

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The use of titanium dental implants has improved with respect to rapid osseointegration and prosthetic loading, as well as an increased implant success rate. In particular, modifications to the surface of implants has played a major role in these improvements [123456]. Topographical and chemical modifications of the implant surface have been shown to improve hydrophilicity and bone-implant contact [5789]. Sandblasted, large-grit, acid-etched (SLA) implant surfaces, which have both a microstructure and a macrostructure, have shown good clinical results in previous studies [1247].
Furthermore, chemical modifications of SLA surfaces have been developed. SLActive (Straumann, Basel, Switzerland) consists of SLA implant surface that has been submerged in an isotonic sodium chloride solution to prevent carbon contamination from the atmosphere. According to a previous study, this surface is thought to promote early-stage bone formation [10]. A chemically activated, calcium-modified SLA surface has also been developed (Osstem Implant Co., Ltd., Busan, Korea); this surface is submerged in a calcium chloride solution instead of a sodium chloride solution. This calcium-modified surface showed similar bone-implant contact to that of the SLActive surface in a recent study using a rabbit model [11].
Interactions with blood cells and molecules on the implant surface could impact surface properties [12]. Proteins such as growth and differentiation factors are attracted to hydrophilic implant surfaces. In many studies, the biochemical characteristics of the implant surface, such as cell viability, proliferation, attachment, and differentiation, were tested through in vitro experiments using cells or cytokines, and these properties were found to influence cellular activities [121314].
Formation of a sufficient fibrin clot offers a direct and stable link at the bone-to-implant interface; therefore, it plays an important role in thrombogenic responses and osseointegration [15]. When the fibrin clots on different implant surfaces were observed, a relationship was found between the implant surface and the extent of the fibrin clot [16].
In the process of drilling prior to implant placement, bone tissue undergoes trauma similar to a fracture. The site becomes relatively hypoxic, and the extracellular pH becomes acidic. In acidic conditions, the bone marrow stromal cells exhibit low alkaline phosphatase (ALP) activity and low collagen synthesis, 2 factors that are important in bone formation [17]. It has been reported that ALP activity decreased from a peak at a pH of 7.4 to almost zero below a pH of 7.0 [18]. Another study found that ALP activity and collagen synthesis, as well as glycolysis and DNA synthesis of osteoblasts, are also affected by acidic conditions [19]. In addition, platelet aggregation was also reduced by extracellular acidosis, as mediated by the calcium ion entry pathway [20].
The novel chemically activated SLA surface that is coated with a pH buffering solution was investigated. This surface is thought to display a high affinity for proteins, cells, and platelets, thereby promoting rapid and stable blood clotting and thrombogenesis. Therefore, the purpose of this study was to evaluate the effectiveness of an SLA surface coated with a pH buffering solution in vitro compared with a conventional SLA surface and a chemically activated calcium-modified SLA surface based on surface wettability, blood protein adhesion, osteoblast affinity, and platelet adhesion and activation.
MATERIALS AND METHODS
Preparation of titanium discs, implants, and reagents
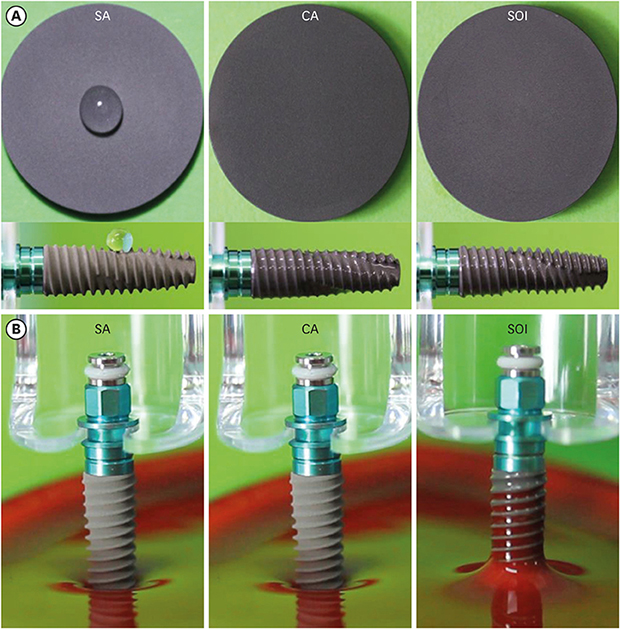
Three types of titanium discs and implants were provided by Osstem Implant Co., Ltd.: 1) a conventional SLA surface (SA, serving as the negative control group), 2) a SLA surface in aqueous calcium chloride solution (CA, serving as the positive control group), and 3) a SLA surface coated with a pH buffering solution (SOI, serving as the test group) (Figure 1A). The Ra values of the surfaces were 2.5±0.5 µm, based on information from the manufacturer. Cell culture plastic wares were purchased from Becton-Dickinson Falcon (Franklin Lakes, NJ, USA). Fetal bovine serum (FBS), trypsin/ethylenediaminetetraacetic acid (EDTA), penicillin and streptomycin, and Dulbecco's modified eagle medium (DMEM) were purchased from HyClone (Salt Lake City, UT, USA), and phosphate-buffered saline (PBS) was obtained from Invitrogen Corporation (Paisley, UK). Alizarin Red S, Triton X-100, p-nitrophenylphosphate (p-NPP), magnesium chloride, and cresyl violet were purchased from Sigma (St. Louis, MO, USA), and 3-(4,5-dimethylthiazol-2-gl)-5-(3-carboxymethoxylphenyl)-2-(4-sulfophenyl-2H)-tetrazolium inner salt (MTS) was obtained from Promega (Madison, WI, USA). Three discs of each titanium surface (SA, CA, and SOI) were utilized for each test.
Figure 1
Surface wettability measurement. (A) Contact angle between a liquid drop and a solid surface. (B) Wetting velocity measurement. After 40 seconds, the SOI surface displayed the most threads wetted by blood. SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in aqueous calcium chloride solution, SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution.

Surface wettability measurement (wetting velocity measurement)
efibrinated sheep blood (MB-S1876; MB Cell, Seoul, Korea) was placed in a dish (diameter, 10 cm) to a depth of 2–3 cm. Implants with SA, CA, and SOI surfaces (diameter, 4.5 mm; length, 13 mm) were immersed into the blood up to 2 mm from the apex (Figure 1B). Nine implants for each surface were tested. The number of threads wetted by blood in 40 seconds was counted for the calculation of the wetting velocity.
Serum albumin adsorption
Bicinchoninic acid assay
Purified bovine serum albumin (BSA, 1 mg/mL, 1 mL) was added to the surfaces of the titanium discs. After incubation at 37°C for 1 hour, the non-adsorbed plasma was washed out. The BSA-treated discs were eluted for 30 minutes using a lysis buffer (0.2% Triton X-100 in PBS, pH 7.4) at 37°C. The supernatants were assayed using comparative bicinchoninic acid (BCA) assays (BCA Protein Assay Kit No. 23227) according to instructions provided by the supplier (Pierce, Rockford, IL, USA). Protein detection was performed at a wavelength of 560 nm using a multimode microplate reader (DTX 880 Multimode Detector, Beckman Coulter GmbH, Krefeld, Germany). Nine titanium discs of each surface were tested.
Fluorescein isothiocyanate (FITC)-labeled BSA
FITC-labeled BSA (Sigma) in PBS was used for the protein adsorption test. Adsorption was measured using fluorescence intensity. FITC-conjugated serum albumin was added in order to examine plasma protein adsorption by the SA, CA, and SOI implants. After incubation, the excess FITC-conjugated serum albumin was washed from the implant surfaces. Three implants of each surface were treated with FITC-conjugated serum albumin, examined using a Typhoon FLA 7000 device (GE Healthcare Life Sciences, Chicago IL, USA), and analyzed using Image J software (National Institute of Health, Bethesda, MD, USA) (Figure 2).
Figure 2
Image depicting FITC-labeled BSA present on each implant surface. The fluorescence intensity of the SOI surface was the strongest, whereas that of the SA surface was the weakest.
FITC: fluorescein isothiocyanate, BSA: bovine serum albumin, SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in aqueous calcium chloride solution, SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution.

Observation for osteoblast morphology
Cell culture (osteoblast culture)
The MG-63 cell line (ATCC, Manassas, VA, USA), established from human osteosarcoma cells, is a non-transformed cell line. These cells were routinely cultured in DMEM with 10% FBS and 0.1 mg/mL of penicillin and streptomycin. The cells were subcultured in trypsin/EDTA twice per week, and the medium was changed every 2 days.
Scanning electron microscopy (SEM)
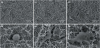
For SEM observations, the MG-63 cells were incubated on the titanium discs and fixed with a 2.5% glutaraldehyde solution. After dehydration, the samples were sputter-coated with Pt-Pd for morphologic examination with SEM (JSM-6480LV, Tokyo, Japan) (Figure 3).
Figure 3
SEM image taken 30 minutes after MG-63 cell incubation on each implant surface. The number of osteoblasts on the CA and SOI surfaces is more prominent than that on the SA surface, and the cells on the CA and SOI surfaces seem to be further differentiated.
SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in calcium chloride aqueous solution, SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution.
Confocal laser scanning microscopy (CLSM; immunofluorescence cell staining)
The cell morphology and cytoskeletal arrangement of osteoblasts were observed with CLSM. MG-63 cells were seeded for 24 hours on the titanium discs and observed using CLSM. The cells were fixed in 4% formalin and permeabilized in 0.1% Triton X-100. The cells were then blocked in 7.5% BSA containing PBS for 1 hour. The fluorescent staining was conducted with vinculin and F-actin using anti-vinculin Alexa Fluor 488 (Bioscience, Allentown, PA, USA) and anti-stain 555 fluorescent phalloidin (Cytoskeleton Inc., Denver, CO, USA), respectively. After incubation overnight at 4°C, the samples were then observed with CLSM (LSM 700, Carl Zeiss, Oberkochen, Germany) (Figure 4).
Figure 4
Confocal laser scanning microscopy (immunofluorescence cell staining) image taken 30 minutes after MG-63 cell incubation on each implant surface. Red indicates phalloidin staining, while green indicates vinculin staining. More bone cells were observed on the CA and SOI surfaces than on the SA surface.
SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in calcium chloride aqueous solution, SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution.

Osteoblast adhesion
With a CellTiter 96® AQueous Non-Radioactive Cell Proliferation Assay kit (Promega), the cell adhesion assay of MG-63 cells was performed according to the manufacturer's instructions. Prior to the cell adhesion assay, the cells were cultured onto either the titanium discs or the plastic material used for culture in 24 multi-well plates (Becton-Dickinson Falcon) at a density of 1×105 cells for 1 hour. Three titanium discs of each surface were tested. After the culture media was removed and washed, 500 µL of MTS/1-methoxy phenazine methosulfate (PMS)/medium mixture was added to each well for 2 hours. Colorimetric measurements of formazan dye were conducted using a DTX 880 device, and the optical density (OD) was read at 490 nm.
Osteoblast proliferation
Using a CellTiter 96® AQueous Non-Radioactive Cell Proliferation Assay kit, the proliferation assay of MG-63 cells was performed according to the manufacturer's instructions. The cells were cultured onto either the titanium discs or the culture plastic. Three titanium discs of each surface were tested. After a period of time, the culture media was removed, and 500 µL of the MTS/PMS/medium mixture was combined into each well for 2 hours. Colorimetric measurements of formazan dye were conducted using a DTX 880 device, and the OD was read at 490 nm.
Osteoblast differentiation (ALP activity)
ALP activity was examined as described in previous studies [21222324], with MG-63 cells cultured onto either the titanium discs or the culture plastic. Three titanium discs of each surface were tested. The osteogenic medium (containing 0.5 µM dexamethasone, 50 µg/mL L-ascorbic acid, and 10 mM β-glycerophosphate) [2526] was replaced every 2 days. After a period of time, the cells were washed out and gathered in an ALP lysis buffer. The dissolved protein was extracted, and 100 g of protein was incubated with p-NPP using the ALP assay buffer in order to measure ALP activity in isolated cell supernatants. The degree of the colorimetric reaction was measured using a DTX 880 device to obtain an OD measurement at 405 nm.
Osteoblast mineralization (Alizarin Red S staining)
The experimental samples were stained with Alizarin Red S as reported elsewhere [272829], with minor modifications. MG-63 cells were cultured on either the titanium discs or the culture plastic. Three titanium discs of each surface were tested. The osteogenic medium was replaced every 2 days. After a period of time, the cells were washed out and then fixed in 10% formaldehyde (Junsei, Tokyo, Japan). The cells were stained with 2% Alizarin Red S at a pH of 4.2 for 20 minutes. The stained cells were collected using the typical collection process. The absorbance level of Alizarin Red S was measured at 405 nm.
Osteoblast migration (chemotaxis assay: Transwell® cell migration assay)
For cell migration, MG63 cells (1×106 cells/mL) were suspended in a 0.1% BSA DMEM medium, and 350 μL of cell suspension was plated in the upper chambers of a Transwell® unit (8 μm pore size, SPL Insert; SPL Life Sciences, Pocheon, Korea) and incubated. The lower chambers were filled with 1 mL of the implant eluents. After 2 hours, the upper chambers were removed and the Transwell® insert was wiped with a cotton-tipped applicator. The inserts were stained with 0.2% cresyl violet, and the stained cells were eluted with citric acid. Colorimetric measurements of cresyl violet were performed using a DTX 880 device, and the OD was read at 590 nm. Nine titanium discs of each surface were tested.
Platelet adhesion
Platelet isolation (platelet-rich plasma)
Blood was obtained by cardiac puncture of a 2.5- to 3.0-kg New Zealand rabbit using a 21G needle into 4% sodium citrate (Fisher Scientific, Pittsburgh, PA, USA). Platelet-rich plasma (PRP) was made according to the technique described in a previous paper [30]. The PRP was incubated with calcium chloride (final concentration, 5 mM) (Fisher Scientific) at 37°C for 10 minutes.
Lactate dehydrogenase assay
The platelet solution had a concentration of 1×108 platelets/mL in PBS. To this solution, calcium chloride was added to yield a concentration of 2.5 mM, after which magnesium chloride was added to yield a final concentration of 1.0 mM. After 30 minutes at 37°C, the platelet suspension was placed on the titanium discs and left to adhere for 1 hour at 37°C. Nine titanium discs of each surface were tested. The platelet suspension was rinsed away to remove the non-adherent platelets. The platelet adhesion level was quantified by a lactate dehydrogenase (LDH) assay. LDH, which is released when the adherent platelets are lysed, was measured with a Triton-PBS buffer and a CytoTox 96® Non-Radioactive Cytotoxicity assay (Promega). The methods reported in previous studies [3132] were used with modifications.
SEM observation of the fibrin network
Preparation of the blood sample to obtain a fibrin clot
As previously described by Park and Davies [33], titanium discs were inserted so as to be almost press-fit into the bottoms of 24-well plates. One milliliter of PRP was added to each well and was gently mixed with blood proteins captured within the fibrin network at 37°C for 24 hours.
Preparation of the washed fibrin clot and SEM observation
To prepare for SEM observation, the fibrin clot samples were lightly rinsed with PBS and then fixed for 1 hour at room temperature using a special fixation buffer (2.5% glutaraldehyde dissolved in Dulbecco's PBS buffer at a pH of 7.0). After dehydrating the adherent fibrin network with an ethanol/water mixture, the samples were treated with hexamethyldisilazane (Sigma) and dried. The SEM procedure was completed by critical point drying of the material. The adherent fibrin networks were observed using SEM (Figure 5).
Figure 5
Scanning electron microscopy image of fibrin networks on each implant surface 1 hour after fibrin clot fixation. On the SOI surface, numerous red blood cells were visible, and the fibrin network was densely present above and around the red blood cells.
SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in calcium chloride aqueous solution, SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution.

Platelet activation
Preparation of human platelet samples and incubation of titanium discs
PRP was obtained from 3 healthy volunteers in the manner previously described [34]. As outlined by Park and Davies [33], titanium discs were inserted so as to be almost press-fit into the bottoms of 24-well plates. Nine titanium discs of each surface were tested. One milliliter of PRP was added to each well. In order to stimulate interactions between the surfaces and the platelets, the plate was gently mixed at 37°C. The supernatant was pipetted off after 1 hour for further analysis.
Enzyme-linked immunoassay (ELISA) for P-selectin
As an index of platelet activation, P-selectin, a platelet membrane glycoprotein that is expressed when platelets are activated, was measured. The previously prepared supernatants were assayed using an ELISA to measure the concentration of soluble P-selectin. All assays were performed according to the manufacturer's instructions.
Statistical analysis
Statistical analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). The records from each experiment were used to calculate the mean and standard deviation values of threads per second and the OD of the assays conducted on the 3 implant surfaces (SA, CA, and SOI). The Kruskal-Wallis test and the Mann-Whitney test (nonparametric analysis of variance) were used to analyze the differences among the 3 implant surfaces. A P value of less than 0.05 was considered to indicate statistical significance. For some tests with n<4, a statistical analysis could not be conducted, and only the mean and standard deviation were presented.
RESULTS
Surface wettability measurements (wetting velocity measurements)
Implants with the SA, CA, and SOI surfaces were immersed in blood for the measurement of wetting velocity (Figure 1B). The mean wetting velocity for each implant surface was measured as 0.000 threads/second, 0.069 threads/second, and 0.124 threads/second, respectively (Table 1). The difference between the wetting velocities of the SA and CA surfaces was statistically significant (P=0.000). The differences between the wetting velocities of the SA and SOI surfaces and between those of the CA and SOI surfaces were also statistically significant (P=0.000 and P=0.000, respectively).
Table 1
Wetting velocity

| Type of surface (n=9) | SA | CA | SOI |
|---|---|---|---|
| Velocity (threads/second) | 0 | 0.069±0.005a) | 0.124±0.012a) |
Values are presented as mean±standard deviation.
SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in calcium chloride aqueous solution, SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution.
a)Statistically significant difference compared to the SA group.
Serum albumin adsorption
BCA assay
Serum albumin was added to the titanium discs with the SA, CA, and SOI surfaces. The mean serum albumin adsorption for each surface was measured as 0.281, 1.120, and 1.287 OD, respectively (Table 2). The differences between serum albumin adsorption of the SA and CA surfaces were statistically significant (P=0.000). The differences between those of the SA and SOI surfaces and those of the CA and SOI surfaces were statistically significant (P=0.000 and P=0.000, respectively).
Table 2
Serum albumin adsorption

| Type of surface | SA | CA | SOI |
|---|---|---|---|
| BSA (OD) (n=9) | 0.281±0.006 | 1.120±0.024a) | 1.287±0.040a) |
| FITC-labeled BSA (pixels) (n=3) | 3,972±607 | 1,599,268±119,340 | 3,102,829±72,992 |
Values are presented as mean±standard deviation.
SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in calcium chloride aqueous solution; SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution, OD: optical density, FITC: fluorescein isothiocyanate, BSA: bovine serum albumin.
a)Statistically significant difference compared to the SA group.
FITC-labeled BSA
The mean protein adsorption as measured by the fluorescence intensity for the SA, CA, and SOI surfaces was 3,972, 1,599,268, and 3,102,829 pixels, respectively. The data are reported in Table 2. A statistical analysis of the differences between the groups could not be conducted because of the lack of a sufficiently large sample size. Nevertheless, large differences in fluorescence intensity could be seen between the groups, with the SA surface displaying the lowest values and the SOI surface the highest.
Observation of osteoblast morphology
SEM
MG-63 cells were incubated on each of the SA, CA, and SOI surfaces. The number of osteoblasts on the CA and SOI surfaces was higher than that on the SA surface, and the cells of the CA and SOI surfaces seemed to be further differentiated. No prominent difference was observed between the CA and SOI surfaces, but the number of osteoblasts on the SOI surface was estimated to be slightly higher (Figure 3).
CLSM
MG-63 cells were incubated on each of the SA, CA, and SOI surfaces. Immunofluorescence staining was performed for vinculin and F-actin, which constitute the cytoskeleton of the cell. As in the SEM observations, more bone cells were observed on the CA and SOI surfaces than on the SA surface (Figure 4).
Osteoblast adhesion
The mean measurements of the cell adhesion assay for the SA, CA, and SOI surfaces were 0.438, 0.842, and 0.949 OD, respectively. The data are reported in Table 3. A statistical analysis of the differences between the groups could not be conducted because of the lack of a sufficiently large sample size; however, the SA surface showed the lowest value for the cell adhesion assay.
Table 3
Osteoblast adhesion, proliferation, differentiation, mineralization, and migration

Values are presented as mean±standard deviation.
SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in calcium chloride aqueous solution, SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution, OD: optical density.
a)Statistically significant difference compared to the SA and CA groups.
Osteoblast proliferation
The mean measurements of the cell proliferation assay for the SA, CA, and SOI surfaces were 0.701, 0.837, and 0.912 OD, respectively. The data are reported in Table 3. A statistical analysis of the differences between the groups could not be conducted because of the lack of a sufficiently large sample size; the SA surface showed the lowest value and the SOI surface showed the highest value, but overall, there seemed to be little difference between the groups.
Osteoblast differentiation
The mean measurements of the osteoblast differentiation assay for the SA, CA, and SOI surfaces were 0.350, 0.379, and 0.385 OD, respectively. The data are reported in Table 3. A statistical analysis of the differences between the groups could not be conducted because of the lack of a sufficiently large sample size; the SA surfaces showed the lowest value and the SOI surface showed the highest value, but overall, there seemed to be little difference between the groups.
Osteoblast mineralization
The mean measurements of the osteoblast mineralization assay for the SA, CA, and SOI surfaces were 320.4, 382.6, and 452.1 nM, respectively. The data are reported in Table 3. A statistical analysis of the differences between the groups could not be conducted because of the lack of a sufficiently large sample size; however, the SA surfaces seemed to show the lowest value for the cell adhesion assay.
Osteoblast migration
The mean measurements of soluble P-selectin ELISA for the SA, CA, and SOI surfaces were 0.195, 0.195, and 0.215 OD, respectively (Table 3). The difference between the SA and CA surface groups was not statistically significant (P=0.931). However, the SOI surface showed a statistically significantly higher value than either the SA or the CA group (P=0.040 and P=0.031, respectively).
Platelet adhesion
The mean measurements of the LDH assay for platelet adhesion to the SA, CA, and SOI surfaces were 0.185, 0.255, and 0.298 OD, respectively (Table 4). The difference in the LDH assay between the SA and CA surfaces was statistically significant (P=0.000). In addition, the SOI surface showed a statistically significantly higher value than both the SA and the CA groups (P=0.000 and P=0.040, respectively).
Table 4
Platelet adhesion and activation

| Type of surface | SA | CA | SOI |
|---|---|---|---|
| Adhesion (OD) (n=9) | 0.185±0.016 | 0.255±0.031a) | 0.298±0.042a,b) |
| Activation (OD) (n=9) | 0.112±0.014 | 0.251±0.024a) | 0.414±0.046a,b) |
Values are presented as mean±standard deviation.
SA: conventional sandblasted, large-grit, acid-etched surface, CA: sandblasted, large-grit, acid-etched surface in calcium chloride aqueous solution, SOI: sandblasted, large-grit, acid-etched surface coated with pH buffering solution, OD: optical density.
a)Statistically significant difference compared to the SA group; b)Statistically significant difference compared to the CA group.
SEM observation of the fibrin network
The morphology of the fibrin networks adherent to each surface was observed. On the SA implant surfaces, the fewest red blood cells were visible, and a fibrin network was hardly observed. In contrast, a large number of red blood cells were located on the CA surfaces, and a fibrin network was clearly formed around the red blood cells. On the SOI surface, more red blood cells were observed, and a fibrin network was densely present above and around the red blood cells (Figure 5).
Platelet activation
The mean measurements of soluble P-selectin ELISA for the SA, CA, and SOI surfaces were 0.112, 0.251, and 0.414 OD, respectively (Table 4). The difference between the SA and CA surface groups was statistically significant (P=0.000). The differences between the SA and SOI surface groups and between the CA and SOI surface groups were also statistically significant (P=0.000 and P=0.000, respectively).
DISCUSSION
It was tested whether an SLA surface coated with a pH buffering solution displayed higher hydrophilicity and affinity for proteins, cells, and platelets than a conventional SLA surface. These in vitro studies conducted using several implant surfaces showed that this novel surface was superior to a conventional SLA surface.
Generally, wettability is quantified by the contact angle between a liquid drop and the solid surface of a flat disc. In this study, wetting velocity, which is the number of threads wetted by blood, was used to indirectly test wettability because the contact angles of the CA and SOI surfaces were almost 0°, making comparison between the groups using only the contact angle impossible. In fact, using wetting velocity to assess surface hydrophilicity or wettability may not yield accurate results. However, we still opted to measure wetting velocity because the ability to attract blood in clinical situations is what we ultimately wanted to assess. In some sense, this may be a methodological limitation of this experiment, because 2 surfaces with very high hydrophilicity were tested. The wetting velocity of the SA surface was almost 0, whereas it was much higher for the CA and SOI surfaces over a short period of time. Essentially, the SA surface appeared to be less hydrophilic than the other 2 surfaces because it was a dry surface that had not been in contact with any liquid, as used in clinical situations. For this reason, the superior result obtained for the SOI group may not have been due to the effect of the buffering agent itself. However, to compare the implant surfaces used in real clinical situations, it is reasonable to use a dry SLA surface rather than an SLA surface submerged in saline that is not isotonic. A previous study [10] comparing the SLA surface submerged in isotonic NaCl solution with a conventional SLA surface also used a dry surface for its control group.
The optimal degree of hydrophilicity of the implant surface remains unclear. Whether and if so, to what extent a super-hydrophilic implant surface is biologically and clinically superior to a conventional hydrophilic implant surface is not evident [9]. However, a more hydrophilic surface is thought to enhance osseointegration according to previous in vivo and human studies [810], as it yields higher bone-to-implant contact. Furthermore, surface wettability has been found to alter the biological responses of implant surfaces regarding the adhesion of proteins and other molecules, as well as cell interactions [9]. Similarly, in the present study, the SOI group with the highest wetting velocity also showed the highest affinity for proteins and osteoblasts.
The biochemical properties of implant surfaces, such as cell viability, cell proliferation, cell attachment, and differentiation, have been tested in previous in vitro studies [121314]. Soares et al. [12] observed the biological performance of differently-treated implant surfaces. Cell viability (mitochondrial activity), cell attachment, serum total protein, and ALP were assessed. The characteristics of the implant surface can determine the cellular response around the implant, as well as the extent of proteins adsorbed on the surface.
Martin et al. [13] performed analyses of cell proliferation, DNA synthesis, ALP activity, RNA and protein synthesis, and proteoglycan synthesis using 5 types of implant surfaces and MG-63 osteoblast-like cells. Additionally, they observed the morphology and distribution of the cells cultured on each type of surface. Their study demonstrated that surface roughness could alter osteoblast proliferation, differentiation, and matrix production.
Eriksson et al. [14] investigated cell viability, ALP activity, the level of vascular endothelial growth factor, the presence of osteocalcin, and cells positive for bone morphogenetic protein-2 according to the surface energy of implant surfaces. Surface energy seemed to be particularly important at early stages, and high surface energy was shown to promote cell differentiation and activation.
In the present study, a proliferation assay was performed to assess the adhesion and proliferation of the MG-63 cells, which was visualized using the colorimetric method of formazan dye. SEM images showed that the cells on the SOI surfaces were more differentiated and had proliferated to a greater extent than those on the other surfaces. Osteoblast differentiation was represented by ALP concentration, since ALP is highly expressed in the proliferation stage of the osteoblast [21222324]. Osteoblast mineralization was represented by the quantification of calcified mineral stained with Alizarin Red S. Alizarin Red S binds to calcium deposits in cell cultures, which is useful for the detection of extracellular matrix calcification [272829]. Additionally, osteoblast migration was tested with the Transwell® cell migration assay, which measures cell mobility toward a chemoattractant gradient [35]. Although the repeated number of experiments for cell adhesion, proliferation, differentiation, and mineralization was not statistically sufficient, there was a tendency for the SA surface to be the least osteoblast-friendly and the SOI surface to be the most osteoblast-friendly in this study.
Di Iorio et al. [16] observed fibrin clots on implant surfaces, and the black points on the SEM images, which were taken to indicate the presence of fibrin clots, were automatically counted using special software. In the present study, the platelet adhesion level was quantified by measuring LDH, which is released during the lysis of adherent platelets. The platelet activation level was quantified by measuring P-selectin, the platelet membrane glycoprotein expressed when platelets are activated. In the platelet adhesion test, the SOI surface showed the highest mean value, but without statistical significance compared to the CA surface. In the platelet activation test, the SOI surface exhibited the highest platelet activation, with statistical significance. The SEM images also showed the same results, with a network of red blood cells and fibrin clearly formed on the SOI surface.
Osteoblast activity peaks at pH 7.4, a weakly basic condition, and almost disappears below 6.9 [1819]. In this experiment, a weakly basic medium was used to culture MG-63 cells, as in blood. Although the cell culture medium was exchanged periodically, the pH could not be kept constant, as it was impacted by the metabolites of the cells. Furthermore, various laboratory errors could affect pH in in vitro experiments. Even when drilling or destruction of bone does not occur, which would produce a weakly acidic pH, a pH buffer may be helpful to keep the pH constant even in in vitro conditions. The pH buffering agent seems to make conditions favorable for osteoblast activity by keeping pH constant or at least preventing significant changes in pH, as the results of this experiment showed increased osteoblast activity in the SOI group. Calcium ions also bind to various proteins in solution, keeping the solution pH weakly basic and functioning as a pH buffer. It should be taken into account that calcium ions themselves contribute to osteogenic processes, but it may also be important that the CA surface has a pH buffering effect, although it is not as effective as the SOI surface. In addition, platelet adhesion and activation were significantly higher on the CA and SOI surfaces than on the SA surface. Platelet activity is inhibited by extracellular acidosis and promoted by extracellular alkalosis [20]. Since platelet activity is affected by extracellular pH, it is thought that platelets may have been activated on the CA and SOI surfaces, which have a pH buffering effect.
In some experiments, significant differences were observed between the CA and SOI surfaces, whereas other experiments showed no significant differences. Since both CA and SOI surfaces have a pH-buffering effect in isotonic solution, the results of the experiments did not appear to be consistently different unless they showed a major effect on cell activity. In contrast, the SA surface, which was not immersed in solution and had no pH buffering effect, showed a significantly inferior results in most experiments.
An SLA surface with a pH buffering agent exhibited higher hydrophilicity and affinity for proteins, cells, and platelets than a conventional SLA surface. Since the number of experiments performed was not standardized and was statistically insufficient in some experiments, caution is needed in interpreting the results. Under acidic conditions after a drilling procedure, the pH buffering capacity is also expected to increase the level of ALP, promoting thrombogenesis and osteoblast activity. Within the limits of this study, it may be concluded that this novel surface can induce attachment to platelets, bone-forming proteins, and cells more than a conventional SLA surface, allowing stable and fast osseointegration to be achieved. Further studies should be conducted to directly compare an SLA surface with a pH buffering agent with other conventional surfaces with regard to its safety and effectiveness in clinical settings.
 XML Download
XML Download