

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hydroxyapatite (HAp; Ca10[PO4]6[OH]2) has long been used for the reconstruction of bony defects in orthopedic surgery and in the field of dentistry [12]. HAp shows excellent biocompatibility and osteoconductivity, but a limitation of its use in bony defect reconstruction is that the material remains stable in the bone as a foreign body. HAp is poorly resorbed in vivo, and it can become a source of infection [345]. Although bone apatite is generally thought to be composed of HAp, in fact, human bone is not stoichiometric HAp; instead, it is carbonate apatite (CO3Ap; Ca10−a[PO4]6−b[CO3]c[OH]2−d), which contains 6%–9% by weight of carbonate in its apatite crystal structure [6]. Since CO3Ap is more soluble in acidic solution than HAp, CO3Ap is easily resorbed by osteoclasts [78]. Doi et al. [9] used a sintering method to fabricate a CO3Ap block. This sintered CO3Ap block contained up to 6% by weight of carbonate in its apatitic structure. Ishikawa et al. succeeded in fabricating low-crystalline CO3Ap without a sintering step by utilizing a dissolution-precipitation reaction involving precursors such as low-crystalline calcite [10]. In their study, since the CO3Ap block was fabricated in the aqueous solution, it contained larger amounts of carbonate in its apatitic structure than the block that was fabricated using a sintering method, and its crystallinity was also similar to that of bone. It was also shown that CO3Ap upregulated the osteoblastic differentiation of human bone marrow cells earlier than sintered HAp [11]. CO3Ap showed faster bone formation than Bio-Oss® (Geistlich‐Pharma, Wolhusen, Switzerland) in a rabbit femur [12]. Taking into account these results, it is evident that CO3Ap possesses higher osteoinductivity than sintered HAp or BioOss®, and CO3Ap may be a superior bone substitute material and scaffold for bone regeneration than those alternatives. This evidence encouraged us to use CO3Ap granules in the treatment of human bone defects. Kudoh et al. previously reported the safety and efficacy of CO3Ap granules in single-stage sinus floor augmentation for cases in which the residual alveolar bone height was between 3.7 and 6.0 mm [13]. The limitation of their study was that only radiographic images were evaluated, and no histomorphometric evaluations were performed. Therefore, little was determined about the resorption behavior and tissue response of CO3Ap in the human body.
The purpose of this study is to clarify the safety and efficacy of CO3Ap granules in sinus floor augmentation for a severely atrophic maxilla with a residual alveolar bone height in the range of 1.0–5.0 mm, with delayed implant placement. This study is the first histological evaluation of low-crystalline CO3Ap granules using bone biopsy specimens in humans.
MATERIALS AND METHODS
Patient selection
A multicenter single-arm prospective study was conducted at 3 university dental hospitals: 1) the Department of Oral Surgery, Tokushima University Hospital, 2) the Dental Implant Clinic, Dental Hospital, Tokyo Medical and Dental University, and 3) the Rehabilitative Dentistry and Implant Center, Kyushu University Hospital. Since no bone substitutes are approved in Japan for use at implant placement sites, other bone substitutes could not be used as a control. The clinical trial, including the recruitment of patients, was performed from January 16, 2015 to May 16, 2017.
The study population was composed of patients who had been treated with implant surgery using a 2-stage sinus floor augmentation procedure on the maxillary posterior of the edentulous region. In the study, 13 patients (4 male and 9 female) between the ages of 37 and 77 years (mean age, 61.0±11.7 years) were selected according to the inclusion and exclusion criteria shown in Table 1.
Table 1
Inclusion and exclusion criteria for patients

This trial was conducted in accordance with the Good Clinical Practice Guidelines and the Declaration of Helsinki, and the protocol was reviewed and approved by the Institutional Review Board (approval No. 1993) of each hospital involved in the study. All participants provided informed consent in writing, and the trial was registered as JPRN-UMIN000019281 in the University Hospital Medical Information Network in Japan and with the International Clinical Trials Registry Platform Search Portal of the World Health Organization.
Graft material
In this clinical trial, CO3Ap granules (code no. GCAP-01) were provided by GC Corporation (Tokyo, Japan). The particle size of CO3Ap was in the range of 600–1,000 µm (short diameter).
The method used to fabricate low-crystalline CO3Ap consists of 2 processes. First, a precursor block is fabricated. For example, calcite block, which is used as a precursor, is fabricated by exposing calcium hydroxide compact to CO2 [14]. The calcite block thus prepared cannot be washed out even when the block is immersed in an aqueous solution. Next, the precursor block is then immersed in a phosphate salt solution. As CO3Ap is the most stable phase thermodynamically at neutral and alkaline pH, the calcite block is transformed into a low crystalline CO3Ap that maintains its macroscopic structure based on the dissolution–precipitation reaction. This low crystalline CO3Ap was found to upregulate differentiation of osteoblasts, and it was resorbed by osteoclasts [59], because CO3Ap was closer in chemical composition to bone mineral.
Two-stage sinus floor augmentation technique and bone biopsy
Local anesthesia was administered, and a horizontal incision was made along the alveolar crest in the edentulous site. Then, vertical incisions were made to elevate the mucoperiosteal flap. After elevation of a full-thickness mucoperiosteal flap, a lateral bony window of the sinus was made by using a small diamond bur, a steel round bur, or a piezosurgical unit (Piezosurgery®, Mectron Medical Technology, Carasco, Italy). The sinus floor membrane was separated from the floor of the sinus and carefully elevated with a mucosal elevator. We checked carefully for any perforation of the membrane. After the sinus floor membrane was elevated, CO3Ap granules were packed into the elevated space. Finally, the mucoperiosteal flap was repositioned and sutured. The patients were given prophylactic antibiotics after augmentation, and they were brought back in 7–10 days later for clinical evaluation and removal of the sutures. Implant placement was planned for 8±2 months after augmentation. Prior to implant hole preparation, a bone biopsy specimen was taken from the same site using a trephine bur (2.1 mm in diameter). The implant was placed according to the standard protocol from the respective implant manufacturer. Implant installation torque was measured using a drilling device (GC Implant Motor IM-III, GC Corporation). Figure 1 shows the treatment protocol for this clinical study and the time schedule of the evaluations using panoramic radiographs.
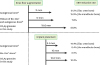
Figure 1
Treatment protocol (upper section) and time schedule of evaluations using panoramic radiographs (lower section). Panoramic radiographs were taken i) pre-sinus floor augmentation, ii) immediately after augmentation, iii) 7±2 months after augmentation, and iv) 18±2 months after augmentation.
CO3Ap: carbonate apatite.

Radiographic examinations
Computed tomography (CT) examinations were performed before and 7±2 months after sinus floor augmentation to evaluate the morphology and the height of the alveolar bone. Panoramic radiographs were taken, and the height of the augmented site containing the alveolar bone and CO3Ap granules was measured at the following points:
i) First measurement: preoperative (within 4 months prior to sinus floor augmentation); ii) Second measurement: immediately after augmentation; iii) Third measurement: 7±2 months after augmentation (within 1 month prior to implant placement); and iv) Fourth measurement: 18±2 months after augmentation.
The alveolar bone crest line, original sinus floor line, and grafted sinus floor line were traced by superimposition of the panoramic images (Figure 2). Elevated bone height (EBH), which represents the distance from the alveolar bone crest line to the CO3Ap-grafted sinus floor line, was measured at the planned implant placement site. The panoramic images were saved as Digital Imaging and Communications in Medicine files, and digital radiographs were then analyzed using the Osiris medical imaging software program (Open-Source, OsiriX Medical Imaging Software, http://www.osirix-viewer.com).

Histological examinations
Biopsy specimens were fixed in 10% buffered formalin and dehydrated in a graded alcohol series. Specimens were then embedded in a methyl methacrylate resin. Next, undecalcified sections were cut into 4-µm-thick sections using a microtome. The sections were stained with hematoxylin and eosin and Villanueva-Goldner stains using standard techniques. The area of new bone or residual CO3Ap granules was measured on the histological sections using Image J software (National Institutes of Health, Bethesda, MD, USA), and the ratio of the area of new bone or residual CO3Ap granules to total specimen area was also calculated for each specimen.
Micro-CT (TOSCANER-30000mhd micro-CT scanner, Toshiba, Tokyo, Japan) scans of the bone biopsy specimens were obtained and stored using 3D Creator software (VG Studio MAX, Volume Graphics, Heidelberg, Germany).
Statistical analysis
The data were classified according to the values obtained from the radiographs and treatment records, and the means and standard deviations were calculated. Statistical analysis was performed using the Wilcoxon signed-rank test using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). Differences were considered statistically significant at P<0.01.
RESULTS
Table 2 summarizes the patients, implants (length, diameter, and installation torque), and amount of CO3Ap granules used. The amount of CO3Ap used in each case was between 0.4–2.5 cm3 (1.3±0.6 cm3). No perforation of the sinus membranes occurred during the augmentation. In all cases, the postoperative healing of the augmentation was uneventful, with no abnormal bleeding, pain, or swelling due to the CO3Ap granules. At 8±2 months after augmentation, it was possible to place 17 implants with lengths of 6.5–11.5 mm. The implant installation torque ranged from 12.0 to 50.0 Ncm, and the mean value was 25.1±13.2 Ncm. All implants achieved osseointegration.
Table 2
Description of patients, implants (length, diameter, and installation torque), and the amount of CO3Ap granules used

Table 3 and Figure 3 show the changes in the mean EBH. Preoperative residual bone height in the molar region of the maxilla ranged from 1.0 to 5.0 mm, and the mean height was 3.5±1.3 mm. The mean EBH increased to 13.3±1.7 mm immediately after augmentation with the CO3Ap granules, then decreased to 10.7±1.9 mm and 9.6±1.4 mm at 7±2 months and 18±2 months after augmentation, respectively. The mean EBH at 7±2 months after augmentation was 19.5% lower than that immediately after augmentation, and the difference was significant (P<0.01). The EBH at 18±2 months after sinus floor augmentation had decreased from that at 7±2 months after augmentation, and this decrease was statistically significant (P<0.01).
Table 3
Bone height at implant placement site
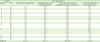
Figure 3
EBH at the implant placement site. Statistically significant differences were observed in comparison to the EBH measured immediately after the augmentation.
EBH: elevated bone height.
a)P<0.01.

Clinically, no abnormal bone resorption was observed for the sites augmented with CO3Ap granules, and a bone height that could support implants was maintained. No implant failures or complications were observed up to 18±2 months after augmentation. Furthermore, no postoperative infection, redness, or persistent pain, such as pain due to an allergic reaction, was observed at the augmented sites under consideration. Therefore, the overall survival rate of the implants was 100% at approximately 31 months after implant placement.
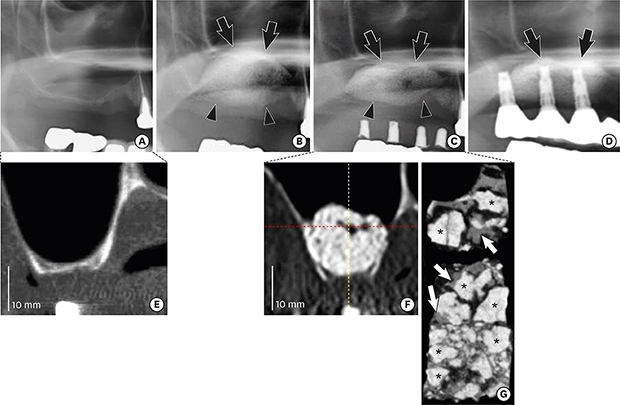
Figure 4 shows surgical views of the maxillary sinus floor augmentation and implant placement in case 10. In this case, the preoperative residual bone heights of the planned implant placement sites (#15, 16, and 17) were 3.0, 1.4, and 1.0 mm, respectively (Figure 5A and E). CO3Ap granules (Figure 4A) were filled into the elevated space immediately after augmentation (Figure 4B and C). The EBH increased to 14.0, 17.0, and 15.0 mm at sites #15, 16, and 17, respectively. At implant placement, 8 months after augmentation, some CO3Ap granules were observed on the surface of the augmented site (Figure 4D). New bone had formed around the CO3Ap granules and was combined with them. Although the EBH had decreased from 14.0 to 10.9 mm at site #15, from 17.0 to 11.5 mm at site #16, and from 15.0 to 10.3 mm at site #17 by 7 months after augmentation, an implant with a length of 10.0 mm could be placed into sites #15 and #16, and an implant with a length of 8.0 mm could be placed into site #17 (Figure 4D). By 18 months after augmentation, the EBH had decreased to 10.0 mm at sites #15 and 16 and to 8.3 mm at site #17. From the panoramic radiographs (Figure 5B, C, and D), the boundary line between the residual bone and the CO3Ap granules could be detected immediately after augmentation (see arrowheads in Figure 5B); however, it gradually became obscure and could no longer be detected at 18 months post-augmentation (Figure 5D). Figure 5E and F show CT images of the CO3Ap-grafted site before and 7 months after augmentation, respectively. Residual CO3Ap granules were observed as high-density areas in contact with the new bone. Figure 5g shows a micro-CT image of a bone biopsy specimen at 7 months after augmentation. The residual CO3Ap granules were in direct contact with the new bone without the presence of intermediate soft tissue.
Figure 4
Graft material and surgical views of maxillary sinus floor augmentation and implant placement (case 10). (A) The CO3Ap granules used in this clinical trial. (B) Preparation of the recipient site of the elevated space. (C) The elevated space filled with CO3Ap granules. (D) Implant placement observed 8 months after augmentation.
CO3Ap: carbonate apatite.

Figure 5
Radiographic examinations (case 10). Panoramic radiographs taken (A) pre-augmentation, (B) immediately after augmentation, (C) 7 months after augmentation, and (D) 18 months after augmentation. Arrowheads indicate the boundary line between residual bone and CO3Ap granules (B, C). Black arrows indicate the grafted sinus floor line, which is elevated by augmentation with CO3Ap granules (B-D). CT images of preoperative residual bone height at site #16 (1.4 mm) (E) and the elevated bone height at 7 months after augmentation of the same site (17.0 mm) (F). The bone height was maintained until implant placement. A micro-CT image of the bone biopsy sample taken 8 months after augmentation (G). Newly formed bone (white arrows) in direct contact with CO3Ap granules (*).
CO3Ap: carbonate apatite, CT: computed tomography.

The images in Figure 6 show bone biopsy sections from case 8 at 7 months after augmentation. The amounts of new bone and residual CO3Ap were 43.8% and 13.2%, respectively (Figure 6A). Few inflammatory cells or foreign body giant cells were observed around the CO3Ap granules (Figure 6B). New bone and CO3Ap granules were in direct contact with each other without any intermediate fibrous tissue (Figure 6C), and the CO3Ap granules were in the process of being replaced by new bone (Figure 6D). In the indicated area of Figure 6d, osteoblasts were observed on the surface of the CO3Ap granules (Figure 6E). In the serial section, using Villanueva-Goldner stain, it was observed that new bone (red) was gradually being replaced with mature bone (green) (Figure 6F).
Figure 6
A histological microphotograph of case 8 taken 7 months after augmentation. (A) A lower-magnification image of the relevant section of the biopsy specimen. The amounts of NB and residual CO3Ap (*) were 43.8% and 13.2%, respectively. (B) Few inflammatory cells or foreign body giant cells were observed around the CO3Ap granules (*). (C) New bone was observed to be in direct contact with the CO3Ap granules (*) with no intermediate fibrous tissue. (D) Black arrowheads indicate the area of replacement of CO3Ap granules (*) with new bone. (E) A higher-magnification image. Arrows indicate that osteoblasts were observed on the surface of new bone. Asterisk indicates residual CO3Ap. (F) The serial section of Figure 6E (visualized with Villanueva-Goldner stain). Mature bone was stained in green, and new bone was stained in red. New bone was gradually being replaced with mature bone (white arrowheads).
NB: new bone, CO3Ap: carbonate apatite.

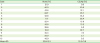
Table 4 shows the amounts of new bone and residual CO3Ap in biopsy specimens subjected to histological evaluation. Bone formation was observed in all cases; the amount of new bone ranged from 11.7% to 63.7%, and the amount of residual CO3Ap ranged from 0.0% to 35.3%, with individual variations among the cases. The mean amounts of new bone and CO3Ap were 33.8%±15.1% and 15.3%±11.9%, respectively.
Table 4
The amount (%) of bone and residual CO3Ap obtained by histomorphometric evaluation in all cases
DISCUSSION
Bone biopsy examination revealed few inflammatory cells or foreign body giant cells, and new bone had formed around the residual CO3Ap granules in all cases. The CO3Ap granules were in direct contact with the new bone, with no intermediate fibrous tissue. The results obtained in this study clearly demonstrate the excellent biocompatibility and osteoconductivity of low-crystalline CO3Ap granules in humans, indicating that CO3Ap granules are a safe and useful bone substitute in two-stage sinus floor augmentation.
Implant insertion torque value, or installation torque value, has been a significant clinical indicator of primary implant stability and superior long-term implant survival rates [1516]. Johansson et al. [17] reported that implant insertion torque values for failed implants were lower than the corresponding values for surviving stable implants. In our study, the installation torque values ranged from 12.0 to 50.0 Ncm (25.1±13.2 Ncm), and the values varied widely. No relationship was observed between the installation torque value and either the ratio of newly formed bone or the height of residual bone (data not shown). Dos Anjos et al. [18] performed implant placement 8 months after sinus floor augmentation with Bio-Oss® and measured the installation torque. Their data indicated that all implants placed in the maxillary sinus presented higher installation torque values (35.0±9.8 Ncm) than those present in our results. However, installation torque value has been found to be affected by implant design and surgical technique. O'Sullivan et al. [19] measured the installation torque values of different implant designs in the maxillary bone of human cadavers, and the Brånemark Mark IV tapered implant showed a significantly higher installation torque than did the straight implants under study, including the Brånemark Standard implant, the Mark II implant, and the Osseotite implant. Tabassum et al. [20] demonstrated that implants placed with the undersized surgical technique showed higher installation torque values than those placed with the press-fit technique. Although the installation torque values from Dos Anjos's report were higher than those in our study, it is worth noting that they used tapered implants in all cases. In contrast, we used several kinds of implants, because multiple institutions were involved in the trial. Therefore, the variation in the installation torque values that we observed could very well be due to the variety of implant designs and surgical techniques used. In our study, all implants achieved osseointegration, and the overall survival rate at about 31 months after implant placement was 100%.
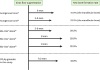
Figure 7 summarizes the reports of EBH reduction after 2-stage sinus floor augmentation using various bone substitutes. Deppe et al. [21] performed sinus floor augmentation solely with autogenous cortical bone obtained from the iliac crest or the mandible. The EBH reduction rates for the autogenous cortical bone graft at 11 months after augmentation were 21.5% in the iliac crest group and 15.9% in the mandibular bone group. Kim et al. [22] performed sinus floor augmentation with a mixture of Bio-Oss® and a small amount of autogenous cortical bone. EBH reduction from immediately after augmentation to 1 year after augmentation was 7.8%. In our study, EBH reduction at 18±2 months after augmentation was 27.8%. Taking into account these results, we conclude that the order of resorption speed after augmentation for the graft materials was, from fastest to slowest, autogenous cortical bone, then CO3Ap granules, and then Bio-Oss®.
Figure 7
EBH reduction rates in 2-stage sinus floor augmentation using various bone substitutes after sinus floor augmentation or implant placement.
EBH: elevated bone height, CO3Ap: carbonate apatite.
Regarding the changes in EBH after implant placement, Deppe et al. [21] showed that EBH reduction for autogenous cortical bone grafts was 14.4% in the iliac crest group and 8.4% in the mandible group at 5.5 months after implant placement, where the EBH at the time of implant placement was assumed to be 100%. Hieu et al. [23] performed sinus floor augmentation with Bio-Oss® alone. EBH reduction at 10 months after implant placement was 6.5% compared to EBH reduction of 10.3% at 10±2 months after implant placement in our study. Therefore, the pace of EBH reduction after implant placement of CO3Ap granules was almost equal to that of autogenous cortical bone and faster than that of Bio-Oss®.
Figure 8 summarizes the reports on the rate of new bone formation in biopsy specimens from histological evaluation after sinus floor augmentation with autogenous bone and Bio-Oss®. Zerbo et al. [24] performed histomorphometric analysis and evaluated new bone formation after augmentation with autogenous cortical bone alone. The graft bone was harvested from the mandible, bone biopsy was performed at 6 months after augmentation, and the rate of new bone formation was 41.0%±10.0%. John and Wenz [25] performed histomorphometric analyses on bone biopsies harvested at 3 to 8 months after augmentation using mandibular bone alone. They reported that the bone formation rate for the mandibular bone was 53.5%±2.5%. It has been proposed that the rate of new bone formation from autogenous cortical bone alone is approximately 40%–50%. New bone formation rates for Bio-Oss® were reported by John and Wenz [25], Sartori et al. [26], and Tadjoedin et al. [27] to be 29.5%±7.4%, 29.8%±2.6%, and 22.9%±2.5%, respectively. Based on these reports, the rate of new bone formation with Bio-Oss® is approximately 20%–30%. In our study, the amount of new bone at 7±2 months after augmentation was 33.8%±15.1%. A comparison with other graft materials, such as autogenous cortical bone and Bio-Oss®, was not performed in this study. However, Fujisawa et al. [12] demonstrated that a significantly larger amount of new bone formation was elicited in the cortical portion of a bone defect in a rabbit femur when reconstructed with CO3Ap granules than with Bio-Oss® at 8 weeks after implantation. Therefore, we surmise that the rate of new bone formation for CO3Ap granules is higher than that for Bio-Oss®.
Figure 8
New bone formation rates in biopsy specimens from histological evaluation after sinus floor augmentation using autogenous bone, Bio-Oss®, CO3Ap granules.
CO3Ap: carbonate apatite.
John and Wenz [25] reported that the bone formation rate of a 2:1 mixture of Bio-Oss® and mandibular bone was 32.2%±6.9%. Tadjoedin et al. [27] demonstrated a relationship between the rate of new bone formation and the ratio of Bio-Oss® to autogenous cortical bone. The bone formation rates for 20%, 50%, 80%, and 100% Bio-Oss® were 37.3%±4.4%, 33.6%±2.7%, 24.7%±2.4%, and 22.9%±2.5%, respectively. This revealed that the bone formation rate was inversely correlated with the amount of Bio-Oss®. These studies demonstrated that the rate of new bone formation for a combination of Bio-Oss® and autogenous cortical bone was approximately 24%–37%. In the same manner, adding autogenous cortical bone to CO3Ap granules would be expected to increase the rate of new bone formation compared to using CO3Ap granules alone.
Hallman et al. [28] and John and Wenz [25] performed sinus floor augmentation with Bio-Oss® and reported the amounts of residual Bio-Oss® at implant placement to be 11.8%±3.6% and 14.9%±6.5%, respectively. In our study, the amount of residual CO3Ap granules at 7±2 months after augmentation was 15.3%±11.9%, and the values varied widely. Fujisawa et al. [12] showed that the CO3Ap granules became smaller in size over time, and they also showed that the resorption speed for CO3Ap granules was faster than that for Bio-Oss® at 8 weeks after implantation, where implantation was made to a bony defect of a rabbit femur. Therefore, it is reasonable to expect that resorption of CO3Ap granules would also be faster than that of Bio-Oss® even in humans.
Galindo-Moreno et al. [29] and Moy et al. [30] reported the results of a histomorphometric study of bone biopsy specimens augmented with Bio-Oss® and HAp, respectively. Inflammatory cells and foreign body giant cells were rarely observed in the bone biopsy specimens of these materials. The new bone was in direct contact with the augmentation materials, without an intermediate layer of fibrous tissue. Bone biopsy of the CO3Ap granules showed similar findings (Figure 5), and these results indicate that CO3Ap granules possess excellent biocompatibility, like Bio-Oss® and HAp.
Although Bio-Oss® is widely used as a viable bone substitute, it is derived from a bovine source. Therefore, Bio-Oss® carries some risk of transmission of infectious diseases, such as bovine spongiform encephalopathy, via prions from cows to humans [31]. Moreover, there remains a possibility of the transmission of new infectious diseases stemming from unknown pathogens. Since Bio-Oss® is a natural material, there are also slight differences in stability and composition across product lots. In contrast, CO3Ap granules are a completely artificial synthetic bone substitute; therefore, they have never contained any pathogens, including prions, and they offer stable properties with no variation across product lots.
In conclusion, this study is the first in-human demonstration of the behavior of low-crystalline CO3Ap granules from bone biopsy specimens. The results of this clinical study suggest that low-crystalline CO3Ap is a safe and beneficial bone substitute in two-stage sinus floor augmentation. Radiographic and histological examination of the bone biopsy specimens suggest that CO3Ap granules possess excellent biocompatibility without any risk of allergic reaction or immunological rejection, and they achieve adequate EBH for implant placement. In all cases, the postoperative recovery from augmentation with CO3Ap granules was uneventful. All implants achieved osseointegration and clinically showed no mobility at 31 months after implant placement. However, further study with a larger sample size and long-term follow-up with patients is needed for a more thorough evaluation.
 XML Download
XML Download