

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ventricular arrhythmia (VA) remains the major cause of mortality and sudden cardiac death (SCD) in patients suffering from acute myocardial infarction (AMI). It is well known that sympathetic hyperactivity is involved in VA during such episodes.1) The sympathetic nervous system has been implicated in the initiation and perpetuation of VA. Recently the beneficial effect of renal denervation (RDN) has been documented in patients suffering from hypertension.2) These effect in hypertensives showed that RDN could modulate the sympathetic nervous system and ventricular electrophysiology.3)4)5)6)7)8) However, antiarrhythmic effect of catheter based RDN after AMI in the early period remains unclear. The goal of the present study was to evaluate the short-term effect of RDN on VA in a porcine model of the induction of AMI.
METHODS
Animal preparation
This study was approved by the Ethics Committee of Chonnam National University Medical School and Chonnam National University Hospital (CNU IACUC-H-2013-12), and conformed to the Guide for the Care and Use of Laboratory Animals published by the United States National Institutes of Health (NIH Publication No. 85-23, revised 1996). Our study included 20 pigs from the animal catheterization laboratory of Chonnam National University Hospital. Yorkshire×Landrace F1 crossbred castrated male pigs (20–25 kg) were used, and observed in the laboratory animal center of Chonnam National University Medical Institute for 5–10 days before the experiment. Experiment protocol was described in Figure 1.

Anesthesia
All pigs were fasted for 24 hours with unlimited access to water before the procedure. On the day of the procedure, the pigs were anesthetized with zolazepam and tiletamine (2.5 mg/kg, Zoletil50®, Virbac, Carros, France), xylazine (3 mg/kg, Rompun®, Bayer AG, Leverkusen, Germany), and azaperone (6 mg/kg, Stresnil®, Janssen-Cilag, Neuss, Germany). Intravenous (IV) fluid administration with 0.9% saline was continued throughout the experiment. After intubation, anesthesia was maintained with an inhalation anesthetic mixture of sevoflurane (1%) in oxygen (100%). The pigs were ventilated mechanically.
Loop recorder implantation for assessing ventricular arrhythmia
After achieving anesthesia, a loop recorder (SJM Confirm®, St. Jude Medical, Inc., St. Paul, MN, USA) was implanted for the detection of VA. We used Vector Check electrodes and conductive patches to determine the preferred implantation site and device position. An implantable loop recorder (ILR) was implanted subcutaneously into the left pectoral region. A small incision was made and subcutaneous tissues were dissected to the muscular level. The cleavage plane between the left pectoralis muscles was gently dissected manually. Once the ILR had been inserted into the submuscular pocket, the amplitude of the spontaneous R wave was measured through the device's telemetry. The device was then anchored through the 2 suture holes of its header and the surgical wound was sutured. The electrodes were oriented outward. The basic electrocardiographic requirements for subpectoral implantation were an R-wave amplitude of at least 0.3 mV and a peak-to-peak R-wave amplitude of at least twice the peak T- and P-wave amplitudes. R-wave amplitudes were determined at implantation and during follow-up. These were defined as the mean value of a manual peak-to-peak measurement of at least 5 consecutive signals. No complications occurred during the implantation. Storage of the electrocardiography (ECG) can be initiated manually or is triggered automatically when arrhythmic events fulfill preprogrammed cutoff criteria. Electrogram (EGM) can be stored for 5 minutes manually. Loop recorder (SJM Confirm®) can detect 4 episodes such as asystole, bradycardia, tachycardia, atrial fibrillation. Data were stored automatically when arrhythmic events corresponded to the following preprogrammed criteria: sinus arrest >3 seconds, ventricular tachycardia (VT) >125 bpm for more than 8 beats, or sustained VT >30 seconds, like other study.9)
Induction of acute myocardial infarction
A 7F arterial sheath was placed in the left carotid artery under local anesthesia with 2% lidocaine. After infusion of 10,000 units of heparin, a 7F coronary artery guiding catheter was placed within the opening of the coronary artery and a baseline coronary angiogram was obtained under fluoroscopic guidance using a mobile C-arm (Phillips BV-25 Gold; Phillips BV, Eindhoven, Netherlands). AMI was induced by embolization using polyethylene terephthalate in the middle left anterior descending artery (LAD), just distal to the second diagonal branch or the septal branch. During the experiment, oxygen and normal saline were supplied continuously and anesthesia was maintained with an additional administration of zolazepam (1.25 mg/kg, IV), tiletamine (1.25 mg/kg, IV), xylazine (1.5 mg/kg, IV), and azaperone (6 mg/kg, intramuscular injection). Continuous electrocardiographic monitoring was performed to confirm a normal ST segment at baseline, any ST elevation during the ischemic period, and to monitor any occurrence of cardiac arrhythmia.
Radiofrequency ablation of renal sympathetic nerves
After the induction of AMI, the pigs were randomly divided into 2 groups: RDN with AMI (n=10) or Sham with AMI (n=10). Aortography at the level of the renal arteries was performed via the left carotid artery sheath, followed by catheterization and selective renal arteriography for the evaluation of the anatomy. An ablation catheter (Simplicity, Medtronic Inc., Minneapolis, MN, USA) was placed in each branch of the renal artery in the RDN group. At least 6 radiofrequency (RF) currents (6–8 W, 120 seconds) were delivered along both renal arteries, starting from the renal artery branch or distal segments toward the proximal segments and the ostium. For the first set of ablation lesions, the most distal electrode was placed 0.5 cm proximal to the bifurcation/trifurcation of the renal artery. The catheter was pulled out and with a 45° rotation of the catheter, a second ablation was performed to produce lesions proximal to the first set. Each ablation was rotated after each RF delivery, thus producing a spiral configuration of the ablations.10) Bilateral RDN was achieved by ablation at 6 to 8 sites in each renal artery. The sham procedure used the same method but no RF current was delivered. ECG was monitored closely for 1 hour to observe development of any VA and then animals were carried back to the animal house and monitored until recovery.
Serum norepinephrine measurements
Serum norepinephrine (NE) concentration levels were determined according to the manufacturer's protocol (Noradrenalin ELISA Kit, MyBioSource, Inc, San Diego, CA, USA). Briefly, 50 µL serum (myocardial infarction [MI]+RDN, MI+Sham) and standard solutions were added to 96 well pre-coated plates. After the addition biotin-detection antibody to 96 well plates, they were mixed thorough and incubated for 45 minutes at 37°C. The plate was washed and HRP-streptavidin conjugate to each well for 30 minutes at 37°C. After 5 times washing, TMB substrate was added to each well for 15 minutes at 37°C and then stop solution to each well. The substrate/HRP reaction was read at 450 nm. Quantitative analysis of samples was calculated from a 4 parameter logistic curve fit.
Follow-up angiograms and tissue preparation for pathologic analysis
One week later, animals underwent follow-up angiography (coronary artery and renal angiograms) in the same orthogonal views to check for vessel patency. At the end of the experiment, the pigs were anesthetized and euthanized with an overdose of potassium chloride. The heart and kidney were extracted. The extracted heart was rinsed, and myocardial sections including the left ventricle (LV) and right ventricle were obtained at 1-cm intervals using a microtome knife. The myocardial sections were incubated in 2,3,5-triphenyl tetrazolium chloride (TTC) solution until regions of viable myocardium turned brick red. Histomorphometrically, infarct size was estimated on digital photographs of TTC staining by outlining the LV area and TTC-negative infarct areas. Infarct size was then expressed as the % LV area. Kidney biopsy was carried out to obtain samples of renal arteries and macroscopic and histological assessment of the arterial wall and perirenal nerves.11) All procedures were provided by a skilled pathologist.
Analysis of loop recorder
Explanted ILR data were analyzed. ECG intervals were measured by 2 investigators blinded to the RDN procedure. The RR and QT intervals were measured by manual positioning on screen marker lines. For definition of the ECG intervals, 3 vertical marker lines were located on each ventricular cycle: the first at the beginning of the QRS complex, the second at the peak of the R wave, and the third at the end of the T wave. RR intervals were defined as cycle length; interval between the peaks of 2 consecutive R waves. QT intervals were defined as the interval between the first deviation of the QRS complex from the isoelectric line and the end of the T wave. The end of the T wave was defined as the point at which the curve of the T wave returned to the isoelectric line. The QTc interval was measured by Bazett's formula. When an R wave seen in an arrhythmic beat chopped off the end of the T wave, then the end of the T wave was defined as the point at which the QRS complex of the subsequent R wave started on the next T wave. The QRS complex that interrupted the T wave of the preceding beat was defined as an R on T arrhythmic beat. A premature ventricular complex (PVC) was measured in 500 consecutive ventricular ECG complexes immediately preceding the VT/ventricular fibrillation (VF) onset.
VAs during acute MI are typically classified based upon their time of onset. A distinction was made between the acute phase of myocardial ischemia (during 1 hour) and the subacute or delayed phase (6 to 48 hours post-MI).12)
Statistical analysis
Analysis was performed using IBS SPSS statistics (version 21.0; IBM Corp., Armonk, NY, USA). Fisher's exact test was used to compare the occurrence of VA in the RDN and Sham groups. Continuous variables are presented as the mean value±1 standard deviation; comparisons between means were conducted using Student's t-test, or using the nonparametric Kruskal–Wallis test if the normality assumption was violated. For all statistical analyses, the null hypothesis was rejected at the 95% confidence level, considering a p value<0.05 as significant. Mortality rates among experimental animals during the follow-up were analyzed using the Kaplan–Meier method.
RESULTS
Coronary angiographic findings
Coronary angiograms confirmed occlusion of the middle LAD (Figure 2). After the procedure, a repeated coronary angiogram showed acute obstruction of the middle LAD in all pigs. When a follow-up angiogram was performed after 1 week, the occlusion had been maintained in all animals.
Figure 2
Coronary angiogram and renal artery angiogram. (A) Coronary angiogram, baseline. (B) Occlusion of the middle left anterior descending artery just distal to the diagonal branch. (C) Follow-up coronary angiogram at 1 weeks. (D) Renal artery angiograms, baseline. (E) Renal artery angiogram after radiofrequency ablation. (F) Renal artery angiogram after 1 week. White arrow indicates occlusion site.

Renal denervation
RDN was performed in both renal arteries in the RDN group. The mean number of complete RF applications was 7.2±1.2 in the right renal artery and 7.3±1.9 in the left renal artery. There were no major procedure-related complications in both sham and RDN group. There were mild renal artery irregularities immediately after RF applications on angiogram. However, those irregularities did not affect renal artery blood flow. Follow-up angiogram after the procedure showed good patency of procedure related renal artery. Also, there was no evidence of aneurysms, procedural injury, dissection, appreciable arterial dilation, or filling defects with mild narrowing.
Implantable loop recorder data analysis
Implantation
The average R-wave amplitude measured by the ILR was 0.65±0.26 mV. No complications occurred during the ILR implantation.
Incidence of ventricular arrhythmias
Total number of VF was not different between 2 groups in acute phase (Table 1). All VF episodes were terminated by successfully by external defibrillation. However, incidence of VF was lower in the RDN group compared to Sham group in delayed phase. Also, the total number of non-sustained or sustained VT was lower in the RDN group in early period.
Table 1
VAs after AMI

Frequency of premature ventricular complexes
Before coronary occlusion, there was no PVC in all pigs. Immediately preceding the onset of VA, the frequencies of PVC increased in both groups, and were significantly greater in the Sham group 19.4% vs. 3.5%, p=0.01; Figure 3). Most episodes of VF were triggered by PVCs (R on T phenomenon).
Figure 3
Effects of RDN on the occurrence of spontaneous PVC induced by occlusion of the left anterior descending coronary artery. The frequencies of PVC increased in both groups and were significantly greater in the Sham group. PVC triggered ventricular fibrillation (black arrow).
PVC = premature ventricular contraction; RDN = renal denervation.

Effect of corrected QT intervals
The baseline QTc was 485±28 ms. After AMI, QTc interval was prolonged in both groups and were significantly greater in the Sham group (Figure 4). QTc interval returned to normal in all pigs after 1 weeks.
Figure 4
(A) A representative electrogram complex from a heart undergoing occlusion of the middle left anterior descending artery is shown. The QTc interval was prolonged from 438 ms to 608 ms. (B) Line graph displaying the average QTc interval at baseline, after AMI induction, after the renal denervation procedure, and 1 week later. After AMI, QTc interval was prolonged in both groups and were significantly greater in the Sham group. QTc interval returned to normal in all pigs after 1 weeks.
AMI = acute myocardial infarction; QTc = corrected QT.

Impact on renal denervation on serum norepinephrine concentration
There was no significant difference serum NE level between groups at baseline state. Serum NE level was remarkably increased in both groups and were significantly greater in Sham group after 1 hour (7.21±5.62 vs. 1.78±1.03, p=0.045; Figure 5).
Figure 5
Effect of RDN on serum NE at baseline, and 60 minutes after AMI. In the baseline state, no significant difference was observed in serum NE between RDN (black bar) and Sham group (grey bar). After 1 hour of AMI, serum NE level was remarkably increased in both groups and were significantly greater in the Sham group.
AMI = acute myocardial infarction; NE = norepinephrine; RDN = renal denervation.

Pathologic analysis of the heart and kidney tissues
The extracted heart in fourteen pigs showed that LAD occlusion resulted in a large infarction area of similar size. Infarction area was not different between 2 groups. (17.4±3.9% to 13.8±2.9% of the LV area; p=0.091). There was no significant difference in the mass of the myocardial infarct area between the 2 groups.
As shown in Figure 6, hematoxylin and eosin stain stating showed inflammatory response in the renal artery, which means catheter ablation was successfully done. The adventitia of renal arties in the RDN group exhibited shows loss of endothelium and medial thinning and fibrosis but this was not seen in the Sham group, confirming that this was not because of instrument placement but from the RF energy delivered to the renal arteries.
Figure 6
Histology of the renal artery. (A) H&E stain of the renal artery at low magnification shows degenerated renal artery and periarterial nerves. Renal artery shows loss of endothelium and medial thinning and fibrosis (black arrow). (B) High magnification view with H&E staining shows fibrosis of perineurium, marked pyknotic nuclei, eosinophilic change of nerve fibers, vacuolization, and inflammation (black arrow).
H&E = hematoxylin and eosin.

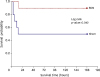
Arrhythmic events
Six pigs died during the follow-up period. VF occurred within 24 hours after the infarction in all expired pigs according to analysis of the ILR data. VF developed more frequently in sham group than RDN group during follow up period (1 death in the RDN group vs. 5 in the Sham group; p=0.041; Figure 7). One pig in the Sham group developed a paroxysmal complete atrioventricular block.
DISCUSSION
AMI induced by occlusion of the middle LAD was associated with a high incidence of VA. RDN significantly reduced VA and the risk of arrhythmic death by restoring electrical stability, which was associated with an attenuation of PVCs and QT prolongation.
VA remains the major cause of mortality and SCD in patients suffering from AMI. Death from a ventricular tachyarrhythmia in the setting of AMI has been one of the most frequent causes of SCD. About 60% of deaths associated with AMI occur within the first hour and are attributable to VA. The causes of electrical instability in association with AMI are various, and are associated with increased ventricular automaticity, reduced vagal tone, and decreased VF threshold.1) The sympathetic nervous system has been implicated in the initiation and perpetuation of VA. Relative excess of sympathetic compared to vagal activity may be an important factor in genesis of VA during AMI.13) RDN was known to reduce renal sympathetic activity as assessed by NE spillover, modulate the sympathetic nervous system and to reduce recurrent VA.3)4)5)6)7)8)14) RDN has been shown to suppress spontaneous PVC and reduced the incidence of VF in pig model.
The frequencies of PVC increased after occlusion of middle LAD in our study. The presence of PVC after acute MI were associated with an increased total mortality among post MI patients, particularly those with larger infarctions and impaired left ventricular function.15) Early R on T PVCs might be of particular concern in patients with ST-elevation MI.16) In our experiments, all arrhythmic deaths appeared as R on T PVC. PVCs that initiate reentry might be reentrants themselves, or might arise via activity triggered from Purkinje fibers in ischemic regions in response to increased catecholamine levels.17) Myocardial ischemia is associated with triggered activity, mainly characterized by delayed after-depolarization (DAD) episodes caused by intracellular calcium overload.18) Autonomic modulation might attenuate DADs, explaining the reduced occurrence of PVCs during VA.19) Thus, by reducing cardiac sympathetic nervous activity, RDN might be effective in reducing the occurrence of spontaneous PVCs after AMI, as seen in our study.
AMI induced by middle LAD occlusion prolonged the QT interval in our study. It is well known that the QT interval generally increases during AMI.20) Several mechanisms have been proposed for this: changes in the myocardial response to catecholamines; perturbation of calcium or potassium ion channels; or the induction of changes in the intracellular hydrogen concentration. Zhou reported that electric stimulation of the left stellate ganglion produced lengthening of a QTc interval, and spontaneous increased stellate ganglion nerve activity was observed before VT/VF events in canine models.21) Similarly, the QT interval was prolonged after AMI and was not increased any more after RDN compared with the Sham group in our study. This suggests that RDN might inhibit QT prolongation after AMI.
The frequency of VA caused by occlusion of the middle LAD within 1 hour was not different between the 2 groups. Pathogenesis of VA differs in the acute and subacute phases of the early post MI period.12) RDN itself could not prevent VA after AMI immediately in this study. However, incidence of VF was higher in Sham group (subacute or delayed phase). Also, the frequency of non-sustained or sustained VT was higher in Sham group in 1 week. RDN decreased VA following an AMI within 1 hour and this effect lasted 1 week.
This study had some limitations. First, the degree of MI may not be the same in both groups even though the data showed the TTC staining had a similar infarct area. We had to check myocardial enzyme levels during the experiment but could not. Second, we performed RF ablation of renal sympathetic nerves without definitive endpoints. However, we confirmed damaged nerve bundles from renal artery biopsy. Third, a carotid arterial sheath was used instead of a femoral arterial sheath for the induction of AMI and for performing RDN. Cervical hematomas might also cause pressure to the carotid sinus and affect the autonomic nervous system adversely. Fourth, ILR has several limitations in recording cardiac arrhythmias, some related to inherent limitations in the detection channel and some related to the prespecified arrhythmia detection criteria. It is possible that other important forms of arrhythmia were missed because of these inherent limitations and limited memory in the ILR. In particular, there were several differences between surface ECG and EGMs recorded by the ILR: 1) different filter settings; 2) different positions of the lead axis; and 3) different spatial scales in the assessment of QT prolongation. Finally, small sample size of the study could have biased the results of some statistical tests. Further larger trials are necessary to clarify these topics.
In conclusion, here, we demonstrated that RDN reduced PVCs, inhibited QTc prolongation, and significantly decreased VA and the risk of arrhythmic death in the early period after AMI in a porcine model. These results suggest that RDN might be a therapeutic option in patients with electrical instability after AMI.
 XML Download
XML Download