

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Peyronie disease (PD) is characterised by the presence of penile pain, deformity, and plaque, with ensuing erectile dysfunction (ED) in advanced cases [1]. At present, a wide range of medical therapies have been utilised for symptomatic PD, many with little-proven benefits, apart from intralesional injection of collagenase Clostridium histolyticum, which to date remains the only approved medical therapy for PD [12]. Although it remains a doctrine that most patients should wait for a minimum of 12 months for the disease to stabilise before surgical intervention, support for this dogma is primarily based on expert opinion, rather than empirical data [123].
Penile reconstructive surgery provides the fastest, most reliable, and most sustained clinical outcomes for the correction of penile deformities. Major international guidelines advocate that surgery should be considered in men with stable PD (once the penile deformity has remained stable and painless for at least 3 months); in the presence of significant penile deformity with difficult intercourse and/or hour-glass or hinge-deformity; and following the failure of conservative treatment or when the patient wants the most definitive possible result [12345]. It should be noted that the surgical outcomes for patients in the active phase are largely unknown. The selection of the appropriate surgical reconstruction in each patient depends on many factors, including an in-depth understanding of the state of PD; patients' expectations related to the outcomes of surgical intervention; and anticipated adverse surgical outcomes, especially postoperative penile length and girth, as well as ED.
The aims of this review are to provide an overview of the current approaches to penile reconstructive surgery in patients with PD and to discuss the challenges in attaining normal penile size and function in men with PD.
Go to : 
MATERIALS AND METHODS
A systematic literature search was conducted to identify published literature relevant to PD and penile reconstructive surgery. English-language publications were searched for in the Medline database using MeSH terms such as ‘Peyronie's disease’, ‘penile reconstructive surgery’, ‘plication’, ‘graft’, ‘penile prosthesis implant’, ‘penile length’, ‘erectile dysfunction’, ‘penile curvature’, ‘sensory change’, and ‘surgical outcomes’. A summary of the published guidelines from major organisations, such as the International Consultation on Sexual Medicine (ICSM) or the International Society of Sexual Medicine (ISSM), the American Urological Association (AUA), and the European Association of Urology (EAU) is included in this review paper.
Go to :
DISCUSSION
1. Types of penile reconstructive surgery
Penile reconstructive surgery for PD is largely divided into 3 major types: penile plication (shortening the convex side), graft surgery (lengthening the concave side of the tunica albuginea [TA] by incision or partial excision of the plaque with the use of various graft materials for closure of the defect), and penile prosthesis implants (PPIs) with or without adjunctive measures, such as penile remodelling, plication, and grafting (Table 1).
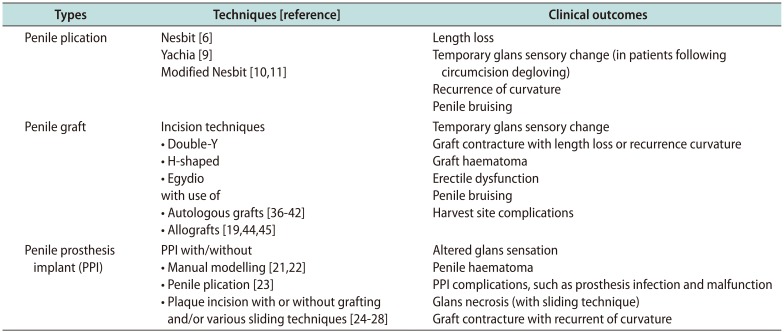
Table 1
Types and clinical outcomes of various penile reconstructive surgical techniques in peyronie disease
| Types | Techniques [reference] | Clinical outcomes |
|---|---|---|
| Penile plication | Nesbit [6] | Length loss |
| Yachia [9] | Temporary glans sensory change (in patients following circumcision degloving) | |
| Modified Nesbit [1011] | Recurrence of curvature | |
| Penile bruising | ||
| Penile graft | Incision techniques | Temporary glans sensory change |
| • Double-Y | Graft contracture with length loss or recurrence curvature | |
| • H-shaped | Graft haematoma | |
| • Egydio with use of | Erectile dysfunction | |
| • Autologous grafts [36373839404142] | Penile bruising | |
| • Allografts [194445] | Harvest site complications | |
| Penile prosthesis implant (PPI) | PPI with/without | Altered glans sensation |
| • Manual modelling [2122] | Penile haematoma | |
| • Penile plication [23] | PPI complications, such as prosthesis infection and malfunction | |
| • Plaque incision with or without grafting and/or various sliding techniques [2425262728] | Glans necrosis (with sliding technique) | |
| Graft contracture with recurrent of curvature |
![]()
Penile plication techniques are generally recommended in men with mild to moderate penile curvature (less than 60°) without concurrent hour-glass or hinge-defect deformity. The original penile plication procedure was described by Nesbit in 1965 and involves the excision of an ellipsoid area of tissue from the TA on the opposite side of the penis to the most prominent point of penile curvature, thereby shortening of the convex side of the penis after closure of the tunica defect [6]. The mobilization of the neurovascular bundle (NVB) for the correction of ventral deformities can be achieved by medial or lateral dissection of the NVB depending on the surgeon's expertise [7]. Several modifications of the Nesbit procedure have been published, including the use of multiple small superficial TA excisions with primary closure and TA U-shaped flaps [8]. The Yachia [9] procedure involves modification of the Nesbit technique based on the Heineke-Mikulicz principle, with a single long incision or multiple small incisions made longitudinally in the TA and subsequently closed horizontally to shorten the convex side of the penis. Another penile plication technique, first described by Essed and Schroeder [10], utilises the placement of nonabsorbable sutures over the convex side of the TA, without the need for excision of the TA or mobilization of the NVB. More recently, Gholami and Lue [11] popularised the 16-dot (2 pairs of plication) or 24-dot (3 pairs of plication) plication technique without tunical incision or excision, which avoids any mobilisation of the NVB or corpus spongiosum.
Penile lengthening surgery with graft reconstruction is ideal for patients with severe penile length loss, significant curvature, and/or prominent hour-glass deformities, but without underlying ED. The graft is applied to the defect following incision of the most prominent point of the convex penis, usually where the Peyronie plaque resides, thereby achieving penile lengthening. Historically, total plaque excision was designed to ‘remove the diseased tunica’, but this invariably leads to a higher postoperative ED rate. Plaque incision or partial excision is now the preferred technique, instead of plaque excision, to avoid compromising the underlying veno-occlusive mechanism while removing sufficient calcified plaque so that grafting is possible [1213]. The surgical technique for graft surgery is generally uniform, and medial or lateral dissection of the NVB may be preferred depending on the plaque location, as a complete dissection of the plaque attachment to the NVB is vital to prevent the recurrence of curvature. The graft material is positioned following plaque incision and is sutured to the edges of the TA to restore tunical tissue integrity. Three major incision techniques have been described in the literature: the double-Y technique, the H-shape technique, and, more recently, the Egydio technique [1]. Whereas the double-Y incision is performed by widening the bifurcation angle of double-Ys, the H-shape technique involves the use of a single, almost complete circumferential-relaxing incision applying geometrical principles. The Egydio technique comprises 4 tripod-shaped forks of 120°, producing a simpler configuration of the tunical defect, which supposedly enables easy suturing of the graft during the procedure [14]. While controversy remains as to which surgical technique is superior, a recent theoretical study analysing these 3 techniques reported that a modified double-Y incision was likely associated with fewer complications and better geometry [15].
Three types of graft materials have been described: autologous grafts, allografts (or xenografts), and synthetic grafts. The use of synthetic materials, including polyester and polytetrafluoroethylene, has largely been abandoned due to higher risks of infection, tissue fibrosis (secondary graft inflammation), graft contracture (due to the inelasticity of the synthetic material), and allergic reactions [1617]. An ideal graft material should be readily available, does not contract, is inexpensive, is resistant to infection, and is able to preserve erectile function. The choice of graft material is likely to be determined by the surgeon's experience, the patient's preference, and the availability of graft material [1]. Since a single ideal graft material has not been established and there is great variation in clinical outcomes, the surgeon's experience, the availability of materials, and features of the patient and the disease play an equally important role in the type of surgical procedure and the choice of a graft material. Advances in technology have resulted in better allograft materials with comparable outcomes to those of autografts [18]. However, the risk of graft contracture remains a concern, as it may lead to future penile curvature and a long-term risk of ED [19].
For men who have poor-quality erections and/or do not respond adequately to pharmacological or vacuum therapy for their ED, a PPI is recommended at the time of penile reconstructive surgery [20]. It is accepted that inflatable PPIs are associated with higher functional satisfaction and lower persistent curvature rates than malleable implants [2021]. In patients with mild curvature (less than 30°), a PPI alone may result in satisfactory straightening of the penis. However, for men with considerable residual penile curvature (greater than 30°) following the placement of a PPI, other options, such as manual modelling, penile plication, and/or plaque incision with or without grafting, should be undertaken at the time of surgery [2122]. Manual penile modelling can be performed with the prosthesis fully inflated by bending the penile prosthesis in the contralateral direction to the curvature for a short period of time (e.g., 30–60 seconds). The tubing between the pump and the cylinders should be occluded with rubber-shod haemostats to protect the pump from high-pressure damage [21]. In addition, when performing the modelling process, excessive pressure on the glans penis should be avoided to prevent urethral erosion by the cylinder tip. An alternative approach is to pre-place plication sutures using the 16-dot method before implanting the prosthesis and then tying them down to correct the curvature [23]. A residual curvature of less than 30° will often improve over time since the prosthesis will act as an internal tissue expander to correct the deformity in the coming months. However, if there is a substantial residual curvature or persistent hour-glass deformity, then releasing incisions can be made on the concave (or abnormal) side and graft patching is recommended, especially if there is a tunical defect greater than 2 cm (in any dimension), to avoid recurrence of penile curvature or herniation of the prosthesis cylinders [20].
Novel surgical techniques to improve penile lengthening and girth at the time of PPI placement with or without concurrent grafting have been described, such as circumferential incision [24], the double dorsalventral approach sliding technique [25], the modified sliding technique (MoST) [2627], and the multiple slice technique (MuST) [28]. The circumferential incision technique involves a circumferential incision at the point of maximal curvature of the tunica with mobilisation of the NVB, whereas the Egydio technique allows partial circumferential incision if the length is limited by the NVB [24]. In the sliding technique [25], both the NVB and urethra are mobilised, with 2 longitudinal incisions made in the lateral aspect of the TA of each corpus cavernosum and joined by hemi-circular incisions (the proximal hemi-circular incision connects dorsally and the distal connects ventrally), for complete transection of the corpora to stretch the penis to its maximum corrected length. The MoST technique is a modification of the sliding technique, with the major notable difference being the use of a single subcoronal incision with mobilisation and utilisation of the Buck's fascia to cover the defects in the TA, obviating the need for graft material [26], whereas MuST is a modification of MoST with multiple pairs of hemi-circumferential incisions enabling multiple sliding sections [28]. The average erect penile length gain achieved in patients who received circumferential incision was found to be around 2.5 to 3 cm, while for men who underwent sliding and various modified of sliding techniques, such as MoST or MuST, the penile length gain was reported to be between 2.5 and 4 cm [28].
2. Clinical outcomes
While penile reconstructive surgery remains the standard of care for many men with PD, it is not without significant risks, and many of them may be permanent [1]. Several factors, such as the severity and the site of curvature, the type of plaque incision, the patient's age and medical comorbidities, and preoperative erectile function, are key determinants of postoperative ED risk [2930].
Penile plication surgery invariably results in penile shortening and requires an adequate preoperative assessment to ensure that patients have adequate penile length and no associated destabilizing penile deformity. Studies evaluating the clinical outcomes following the Nesbit procedure showed high success rates of penile straightening (79%–100%) and overall patient satisfaction (67%–100%) [6313233]. The estimated stretched penile length loss has been reported to be up to 3 cm in some series [63132]. The reported patient satisfaction rates after the Yachia procedure were similarly high (72%–100%) [3435]. While plication surgery is often thought to preserve erectile function, mobilisation of the neurovascular bundle (NVB) and disruption of cavernosal integrity can result in the loss of penile tactile sensation (24%) and ED (12%) [1011].
The saphenous vein is probably the most commonly utilised autologous graft material owing to its ease and reliability of harvesting, large surface area, good compliance, and easy tissue perfusion [363738]. Furthermore, it has been hypothesized that the nitric oxide secreted from the endothelium may prevent haematoma formation and improve erectile function [39]. However, in an animal model, buccal mucosa tissue appeared to perform better than vein tissue, dermis, aponeurosis, and peritoneum in terms of tissue elasticity, lengthening, and morphological properties of the graft, which was likely due to its rich vascular blood supply providing good graft nourishment [40]. Although previous studies have reported high functional and anatomical success rates in autologous grafts [4142], complications such as, de novo ED, penile length loss, and persistent and/or recurrent curvature are not uncommon, especially in the longer term [43]. Furthermore, harvest site complications such as wound haematoma and contracture, altered sensation, and potential inclusion cysts requiring secondary surgery are likewise not uncommon.
The mid-term outcomes of allograft surgery are similar to those of autologous grafts, but with the perceived advantages of a shorter operation time and no harvest-site-associated complications [1]. While short-term data on various allograft materials, such as dermal, cadaveric fascia lata, and 4-layered small intestinal submucosa grafts showed relatively low complication rates [4445], long-term data highlighted the increasing prevalence of issues related to graft reconstruction, such as subsequent penile length loss (22%), recurrence of curvature (up to 80%), glans hypoesthesia (17%), and postoperative ED (67%) [19]. Due to the inadvertent operative risk of diminished rigidity, men with suboptimal preoperative penile erection should avoid grafting surgery and/or be prepared to undergo subsequent PPI placement [46].
The reported risk of urethral injury at the time of penile remodelling following PPI placement is relatively low, if remodelling is done in a controlled manner (i.e., over 30 to 60 seconds with the tubing between the pump and the cylinders occluded with rubber-shod hemostats) [2147]. Published studies comparing the clinical outcomes and patient satisfaction rates between the 2 major penile prostheses showed no significant difference in mechanical survival, that both PPIs provided similar penile strengthening, and that most patients would undergo the same operation again [21].
It has been reported that up to 20% of patients reported diminished glans sensitivity following PPI placement, likely related to mobilisation of the NVB coupled with various lengthening strategies [28]. In addition, penile haematoma (up to 25%) and graft retraction (up to 10%) with residual curvature are not uncommon [2428]. Serious complications such as glans necrosis (2%) can occur due to compromised glans vascularity, and the ensuing glanular loss is often associated with cardiovascular disease, diabetes, smoking, previous prosthesis explantation, and previous radiation [2848]. In addition, the risk of prosthetic infection and explantation should not be underestimated in this cohort of patients, with prosthesis infection reported in 7% of cases due to a longer operative time and concurrent use of graft material.
Go to :
CONCLUSIONS
Despite published recommendations and the guidelines of international organisations [123], there is a lack of consensus among surgeons on the optimal management strategies for PD. Among the challenges facing clinicians is the lack of strong evidence-based reports defining the utility of preoperative testing, the optimal timing of interventions, the type of intervention, and the physical and psychological characteristics of the ideal patient. Many men with PD are often depressed, have a marked reduction of self-esteem, and at times have unattainable expectations regarding the outcomes of surgical reconstruction [4950]. While surgical approaches remain the standard of care, they pose considerable risks, including neuropraxia with sensory numbness and ED, as well as recurrent or residual penile curvature and the need for prolonged postoperative rehabilitation [1].
In summary, the major advantages of plication procedures are that they are simple and minimally invasive and tend to preserve potency in most patients. The disadvantages of plication procedures include penile length loss and the fact that they do not address or may, in fact, worsen a pre-existing hour-glass or hinge effect, particularly if larger plications are used. In contrast, graft reconstructive surgery can address issues relating to the loss of penile length and complex penile deformities (e.g., hour-glass deformities), but long-term data highlight the risks of altered glans sensation, recurrence of curvature, and/or loss of penile length from graft contracture, as well as the development of ED due to the underlying progression of arteriogenic or veno-occlusive dysfunction [5152]. Complex penile reconstruction with the concurrent placement of a PPI to address ED is a demanding operation and should be performed by surgeons with extensive prosthetic and reconstructive experience, as the risk of sensory loss, glans ischemia/necrosis, prosthesis-related complications, and failure to gain any meaningful length are serious concerns and cannot be underestimated.
At present, there is a paucity of literature regarding the decision to reoperate or to perform revision surgery in cases of persistent and/or recurrent penile curvature. It is generally agreed that revision surgery should be postponed until at least 6 months postoperatively to allow for normal healing to occur and to assess whether a new deformity or ED develops [1]. During this period, it is advisable that patients undergo various conservative penile rehabilitative measures to correct any residual penile curvature, such as penile traction therapy [53], or pro-erectile agents to facilitate the return of penile erection [54]. In men who undergo graft surgery, postoperative penile rehabilitation is generally recommended to enhance the recovery of erectile function. Proposed penile rehabilitation protocols include penile massage and stretch therapy, the use of erectogenic medications, and traction therapy [3055]. Adjuvant surgical therapy such as suspensory ligament release with or without a silicone buffer, suprapubic lipectomy, and ventral phalloplasty may be used to increase perceived or enhanced actual penile length to provide higher patient satisfaction and improved cosmetic outcomes for men undergoing a surgical intervention for PD [28].
The most critical part of the surgeon's role in the preoperative stage is to set appropriate expectations for the patient and to obtain adequate informed consent regarding the potential surgical complications. Obtaining proper informed consent and establishing realistic outcome expectations are imperative for successful postoperative outcomes, and the risks of persistent or recurrent curvature, penile length loss, ED, and/or reduced sexual sensation should be discussed with the patient and his partner.
Go to :
 XML Download
XML Download