

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
It is often possible to carry out an organ preserving operation that ensures a high quality of life for patients during the early stages of breast cancer.1 The recurrence rate of patients with stage I of breast cancer (T1a, T1b and T1c) reaches 22%, and the 5-year relapse-free and overall survival in the general population is 84.3% and 93.4%.2 It is important to note that despite the high survival rates, only T1 tumors have a favorable outcome. At T1b and T1c stages, the characteristics of the tumors are more aggressive and this significantly worsens the outcome of the disease.3
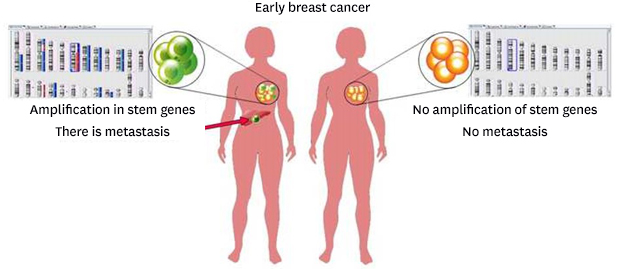
For early forms of breast cancer, it was found that the size of the primary tumor site affects the development of regional and distant metastases and the overall and relapse-free survival rates. Nowadays, the degree of malignancy, the hormonal status of the tumor, age, etc. are used as additional prognostic markers.4 There are various prognostic models for patients with early breast cancer, including multifactorial, but they all can predict the outcome of the disease in these patients with a small and relative accuracy.5 Thus, there is a need to search for additional prognostic markers in patients with early breast cancer to predict the outcome of the disease and determine the feasibility and extent of systemic (neoadjuvant and adjuvant) therapy. According to the results of our previous studies, it was found that during neoadjuvant chemotherapy (NAC) in breast cancer patients, clonal evolution of the tumor occurs - there is a change in the presence of tumor clones - their complete/partial disappearance or the emergence of new clones with amplifications of stem genes (locus 3q, 5p, 6p, 7q, 8q, 13q, 9p, 9q, 10p, 10q21.1, 16p, 18chr, 19p), which was associated with almost 100% metastasis.67 It has been suggested that the presence of amplifications of stem genes locus can lead to their ectopic expression and this is associated with an increased activity of tumor stem cells in these patients. This leads to a high aggressiveness of the tumor and the development of metastatic disease. Thus for studying prognostic significance, we studied the presence of amplifications locus of stem genes and their expression in patients with breast cancer stage I without systemic chemotherapy with metastases and without metastases.
METHODS
The study included 28 patients with T1NxM0 breast cancer (T1a, T1b, T1c), with a morphologically verified diagnosis, aged 29–64 years (mean age ± standard error, 48.5 ± 1.22 years) (Table 1). All patients underwent surgery. Adjuvant, radiation therapy and/or hormonal treatment was prescribed according to indications. The study was conducted in accordance with the 1964 Helsinki Declaration (revised in 2013).
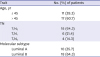
Table 1
Clinical and morphological parameters of the examined patients with breast cancer
| Trait | No. (%) of patients | |
|---|---|---|
| Age, yr | ||
| ≤ 45 | 11 (39.3) | |
| > 45 | 17 (60.7) | |
| TN | ||
| T1N0 | 18 (64.3) | |
| T1N1 | 6 (21.4) | |
| T1N2 | 4 (14.3) | |
| Molecular subtype | ||
| Luminal A | 10 (35.7) | |
| Luminal B | 18 (64.3) | |
As a test material we used a surgical specimen (around 60–70 mm3). The presence of tumor tissue in all samples was morphologically confirmed. Tumor samples were placed in a RNAlater solution (Ambion, USA) and stored at −80°C (after 24 hours incubation at +4°C) for further DNA and RNA isolation. We used the archive material from formalin-fixed paraffin-embedded (FFPE) for 8 patients.
DNA isolation
DNA was isolated from 28 tumor tissue samples using the QIAamp DNA Mini Kit (Qiagen, Hilden, Germany). DNA isolation from FFPE (n = 8) was carried out using the blackPREP FFPE DNA Kit (Analytik Jena, Jena, Germany). The DNA concentration and purity of the isolation was evaluated on a NanoDrop-2000 spectrophotometer (Thermo Scientific, Waltham, MA, USA) (from 10 to 120 ng/μL, A260/A280 = 1.95 − 2.05; A260/A230 = 1.88 − 2.20). DNA integrity was assessed by capillary electrophoresis using a TapeStation (Agilent Technologies, Santa Clara, CA, USA).
RNA isolation
Total RNA was isolated from 28 tumor samples using the RNeasy Mini kit Plus kit containing DNAasa I (Qiagen) with the addition of the RNA as inhibitor RiboLock (Fermentas, Vilnius, Lithuania) to the RNA solution. RNA isolation from paraffin blocks (n = 8) was carried out using the RNeasy FFPE Kit (Qiagen). The concentration and purity of RNA isolation was evaluated on a NanoDrop-2000 spectrophotometer (Thermo Scientific) (25–100 ng/μL, A260/A280 = 1.75–1.90; A260/A230 = 1.80–2.00). RIN was 5.6–7.0. To obtain cDNA on an RNA template, a reverse transcription reaction was performed using a RevertAid ™ kit (Fermentas) with random hexanucleotides.
Quantitative PCR
The expression level of stem genes (OCT3, SMO, MYC, SNAI2, MOB3B, KLF4, BMI1, VIM, FLT3, LAT, SMAD2, LMNB3, KLF1, TERT, TGFB1, TGFBR1) was assessed using reverse transcriptase quantitative real-time PCR (RT-qPCR) with original primers and probes using TaqMan technology on a Rotor-Gene-6000 amplifier (Corbett Research, Mortlake, Australia). PCR was set up in three replicas in a volume of 15 μL containing 250 μM dNTPs (SibEnzyme, Novosibirsk, Russia), 300 nM forward and reverse primers, 200 nM probe, 2.5 mM MgCl2, 19 SE buffer (67 mM Tris-HCl pH 8.8 at 25ºC, 16.6 mM (NH4) 2SO4, 0.01% Tween-20), 2.5 units of HotStart Taq polymerase (SibEnzyme) and 50 ng of cDNA. The two-step amplification program included 1 cycle - 94ºC, 10 minutes - pre-denaturation; 40 cycles - 1 step 94ºC, 10 seconds and 2 steps 20 seconds - at a temperature of 60ºC. Two referee genes were used as the referee gene: GAPDH (glyceraldehydes-3-phosphatedehydrogenase) and ACTB (actin beta), the level of gene expression was normalized in relation to the expression of the referee genes and measured in arbitrary units. Relative expression was estimated using the Pfaffl method. RNA from 20 patients, isolated from normal breast tissue obtained during the operation from patients who did not undergo NAC, was used as a calibrator.
Microarray analysis
Microarray analysis was performed on high-density DNA chips from Affymetrix (Santa Clara, CA, USA) CytoScanTM HD Array and using a FFPE OncoScan™ microarray (Affymetrix). Sample preparation, hybridization, and scanning procedures were performed according to the manufacturer's protocol on the Affymetrix GeneChip® Scanner 3000 7G system (Affymetrix). To process the results of microchipping, the program Chromosome Analysis Suite 3.3 (Affymetrix) was used, which was developed specifically for analyzing the results of micromatrix research. Using the program in the chromosomes, unbalanced chromosomal aberrations - deletions and amplifications (Loss and Gain), representing copy number aberration (CNA) were determined.
Statistical methods
Statistical data processing was carried out using the software package STATISTICA 8.0 (StatSoft Inc., Tulsa, OK, USA). Statistical processing of the results was carried out using the accepted methods of parametric and non-parametric statistics.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of the Oncology Research Institute of Tomsk National Research Medical Center of the Russian Academy of Sciences (protocol No. 1, January 14, 2013). Informed consent was submitted by all subjects when they were enrolled.
RESULTS
Table 2 presents data on the presence of amplifications of stem genes locus, as well as stem genes that are located in these locus in the studied patients.
Table 2
Data on the presence of amplifications locus of stem gene genes in patients without preoperative chemotherapy

Analysis of the CNA-genetic landscape of the studied tumors showed that 17 of 18 (94.4%) patients without metastases did not have two or more amplifications of chromosomal regions 3q, 5p, 6p, 7q, 8q, 13q, 9p, 9q, 10p, 10q21.1, 16p, 18chr, 19p, in which stem genes are localized (TERT, LIFR, OCT3, SOX4, NOTCH4, BMP6, FZD9, FZD1, WNT2, SMO, SNAI2, MYC, MOB3B, ALDH1A1, TGFBR1, KLF4, NOTCH1, KLF6, VIM, BMI1, ZEB1, ITGB1, NANOG, FLT3, SMAD9, KLF5, ZIC2, SOX1, LAT, SMAD2, SMAD4, LMNB2, INSR, KLF1, KLF2, TGFB1). In 5 of 17 patients (patients D2, P1, S1, S4, U1) there were single amplifications of these chromosomal regions. The frequency of cytobends with CNA (the number of cytobends with CNA/total number of cytobends in the human genome 862) in the group of patients without hematogenous metastases did not exceed 25%. Interestingly, the patient M3 had six amplifications in the tumor, and the absence of progression within 6 years after treatment. Despite this, the chance of metastasis remains at a later date.
Ten patients had visceral metastases at various times after surgery (from 3 to 120 months). In 9/10 (90%) of these patients in the primary tumor there were two or more amplifications of the stem genes and this, in our opinion, predetermined an unfavorable outcome in these patients. One patient (E1) in the tumor had only 1 amplification of the TGFB1 stem gene on the long arm of chromosome 19 and the development of metastatic disease was observed three years after the operation (Table 2). It is well known that amplifications very often lead to increased expression of genes located in amplification sites and/or readiness to increase expression of these genes in response to external stimulation.8 The expression of 16 stem cells genes (OCT3, SMO, MYC, SNAI2, MOB3B, KLF4, BMI1, VIM, FLT3, LAT, SMAD2, LMNB3, KLF1, TERT, TGFB1, TGFBR1), located in different chromosomes in this patient was also evaluated. A comparison was made with the expression of stem genes in tumors of patients without metastases who did not have amplifications of stem gene genes or there was only 1 amplification in the tumor (Fig. 1).
Fig. 1
Heat maps of stem gene expression in patients with early breast cancer with the absence or presence of 1 amplification of stem genes locus.
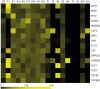
Despite the presence of only one amplification in patient E1, there is a very high expression of 7 stem genes (OCT3, SMO, LAT, LMNB2, KLF1, TGFB1, TGFBR1), which is 2–18 fold higher than in the other examined patients with 1 amplification or without amplification of stem gene genes. In this case, overexpression of stem genes is not due to amplification, but to some other mechanisms that may be associated with their regulation, for example, hypomethylation of the promoters of these genes, miRNA, and other mechanisms. As a result of the study, it was shown that in patients with stage I tumors who developed metastases, most had either 2 or more stem cell amplification (90%). While in the tumor of patients with a favorable outcome, there was a low expression of stem genes and no more than 1 amplification of their localization regions. This shows that the presence of 2 or more amplifications of stem genes is a good prognostic marker. Along with this, the relationship of the age of the studied patients with the presence of stem gene amplifications was evaluated. A very interesting result was obtained, using the Mann-Whitney criterion it was shown that the age of patients with 2 or more amplifications was statistically significantly higher compared to the other group (55.3 ± 4.48 vs. 47.3 ± 2.16; P = 0.03).
Further, using the Kaplan-Meier method, we estimated the metastatic-free survival in groups of patients with 1 or without amplifications and with two or more amplifications (Fig. 2).
Fig. 2
Non-metastatic survival of patients with breast cancer depending on the presence/absence of amplifications in the regions where the stem genes are located.
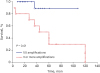
It was found that the 5-year survival of patients with one or no amplifications is 89%, compared with the second group, in which this indicator is only 30%. The differences are statistically significant (log-rank test P = 0.01).
DISCUSSION
Currently, the prognostic significance of many clinical and morphological factors is well studied. The degree of malignancy (high or low) allows us to predict the frequency of relapses with a sensitivity of 74% and a specificity of 12%.9 A large multicenter study, which included more than 1,000 patients with early breast cancer without prescribing adjuvant systemic treatment, showed that both age and molecular genetics subtype affect long-term results, but have low diagnostic value.1011 Experts St. Gallen did not find evidence in favor of assigning an adjuvant chemotherapy in N+ status (less than 3 affected lymph nodes), but the vast majority of them recommend chemotherapy in this case. To date, only two molecular genetic test systems: Oncotype DXTM and MammaPrint, are allowed for clinical use by experts from the FDA USA and St Gallen. According to the NSABP-B14 study, the risk of distant metastasis for 10 years, estimated by OncotypeDX, is 6.8% (4%–10%), 14.3% (8%–20%) and 30.5% (24%–37%) for low, moderate and high risk (P < 0.001).12 In other words, OncotypeDX is 70% mistaken in predicting a high risk of recurrence for a high-risk group, and in 7% of cases it is mistaken in predicting a favorable outcome in a low-risk group. Nevertheless, even this low OncotypeDX prognosis makes it possible to benefit for the patient, and in the NSABP B20 study, it was demonstrated that chemotherapy for high-risk patients can increase patient survival by 28% (from 60% to 88%), while the effectiveness of chemotherapy in the group low risk remained unproved.13 Today, no prognostic model makes it possible to unify the indications for determining the need for and the selection of the adjuvant systemic therapy scheme, so that it is possible to talk about the individualization of the treatment program. It is necessary to search for markers that determine the prognosis of the disease and the need for adjuvant therapy. In this sense, our results allowed us to demonstrate 83% of the sensitivity and specificity of 83%, which is significantly higher than all prediction factors used for early breast cancer. This makes promising further research in this direction.
According to the literature, with an increase in the age of patients, an increase in the number of chromosomal abnormalities is shown, and stem gene loci are not an exception.1415 Moreover, it was found that at the age of 45 years and more, most women begin hormonal changes in the body associated with the menopausal period.16 It can be assumed that a decrease in the level of female sex hormones may have an indirect effect on the appearance of new structural chromosomal rearrangements. According to the results of our study, elderly age along with determining the number of stem gene amplifications, can be considered as an additional criterion that defines the assignment of patients to an increased risk group for the development of metastatic disease. But this issue requires further additional research.
It was found that the OCT3 gene (POU5F1), whose function is to maintain pluripotency and stem cell self-renewal, is involved in tumor progression.1718 In addition, it was established that overexpression of this gene is statistically significantly associated with metastasis (P < 0.001) in patients with breast cancer.19 LMNB2 belongs to the lamin B-type family and plays a key role in maintaining the structural integrity of the nucleus and chromosomal stability. It was shown that overexpression of this gene in non-small cell lung cancer contributes to increased invasion and development of the tumor process.20 LAT is over-expressed in many types of cancer, and is associated with an unfavorable outcome for patients with endometrial cancer and breast cancer.21 The high expression level of BMI1 was significantly correlated with the presence of metastasis in the axillary lymph nodes, tumor progression and hematogenous metastasis of invasive ductal carcinoma.22 Although other authors found that the expression of BMI-1 protein in breast tumor tissue was associated with a favorable prognosis. Studies by other authors have shown that low expression of the MOB3B gene in prostate cancer is associated with tumor progression and the development of metastatic disease.23
In conclusion, our studies have shown that the presence in the primary tumor of patients with breast cancer T1NxM0 clones carrying two or more amplifications of the stem gene genes in 3q, 5p, 6p, 7q, 8q, 9p, 9q, 10p, 10q21.3, 13q, 16p, 19p, has a prognostic significance and determines the unfavorable prognosis in distant metastasis. At present, it is necessary to conduct more extensive studies of the significance of stem gene amplification in early forms of breast cancer.
 XML Download
XML Download