

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Yong-Sik Lee, Il-Hyun Nam , Tae-Hun Lee, Gil-Yeong Ahn, Yeong-Hyeon Lee, Hee-Hyung Lee, Sung-Hyun Hwang
, Tae-Hun Lee, Gil-Yeong Ahn, Yeong-Hyeon Lee, Hee-Hyung Lee, Sung-Hyun Hwang
, Tae-Hun Lee, Gil-Yeong Ahn, Yeong-Hyeon Lee, Hee-Hyung Lee, Sung-Hyun Hwang
Abstract
Purpose
The aim of this study is to evaluate if the Ilizarov external fixation procedure with axial compression can help to obtain fusion across the ankle joint in patients with a high risk of nonunion.
Materials and Methods
From January 2006 to December 2015, the study reviewed 17 patients who underwent ankle arthropathy with a high risk of nonunion and who underwent ankle fusion using the Ilizarov external fixator with axial compression and auto bone grafting. After the lateral surface of the ankle joint was exposed through a lateral trans-fibular approach, massive removal of the articular cartilage and excision of any loose or avascular bone were done. With the cortical bone harvested from the pelvis as corticocancellous bone blocks, we inserted the two cortical blocks longitudinally into the anterior and posterior part of the free ankle space from lateral to medial to make the rectangular chamber to fill the cancellous bones. After the Ilizarov external fixator was equipped, we tightened the frame by 5 mm to compress the bone graft space. We accessed the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot score both preoperatively and postoperatively.
Results
The average age at the time of operation was 63.4 years (range, 47~78 years). The mean frame time was 17.4 weeks (range, 15~23 weeks). The average follow-up period was 3.7 years (range, 2~6 years). Osseous fusion was obtained in 15 patients (88.2%). There were two stable pseudarthroses among the rheumatoid arthritis patients, and we continued their follow-up. The mean AOFAS Ankle-Hindfoot score improved from 48.5 to 73.7 points.
Figures and Tables
 | Figure 1(A) The left ankle of a 78-year-old female with rheumatoid arthritis shows marked secondary arthritis. (B, C) Articular cartilage and sclerotic avascular bone around the ankle joint were massively removed. (D) Temporary fixation through the calcaneus, talus, and tibia was done using a Steinman pin.
|


 | Figure 4(A) A 53-year-old male, lateral radiograph showed avascular necrosis of the talar body due to comminuted fracture of the talus. (B) Necrotic talar body was removed completely. (C) We inserted two cortical blocks longitudinally into the anterior and posterior part of free ankle space from lateral to medial to make a rectangular chamber. (D) We filled the chamber with the autogenous cancellous bones. (E) We confirmed the solid bony union at 26 weeks after operation.
|
 | Figure 5(A, B) After the Ilizarov external fixator which was composed of two tibial rings and one foot plate was equipped, we tightened the frame by 5 mm to compress the bone graft space.
|
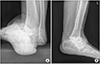 | Figure 6(A) Anteroposterior radiopraph of a 65-year-old male with diabetic charcot neuroarthropathic joint. (B) We confirmed the solid bony union at 38 weeks after operation.
|


References
1. Yasui Y, Hannon CP, Seow D, Kennedy JG. Ankle arthrodesis: a systematic approach and review of the literature. World J Orthop. 2016; 7:700–708. DOI: 10.5312/wjo.v7.i11.700.

2. Glick JM, Morgan CD, Myerson MS, Sampson TG, Mann JA. Ankle arthrodesis using an arthroscopic method: long-term follow-up of 34 cases. Arthroscopy. 1996; 12:428–434. DOI: 10.1016/s0749-8063(96)90036-5.
3. Townshend D, Di Silvestro M, Krause F, Penner M, Younger A, Glazebrook M, et al. Arthroscopic versus open ankle arthrodesis: a multicenter comparative case series. J Bone Joint Surg Am. 2013; 95:98–102. DOI: 10.2106/JBJS.K.01240.
4. Colman AB, Pomeroy GC. Transfibular ankle arthrodesis with rigid internal fixation: an assessment of outcome. Foot Ankle Int. 2007; 28:303–307. DOI: 10.3113/FAI.2007.0303.
5. Cameron SE, Ullrich P. Arthroscopic arthrodesis of the ankle joint. Arthroscopy. 2000; 16:21–26. DOI: 10.1016/s0749-8063(00)90123-3.
6. Mann RA, Van Manen JW, Wapner K, Martin J. Ankle fusion. Clin Orthop Relat Res. 1991; (268):49–55.
7. Clifford C, Berg S, McCann K, Hutchinson B. A biomechanical comparison of internal fixation techniques for ankle arthrodesis. J Foot Ankle Surg. 2015; 54:188–191. DOI: 10.1053/j.jfas.2014.06.002.
8. Early JS, Hansen ST. Surgical reconstruction of the diabetic foot: a salvage approach for midfoot collapse. Foot Ankle Int. 1996; 17:325–330. DOI: 10.1177/107110079601700605.
9. Sammarco GJ, Conti SF. Surgical treatment of neuroarthropathic foot deformity. Foot Ankle Int. 1998; 19:102–109. DOI: 10.1177/107110079801900209.
10. Yousry AH, Abdalhady AM. Management of diabetic neuropathic ankle arthropathy by arthrodesis using an Ilizarov frame. Acta Orthop Belg. 2010; 76:821–826.
11. El-Alfy B. Arthrodesis of the ankle joint by Ilizarov external fixator in patients with infection or poor bone stock. Foot Ankle Surg. 2010; 16:96–100. DOI: 10.1016/j.fas.2009.06.004.
12. Onodera T, Majima T, Kasahara Y, Takahashi D, Yamazaki S, Ando R, et al. Outcome of transfibular ankle arthrodesis with Ilizarov apparatus. Foot Ankle Int. 2012; 33:964–968. DOI: 10.3113/FAI.2012.0964.
13. Campbell P. Arthrodesis of the ankle with modified distraction-compression and bone-grafting. J Bone Joint Surg Am. 1990; 72:552–556.
14. Charnley J. Compression arthrodesis of the ankle and shoulder. J Bone Joint Surg Br. 1951; 33B:180–191.
15. Ilizarov GA, Okulov GV. [Compression arthrodesis of the ankle joint and adjacent foot joints]. Ortop Travmatol Protez. 1976; (11):54–57. Russian.
16. Fragomen AT, Borst E, Schachter L, Lyman S, Rozbruch SR. Complex ankle arthrodesis using the Ilizarov method yields high rate of fusion. Clin Orthop Relat Res. 2012; 470:2864–2873. DOI: 10.1007/s11999-012-2470-9.
 XML Download
XML Download