errors and subsequent patient harm.17
Our study has several potential limitations. First, only one brand of each infusion device used in the conventional changeover method was evaluated, which might limit the generalizability of the results. These devices were chosen because of their current use in our hospital and their reputation for good usability. However, other brands of pumps may result in different workload profiles.
Second, while the participating nurses had prior experience with the infusion devices used in the conventional method, they lacked experience using the Anyfusion®. To minimize this imbalance, we provided sufficient training in the three devices (a 2-hour practical demonstration of the operation of the relevant devices, followed by a 4-week training course including practical work). In addition, a randomized crossover trial design was selected to minimize bias due to variability among the study participants. As a result, participants' clinical experience levels were not significantly correlated with the total execution times of the two methods.
Third, as with other studies using similar methodology, the participants could not be blinded to infusion devices they used. Finally, this study was performed in a simulated situation with an imitation arm and IV line. More stressful real-life situations may compromise operator performance. A before-and-after clinical study is needed to confirm the ability of the Anyfusion® to reduce medication errors related to the changeover process.
In conclusion, this study demonstrated that, compared to the conventional changeover method, the simplified changeover using the Anyfusion® reduced the number of button clicks and improved device usability by operators without affecting execution time. The ability of the Anyfusion® to reduce the workload of practitioners during a changeover process may reduce the risk of medication errors and subsequent patient harm.
 XML Download
XML Download