

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Optimal periodontal healing and regeneration of lost periodontal structures in intrabony defects can be achieved by maximal preservation of soft tissues and maintenance of primary wound closure after application of regenerative material into osseous defects [1]. The introduction of the operative microscope into periodontal practice led to further enhancement of clinical outcomes [2].
Applying the principles of the papilla preservation flap, Cortellini and Tonetti [2] recommended the use of the minimally invasive surgical technique (MIST) with microsurgical instruments and an operating microscope and demonstrated better healing in terms of a significant gain in attachment level, pocket depth reduction, and minimal gingival recession in the treatment of isolated deep intrabony defects [3]. Cortellini and Tonetti [4] further enhanced MIST by developing the modified MIST (M-MIST) to reduce surgical invasiveness by limiting the incision line to the buccal side. This fulfilled the following objectives: to maintain the interdental papillary height by minimizing its tendency to collapse, to increase the likelihood of primary wound closure, and to reduce the chances of gingival recession. The efficacy of M-MIST in the treatment of intrabony defects has been studied in randomized controlled clinical trials, with and without regenerative materials such as enamel matrix derivative (EMD), bone mineral derived xenograft (BMDX), and recombinant human platelet-derived growth factor (rhPDGF) [56]. However, the concomitant use of M-MIST with autologous platelet-rich fibrin (PRF) has not been previously attempted.
PRF is considered a second-generation platelet concentrate; it has trimolecular fibrin morphology with a 74% composition of leukocytes, and is known to have osteoconductive, immunomodulatory, and neo-angiogenic properties [78910]. In vitro studies have demonstrated that PRF acts as a scaffold for the culture of human periosteal cells and can be applied in bone tissue engineering [811]. Furthermore, it releases autogenous growth factors gradually and manifests a stronger effect on the proliferation and differentiation of osteoblasts [12]. Clinical studies have also demonstrated convincing results of PRF in achieving periodontal regeneration in intrabony defects, class II furcation defects, coronally advanced flaps with multiple gingival recession, and sinus augmentation during implant placement [13141516].
Considering the benefits of PRF for augmenting bone and soft tissue healing, it was hypothesized that PRF could act as an adjunct to M-MIST, potentially yielding better results than M-MIST alone in the treatment of isolated intrabony defects. Thus, this study was conducted to observe the outcomes of periodontal surgery in which M-MIST was used with or without PRF for the treatment of isolated intrabony defects.
MATERIALS AND METHODS
Study design
This study was designed as a randomized clinical trial and performed at the Department of Periodontics, Post Graduate Institute of Dental Sciences (PGIDS), Rohtak, Haryana. The study protocol followed the ethical standards outlined in the 1975 Declaration of Helsinki, revised in 2013. The study was approved by the Institutional Review Board and ethical approval (IEC No. PGIDS/IEC/2016/90) was obtained from the ethical committee of PGIDS. This clinical trial was registered on ClinicalTrials.gov (NCT03169920).
Patient selection
Patients were selected from the outpatient department of periodontics, with no discrimination on the basis of sex, caste, religion, or socioeconomic status. In total, 85 patients were examined, and 36 patients who had chronic periodontitis and a single-site buccal probing pocket depth (PPD) of ≥5 mm and met the inclusion criteria were selected. The procedure was explained to each patient in the patient's native language. Patients were enrolled in the study only after obtaining written informed consent.
The inclusion criteria were as follows: 1) patients with chronic periodontitis between the ages of 28 and 55 years who were otherwise systemically healthy with the presence of at least a single site with PPD and clinical attachment level (CAL) ≥5 mm on the buccal surface associated with a 3-walled osseous defect depth of ≥3 mm (Figure 1A and D) [17] (according to new classification scheme of periodontal and peri-implant diseases and conditions, the current status of the patients included in the present study was classified as stage II or III periodontitis [18]); and 2) patients demonstrating optimal plaque control after phase 1 periodontal therapy (plaque index [PI] <1.5). The exclusion criteria were as follows: 1) patients with a systemic illness such as diabetes mellitus or arthritis; 2) patients on systemic medications such as corticosteroids or calcium channel blockers or taking long-term non-steroidal anti-inflammatory drugs; 3) patients with a history of periodontal treatment over the past 3 months; 4) pregnant or lactating women; 5) smokers and tobacco chewers; 6) patients who had periodontal sites with fractured and perforated roots; 7) teeth with grade III mobility and furcation involvement; and 8) non-vital tooth with or without periapical pathology.
Figure 1
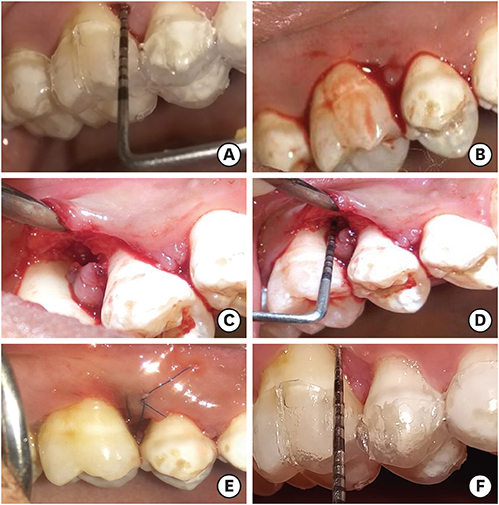
Procedure depicting the M-MIST. (A) Preoperative photograph showing a single-site pocket probing depth of 6 mm on the buccal surface. (B) Intraoperative photograph showing the M-MIST incision. (C) Intrabony defect after debridement. (D) Measurement of the defect depth with a UNC-15 periodontal probe. (E) A modified vertical internal mattress suture was placed. And (F) Residual pocket probing depth 6 months after surgery.
M-MIST: modified minimally invasive surgical technique.

Clinical parameters
The full-mouth periodontal parameters included the percentage of sites with bleeding on probing (BOP%), PPD, and CAL. Eight weeks after completion of the initial phase of periodontal therapy and just before surgery, baseline clinical and radiographic measurements were recorded. Site-specific clinical parameters were recorded for the PI [19], gingival index (GI) [20], BOP%, PPD, relative attachment level (RAL), and relative gingival margin level (RGML). All the parameters were clinically assessed by a single examiner. Intra-examiner calibration was conducted in 10% of the patients for PPD and RAL measurements (2 measurements at an interval of 48 hours). Calibration was judged reproducible when both the measurements differed by 1 mm or less, 95% of the time.
Periodontal parameters were assessed at 4 sites (mesiobuccal, midbuccal, distobuccal, and midlingual/midpalatal) for PI and GI, and at 6 sites (mesiobuccal, midbuccal, distobuccal, mesiolingual/mesiopalatal, midlingual/midpalatal, and distolingual/distopalatal) for BOP%, PPD, RAL, and RGML. A periodontal probe (PCP-UNC 15 periodontal probe, Hu-Friedy, Chicago, IL, USA) and a customized stent were used to measure the periodontal parameters at each follow-up. The customized stent was prepared by using a bioplastic sheet using a Biostar machine (Scheu, Eurodontic Ltd, Sheffield, United Kingdom) with a model prepared from the patient's dental impression.
Radiographic parameters
Intraoral periapical radiographs were taken using the long-cone paralleling technique and standardized exposure parameters (70 kVp, 3.5 mA, and 0.2 seconds) by the investigator (A.N.). To maintain the projection geometry and to stabilize the X-ray film at subsequent appointments, a customized silicone stent was made for the surgical site in each patient. Radiographs of the selected teeth were obtained at baseline and 6 months after surgery. All radiographs were assessed by the investigator (T.N.) to ensure blinding. Radiographic analysis was done using ImageJ software [21]. The anatomical landmarks on the tooth associated with the intrabony defect were identified on the radiographs, and included the cemento-enamel junction (CEJ), alveolar crest (AC), and the base of the defect (BOD). Radiographic defect depth (RDD) was measured as the distance from the AC to BOD by drawing a perpendicular line from the AC to a line running parallel to the long axis of the tooth. The baseline and 6-month radiographs were compared to calculate linear bone growth (LBG), percentage bone fill (%BF) and change in AC position (C-ACP) [22]. LBG was calculated as the difference between the CEJ-BOD value at 6 months and the CEJ-BOD value at baseline. The following formula was used to calculate %BF: %BF=(LBG/RDD value at baseline)×100. C-ACP was calculated as the difference between the baseline and 6-month values of the CEJ-AC distance [23].
Randomization
Patients were allocated to groups using randomization by a computer-generated table by another investigator (S.R.K.) [24]. The periodontist was informed of the treatment allocated to the patient at the time of periodontal surgery after confirming that the bone defect anatomy fit the inclusion criteria. All periodontal operations were performed by a trained periodontist (A.N.). The baseline, 3-month, and 6-month parameters were recorded by another investigator (T.S.), who was blinded to the nature of the intervention received by the patients. All the patients were randomly assigned to either the test group, which received PRF along with M-MIST in isolated intrabony defects under an operative microscope, and the control group, in which M-MIST alone was performed under an operative microscope.
PRF preparation
Blood was collected in an anticoagulant-free sterile tube and immediately centrifuged in a table-top centrifugation machine (Remi Elektrotechnik Limited, Mumbai, India) at 3,000 rpm for 10 minutes. After centrifugation, the fibrin clot was collected with sterile tweezers. Red blood cells were separated from the bottom of the fibrin clot and the PRF membrane was formed by gently pressing the clot between two moist gauze pieces [7].
Surgical approach (M-MIST)
All surgical procedures were performed under an operating microscope (OPMI PICO, Carl Zeiss, Gottingen, Germany) with a magnification of ×6. Povidone-iodine solution (Glide Chem Pvt Ltd, New Delhi, India) was used for extraoral and intraoral antisepsis. After the administration of local anesthesia (2% lidocaine with 1:80,000 epinephrine, Coax Bioremedies Pvt. Ltd, Hisar, India), the papilla associated with the intrabony defect was surgically approached using M-MIST as described by Cortellini and Tonetti [4] (Figure 1B). Intrabony defects were debrided using mini-curettes (SAS 3/4, 5/6, 11/12, 13/14, Hu-Friedy) aided with an operating microscope in both the groups (Figure 1C and D). PRF was delivered into the intrabony defect in the test group, and pre-suturing was done before the placement of PRF. Modified vertical internal mattress sutures were placed in both the test and control groups using 6-0 Ethicon polypropylene sutures with a 3/8 reverse cutting needle (Johnson & Johnson Ltd., Aurangabad, India) (Figure 1E).
Postoperative care
Postoperative instructions were given to all patients, advising them not to use mechanical means of plaque control until the suture was removed. All patients were advised to rinse with 0.2% chlorhexidine (ICPA Health Products Limited, Ankleshwar, India) twice daily until they could resume tooth brushing. One week after surgery, the suture was removed. All patients received encouragement to maintain good oral hygiene at each visit. Patients were examined weekly after surgery for 1 month, and again at 3 months and 6 months (Figure 1A and F).
Statistical analysis
In total, 36 patients were selected and divided into 2 groups of 18 each. The sample size of 18 patients in each group was found sufficient to detect a clinically significant difference in PPD reduction and CAL gain with an effect size of 1 and a type 1 error (α) of 0.05, at 80% power. Upon application of the Shapiro-Wilk test, the data were found to be normally distributed for PI, GI, RDD, and CEJ-BOD. Hence, further analysis of these parameters was done using the paired t-test for intragroup comparisons and the independent t-test for intergroup comparisons.
All other periodontal and radiographic parameters were found to be non-normally distributed; therefore, they were analyzed using the Wilcoxon signed-rank test for intragroup comparisons and the Mann-Whitney U test for intergroup comparisons.
RESULTS
A total of 36 patients fulfilling the inclusion criteria were enrolled in the study, and 32 patients (16 from each group) completed the 6-month follow-up. Four patients (2 in each group) did not report at the 3-month follow-up (Figure 2). On postoperative day 7, primary closure was observed in all patients except in 1. Gingival recession was observed in 2 patients: 1 patient from the test group in whom the flap margins were not approximate on the seventh postoperative day, and another patient from the control group who presented with trauma from masticatory forces at the 3-month follow-up. The recruitment of the patients was started in November 2016, and the study was completed in March 2018.
Figure 2
Flow chart of the participants in this study.
PRF: platelet-rich fibrin, M-MIST: modified minimally invasive surgical technique.

Table 1 demonstrates non-significant differences in age and sex between both groups. After applying the independent t-test for PI, GI, RDD, and CEJ-BOD and the Mann-Whitney U test for BOP%, PPD, RAL RGML, and CEJ-AC, it was found that all parameters were comparable at baseline (P>0.05).
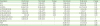
Table 1
Demographic data, clinical characteristics, and radiographic defect features at baseline in the TG and CG
Values are presented as mean±standard deviation.
CG: control group, TG: test group, PI: plaque index, GI: gingival index, BOP: bleeding on probing, PPD DEEP: probing pocket depth at the deepest site, PPD ADJ: probing pocket depth at the adjacent site, RAL DEEP: relative attachment level at the deepest site, RAL ADJ: relative attachment level at the adjacent site, RGML DEEP: relative gingival margin level at the deepest site, RGML ADJ: relative gingival margin level at the adjacent site, RDD: radiographic defect depth, CEJ-BOD: cement-enamel junction to base of defect, CEJ-AC: cemento-enamel junction to the alveolar crest.
The intragroup comparison of clinical parameters showed consistently significant (P≤0.05) improvements in PI, GI, BOP%, PPD, RAL, and a stable RGML at both the deepest and adjacent sites at 3- and 6-month postsurgery (paired t-test and Wilcoxon signed rank test). LBG and %BF were also demonstrated meaningful changes at 6 months in both groups.
As shown in Table 2, an intergroup comparison of site-specific parameters revealed similar improvements in PI, GI, BOP%, PPD, RAL, and no significant change in RGML at both the deepest and adjacent sites at 3 and 6 months post-surgery (P>0.05). LBG, %BF, and C-ACP also demonstrated comparable improvements (P>0.05) in both groups at the end of 6 months.
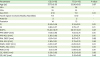
Table 2
Intergroup comparison of improvements (Δ) in periodontal and radiographic parameters between baseline and 3 and 6 months in the CG and TG
Values are presented as mean±standard deviation.
CG: control group, TG: test group, PI: plaque index, GI: gingival index, BOP%: percentage of sites with bleeding on probing, PPD DEEP: probing pocket depth at the deepest site, PPD ADJ: probing pocket depth at the adjacent site, RAL DEEP: relative attachment level at the deepest site, RAL ADJ: relative attachment level at the adjacent site, RGML DEEP: relative gingival margin level at the deepest site, RGML ADJ: relative gingival margin level at the adjacent site, LBG: linear bone growth, %BF: percentage bone fill, C-ACP: change in the alveolar crest position.
DISCUSSION
To the best of the authors' knowledge, this is the first study that attempted to observe the effect of PRF with M-MIST in the treatment of single-site intrabony defects. M-MIST was proposed as an extension of MIST by Cortellini and Tonetti [4]. Since the debridement is performed through a narrow buccal window that limits visibility, the use of magnifying devices to facilitate scaling, root planing, and granulation tissue removal is mandatory [2].
PRF has the property of promoting cellular migration through its fibrin scaffold, which is advantageous in wound healing [8]. The leukocytes present in the PRF matrix are involved in the production of significant amounts of growth factors [25]. The granules of platelets in PRF contain serotonin, von Willebrand factor, factor V, osteonectin, and antimicrobial proteins [26]. Upon contact of platelets with the collagen of damaged blood vessels, degranulation and sequential release of cytokines take place, which further aid in hemostasis [27]. Since it is autologous, PRF does not induce an inflammatory reaction at the site of delivery. Dohan et al. [10] stated that PRF has immunological properties and a high concentration of vascular endothelial growth factor A cytokines, which play a direct role in endothelial cell growth and angiogenesis [28]. In a split-mouth, randomized controlled clinical trial, Patel et al. [13] demonstrated that the adjunctive use of PRF was advantageous for the treatment of intrabony defects, along with open flap debridement.
The results of the present study showed similar reductions in PPD at the deepest site in both groups after 6 months of follow-up (ΔPPD, 4.18±1.00 mm in the M-MIST group and 4.12±0.95 mm in the M-MIST with PRF group). These results are in accordance with results of Mishra et al. [6], who used a rhPDGF composed of 2 B subunits (rhPDGF-BB gel) with M-MIST (ΔPPD, 3.8±0.9 in the M-MIST group and 4.2±0.6 in the M-MIST with rhPDGF-BB group), and slightly greater than those reported by Ribeiro et al. [29], who applied EMD with MIST (ΔPPD, 3.55±0.88 mm in the MIST group and 3.56±2.07 in the MIST with EMD group). Furthermore, a similar reduction in probing depth was reported by Cortellini and Tonetti [5], who compared an M-MIST alone group with an M-MIST and EMD group and an M-MIST with EMD and BMDX group (ΔPPD, 4.4±1.6 mm in the M-MIST group, 4.4±1.2 mm in the M-MIST with EMD group, and 4.0±1.3 mm in the M-MIST with EMD and BMDX group).
The present study reported a similar gain in attachment level in both groups at the deepest site (ΔRAL, 4.0±1.09 mm in the M-MIST group and 4.062±1.63 mm in the M-MIST with PRF group). This was greater than the gain in attachment level (Δ Relative CAL [RCAL], 2.6±0.8 mm in the M-MIST group and 3.0±0.9 mm in the M-MIST with rhPDGF-BB group) reported by Mishra et al. [6], who used rhPDGF-BB gel with M-MIST and by Ribeiro et al. [29] at the end of a 6-month follow-up (Δ RCAL, 2.85±1.19 mm in the MIST group and 2.56±1.12 mm in the MIST with EMD group). The present study observed an attachment level gain comparable to that reported by Cortellini et al. [5], who compared an M-MIST alone group with an M-MIST and EMD group and an M-MIST with EMD and BMDX group (ΔCAL, 4.1±1.4 mm in the M-MIST group, 4.1±1.2 mm in the M-MIST with EMD group and 3.7±1.3 mm in the M-MIST with EMD and BMDX group).
A non-significant change in the position of the gingival margin was observed in this study at 3 months and 6 months in both the test and control groups. The studies conducted by Mishra et al. [6] and Ribeiro et al. [29] also showed a minimal increase in gingival recession. The remarkable stability of the marginal gingiva can be attributed to the unhampered blood supply to the papilla during the surgical procedure and the stability of blood clot inside the intrabony defect. It is very likely that both these factors act synergistically to prevent the collapse of the papilla into the intrabony defect [5].
Regarding LBG and %BF (LBG, 1.07±0.38 mm in the M-MIST group and 1.107±0.322 mm in the M-MIST with PRF group; %BF, 33.98%±11.13% in the M-MIST group and 37.4%±10.05% in the M-MIST with PRF group), both groups in the present study demonstrated comparable improvements. Mishra et al. [6] (LBG, 1.85±0.6 mm in the M-MIST group and 1.89±0.6 mm in the M-MIST with rhPDGF-BB group; %BF, 35.04%±10.99% in the M-MIST group and 36.02%±17.74% in the M-MIST with rhPDGF-BB group) and Ribeiro et al. [29] (CEJ-BD, 0.95 ± 0.72 mm in the MIST group and 1.52 ± 1.22 mm) in the MIST with EMD group) also reported similar results. Cortellini and Tonetti [5] demonstrated a higher %BF at the end of a 1-year follow-up (77%±19% in the M-MIST group, 71%±18% in the M-MIST with EMD group, and 78%±27% in the M-MIST with EMD and BMDX group) than at the 6-month follow-up period of the present study.
The change in the AC position was found to be +0.09±0.01 mm in the control group and +0.03±0.21 mm in the test group. This implies that there was a mean bone gain of 0.09 mm in the control group and 0.03 mm in the test group at the most coronal position of the crest of the alveolar bone. Since the radiographic analysis in this study was carried out using conventional periapical radiographs, it cannot be ruled out that the use of contemporary techniques, such as cone-beam computed tomography (CBCT) and digital subtraction radiography, could have yielded more accurate results for LBG and %BF.
The present study showed similar results in terms of clinical and radiographic parameters for M-MIST alone and M-MIST with PRF. Several studies have reported that PRF, when used with other bone graft materials, yielded better clinical results in terms of periodontal regeneration [30313233]. The use of bone graft materials with PRF in M-MIST may yield better results; this possibility needs further investigations in clinical trials.
Strength of the present study is the use of strict inclusion and exclusion criteria. The standardized measurement of periodontal parameters was done using customized stents at each follow-up to maintain accuracy. The study was designed as a randomized controlled clinical trial, which is considered the gold standard for clinical trials. The investigators who assessed the outcomes were not aware of the group allocation, thereby ensuring blindness to avoid bias. Smokers were strictly excluded, as smoking may act as a confounder in periodontal healing.
The limitations of this study included the use of conventional radiography instead of CBCT or digital subtraction radiography, a smaller sample size due to dropouts, and a short follow-up of 6 months due to the time-bound nature of this study. In further studies, a long-term follow-up of at least 1 year is suggested for the better evaluation of bone gain.
Within the limitations of this study, it can be concluded that M-MIST alone and PRF with M-MIST yielded similar improvements in periodontal parameters. Single-site periodontal pockets with intrabony defects can be easily debrided by M-MIST alone, but it cannot be ruled out at this stage that using PRF in combination with regenerative bone grafts may yield better healing than M-MIST alone. However, further research is needed in this regard, with a longer follow-up period and large multicenter trials to corroborate the results of the present study.
 XML Download
XML Download