

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Severe cutaneous adverse reactions (SCAR) to drugs are among the most life-threatening conditions involving the skin, mainly encompassing drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN), and acute generalized exanthematous pustulosis (AGEP)1. DRESS is a hypersensitivity reaction, characterized by a variable combination of heterogenous clinical presentations2, such as fever, lymphadenopathy, eosinophilia, facial edema, erythroderma and even internal organ involvement3. SJS/TEN is known as a drug-induced hypersensitivity reaction, showing atypical target lesions and bullous lesions with acute exanthema. SJS and TEN are differentiated by the extent of epidermal detachment (SJS with body surface area [BSA] <10%, TEN with BSA >30%, and anything in-between called SJS-TEN overlap syndrome)4. AGEP is characterized by the rapid development of multiple non-follicular, sterile pustules on an erythematous base, mainly attributed to drugs, especially antibiotics, in the majority of cases5.
Given the severity of SCAR, numerous studies have been conducted. However, to date no specific treatment has been universally accepted. Meanwhile, information of SCAR patients in Asian population was extremely limited. In this retrospective study, we determined the reasons for administration in patients hospitalized with SCAR, the clinical pattern of reactions and the drugs causing adverse reactions in the biggest department of dermatology in China. Most notably, we aimed to examine the role of systemic corticosteroids in SCAR treatment and explore the potential prognostic factors of SCAR.
MATERIALS AND METHODS
Patient selection
A retrospective review of electronic medical records was performed for all patients admitted to Department of Dermatology, Huashan Hospital as DRESS, SJS/TEN, and AGEP between January 2014 and December 2017. Inclusion criteria for this study required that patients met the diagnostic guidelines set by the European Registry of Severe Cutaneous Adverse Reactions (RegiSCAR)6 for DRESS and SJS/TEN or the modified European Study of Severe Cutaneous Adverse Reactions (EuroSCAR) described by Sidoroff et al.7 for AGEP. No patients were lost to follow-up in this retrospective study. Informed consent was obtained from all patients to use their electronic medical data. The study protocol was approved by the Ethical Committee of Huashan Hospital (IRB no. KY2019-316).
Assessment of drug causality
The drugs responsible for SCAR were defined as previously described67. The evaluation of drug causality was decided by a group of experienced dermatologists. In brief, if a drug was used continuously for more than three months, withdrawn for more than 14 days, or with a latent period less than three days, it would not be considered as the culprit drug for DRESS or SJS/TEN6. However, latent period for AGEP could be less than three days (typically within 48 hours or 24 hours for antibiotics)8. The “latent period” referred to the period from drug initiation to symptom onset. Moreover, previous use without a drug eruption history decreased suspicion, whereas an earlier reaction prioritized the drug. Hereafter, the remaining suspected drugs were re-evaluated based on the literature review. For cases with several suspected drugs remained, those with high notoriety were firstly considered (listed in Table 1) and those with low notoriety were marked as ‘possible’ (not listed in Table 1). Moreover, the sensitizing properties of different drugs were also taken into account.
Assessment of SCAR outcomes
Clinical information with regards to demographic data, comorbidities, latency, and duration from onset to maximum BSA or BSA detachment (maximum BSA detachment for SJS/TEN and maximum BSA skin lesion involvement for DRESS and AGEP), maximum BSA or BSA detachment, time from onset to pharmacotherapy, co-administration of corticosteroids and intravenous immunoglobulin (IVIG) was recorded and analyzed. Outcomes analyzed for pharmacotherapy were progression of disease (defined as duration from the index day to maximum BSA or BSA detachment), severity of disease (maximum BSA or BSA detachment) and mortality. The 25th and 75th percentile of the time length of the lesions withdrawal by 50% were calculated, and prognosis were defined as good when 50% of the lesions withdrew less than seven days.
Statistical analysis
Linear regression analysis was applied to explore the association between the time from onset to corticosteroids treatment and progression of disease (duration from the index day to maximum BSA or BSA detachment) or severity of disease (maximum BSA or BSA detachment), while mortality analysis was based on logistic regression. Linear regression models were adjusted for age, sex, and disease classification (SJS/TEN, DRESS or AGEP) and co-administration of IVIG in order to take into account the confounding factors. In terms of prognostic factor analysis of SCAR, chi-squared test and one-way ANOVA were applied for univariate analysis. Then, the variables significantly associated with prognosis of SCAR in univariate analysis and the variables of great clinical concerns were further included in Cox regression analysis and enter selection was applied. The categorical variables were coded. The threshold for significance was set at p-value <0.05. All statistical analyses were performed using IBM SPSS Statistics ver. 21.0 software (IBM Corp., Armonk, NY, USA).
RESULTS
Demographics
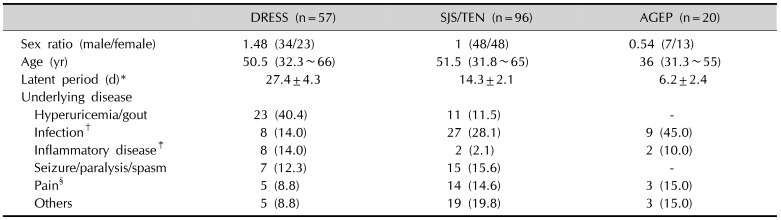
As shown in Table 2, 173 SCAR patients were studied in this study. SJS/TEN was the most prevalent SCAR observed (55.5%, 96 cases), followed by DRESS (32.9%, 57 cases) and AGEP (11.6%, 20 cases). Males were predominant (1.48:1) in DRESS and females were predominant (0.54:1) in AGEP, whereas the number of males and females were similar for SJS/TEN. The mean period from drug initiation to symptom onset is 27.4 days for DRESS, 14.3 days for SJS/TEN, and 6.2 days for AGEP. The most common underlying diseases justifying the use of drugs were hyperuricemia or gout in DRESS, infection in SJS/TEN and AGEP.
Clinical characteristics
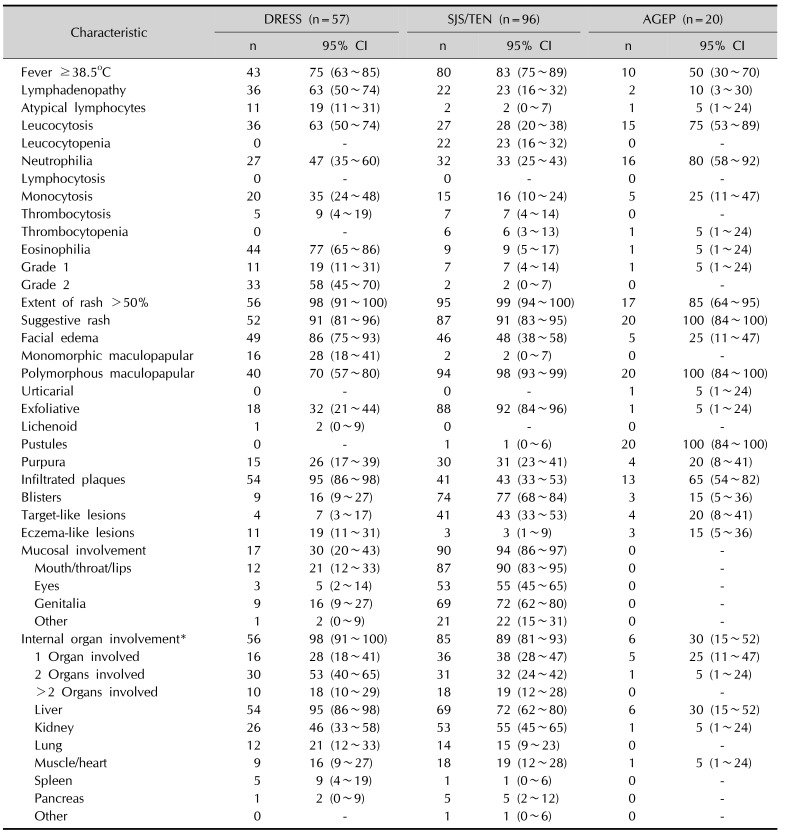
The clinical characteristics of the 173 SCAR patients were summarized in Table 3. Fever ≥38.5℃ was documented in 75% of DRESS patients, 83% of SJS/TEN patients and 50% of AGEP patients. Lymphadenopathy was observed in 63% and 23% of DRESS and SJS/TEN patients respectively. Notably, 19% DRESS patients, 2% SJS/TEN patients and 5% AGEP patients showed peripheral atypical lymphocytes. Leucocytosis was found in 63% of DRESS, 28% of SJS/TEN and 75% of AGEP patients. Leucocytopenia was infrequent, with only 23% in SJS/TEN. Neutrophilia was found in 47% of DRESS, 33% of SJS/TEN and 80% of AGEP patients. Monocytosis was prevalent in DRESS patients (35%) but not in SJS/TEN (16%) and AGEP (25%). Thrombocytosis was infrequent, with only 9% in DRESS and 7% in SJS/TEN patients. Thrombocytopenia was rare, with only 6% in SJS/TEN. Eosinophilia, defined as an absolute eosinophil count ≥700 U/L, was present in 77% of DRESS patients. While in SJS/TEN, only 9% of patients had an absolute eosinophil count ≥700 U/L.
All patients experienced an acute skin eruption. 91% of DRESS and SJS/TEN patients, and all of the AGEP patients had suggestive rash. The criteria for suggestive rash was facial edema or exfoliative dermatitis in DRESS, edematous erythema, target-like lesions, mucosal involvement, flaccid blisters, and exfoliation in SJS/TEN, and sterile nonfollicular pustules in AGEP6910. The rash was a monomorphic maculopapular in 28% of DRESS patients and only 2% of SJS/TEN patients, while in all other cases it was polymorphous, including variable combinations of other lesions. For example, DRESS patients usually had infiltrated plaques (95%), exfoliation (32%), purpura (26%), eczema-like lesions (19%), and blisters (16%). Whereas, SJS/TEN patients usually had exfoliation (92%), blisters (77%), target-like lesions (43%), and purpura (31%). Facial edema was observed in 86% of DRESS patients, 48% of SJS/TEN patients and 25% of AGEP patients. Mucosal involvement was recorded in 30% of DRESS patients and 94% of SJS/TEN patients. Most popular were oral lesions (21% of DRESS patients and 90% of SJS/TEN patients).
In terms of systemic involvement, most frequently the reaction affected the liver (95% of DRESS patients, 72% of SJS/TEN patients, and 30% of AGEP patients), followed by kidney (46% of DRESS patients, 55% of SJS/TEN patients, and 5% of AGEP patients) and lung (21% of DRESS patients and 15% of SJS/TEN patients).
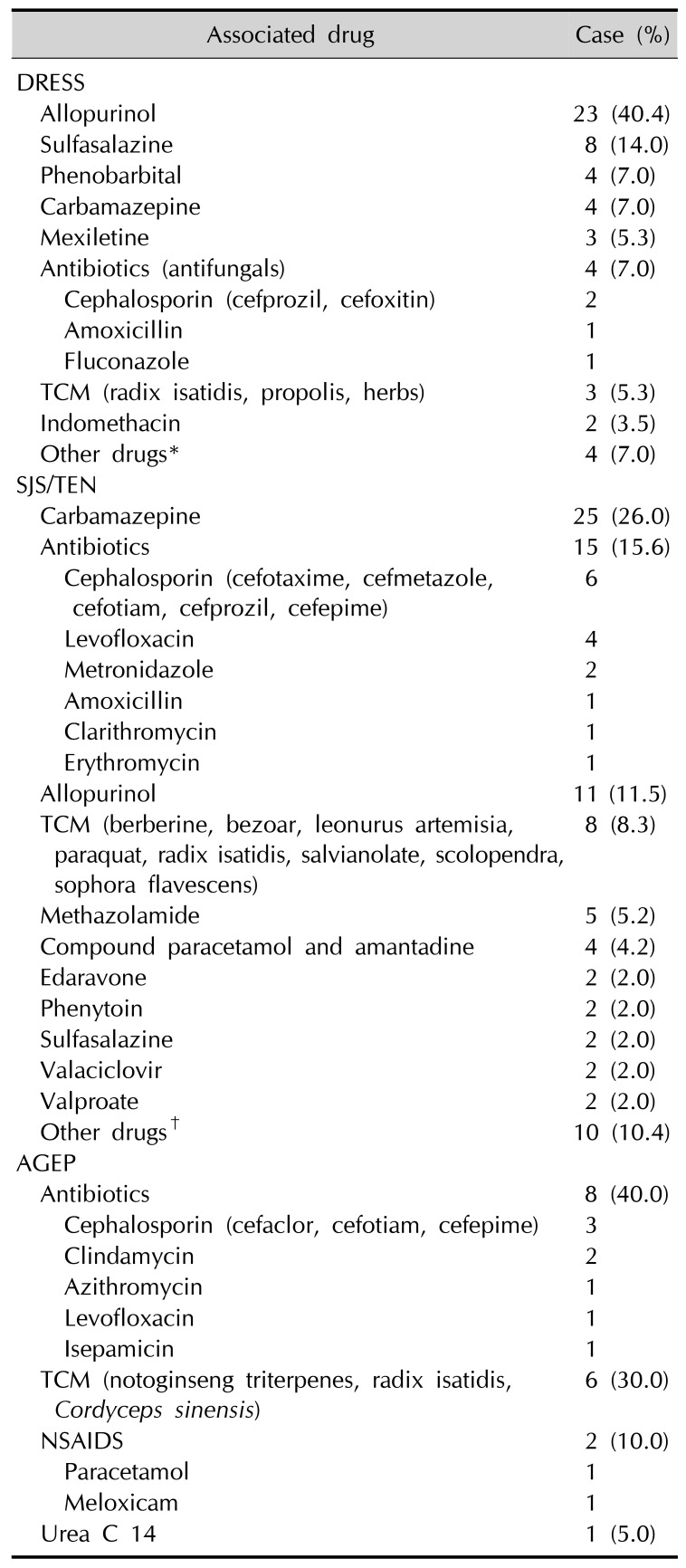
Causative drugs
In this study, two DRESS patients (3.5%), eight SJS/TEN patients (8.3%), and three AGEP patients (15.0%) were not exposed to any medication according to the criteria of culprit drugs in RegiSCAR6 or modified EuroSCAR for AGEP7. As for other SCAR cases, the summary of drug causality was presented in Table 1. In addition, we categorized all SCAR cases by causative drugs into three groups: allopurinol group, carbamazepine group, and other causative drugs group. Univariate analysis of the outcome measures showed difference in the severity of SCAR (p=0.031) but no difference in the progression of SCAR among three causative drugs groups. Further two-two comparisons also showed that the difference between allopurinol group and carbamazepine group (p=0.039) and the difference between carbamazepine group and other causative drugs group were statistically significant (p=0.010). However, when stratified by disease types, causative drugs showed difference only in the severity of SJS/TEN, whereas no differences in the severity of DRESS or AGEP.
Treatment
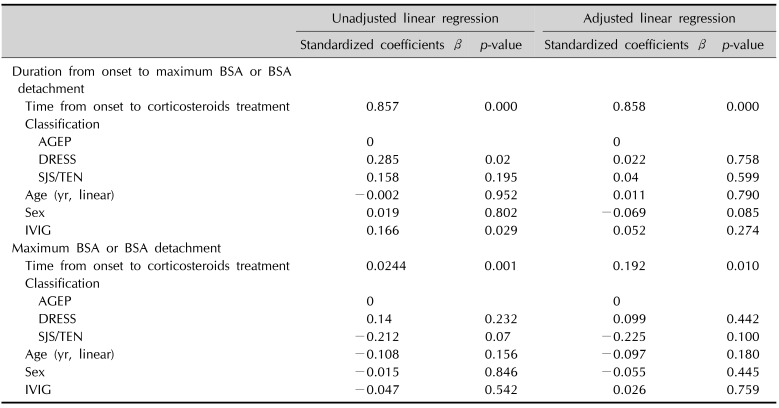
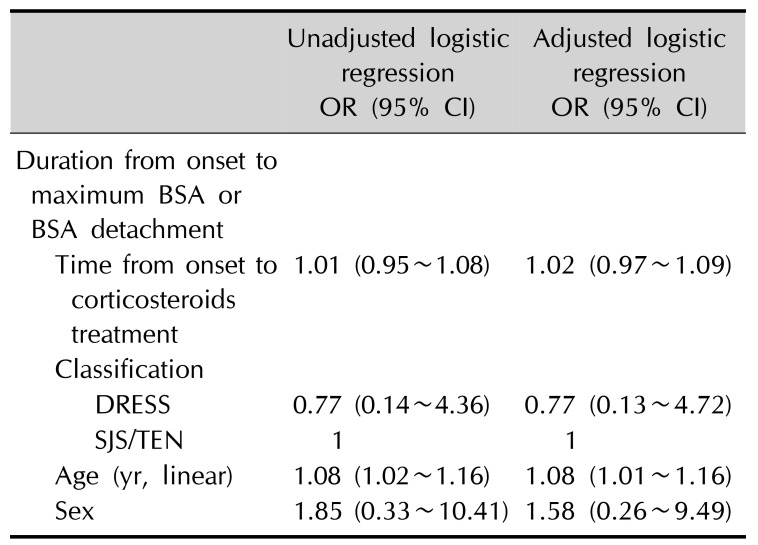
In our observational study, 56 DRESS patients (98.2%), 96 SJS/TEN patients (100.0%), and 20 AGEP patients (100.0%) received systemic corticosteroids. Intravenous methylprednisolone was given at 1~1.5 mg/kg/d. Once the progression of the disease was halted, which manifested as no new lesions, Nikolsky sign turning negative, exudation improved, re-epithelialization and laboratory test results being stable, the dose of corticosteroids was tapered promptly. Meanwhile, 43 DRESS patients (75.4%), 88 SJS/TEN patients (91.6%), and four AGEP patients (20.0%) received treatment with IVIG. IVIG was administered at 0.4 g/kg/d for over 5 days. Univariate analysis of the outcome measures showed that early use of systemic corticosteroids was significantly and negatively related to the progression of SCAR (p=0.000) and the severity of SCAR (p=0.001). Further multivariate analysis also indicated the negative linear association of early use of systemic corticosteroids and the progression (p=0.000) and the severity of SCAR (p=0.01) (Table 4). Duration from onset to maximum BSA or BSA detachment will be 0.858-day longer when the initiation of systemic corticosteroids was delayed for 1 day (Table 4). It means later systemic corticosteroids use might prolong the duration of active stage SCAR, and it would take more time for SCAR patients to reach stable stage (no new lesions). Moreover, one-day delay of the systemic corticosteroids use would increase 19.2% of maximum BSA or BSA detachment (Table 4). In contrast, IVIG treatment did not statistically affect the primary outcomes of both the disease progression and severity. Among all 173 SCAR patients, none of them died during their stay in hospital, and only two DRESS patients (3.5%), four SJS/TEN patients (4.2%) and no AGEP patient died in the first three months after discharge. Both two DRESS patients died of lung infection. Three SJS/TEN patients died of multiple organ dysfunction syndrome, and one SJS/TEN patients died of lactic acidosis. For mortality analysis, no statistical difference was revealed between early and delayed systemic corticosteroids use (odds ratio [OR]: 1.01, 95% confidence interval [CI]: 0.95~1.08) (Table 5).
Prognostic factors of SCAR
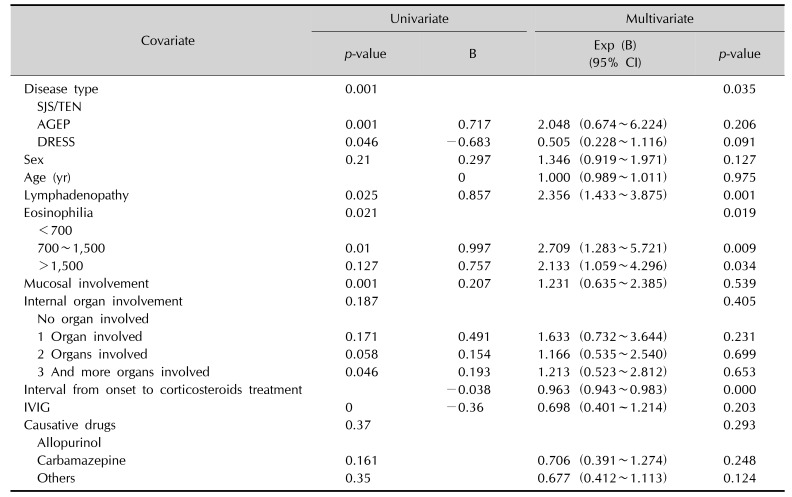
Following risk factors were included in the regression model to analyze their associations with SCAR: disease type, age, sex, lymphadenopathy, eosinophilia, mucosal involvement, internal organ involvement, interval from onset to standard treatment with adequate corticosteroids, combination therapy with IVIG, and causative drugs (Table 6). Multivariate analysis showed disease type (p=0.035), lymphadenopathy (p=0.001), eosinophilia (p=0.019) and interval from onset to standard treatment with adequate corticosteroids (p=0.000) were the independent risk factors for the prognosis of SCAR. Patients with lymphadenopathy had longer time for 50% lesions' withdrawal than those with no lymphadenopathy (OR: 2.356, 95% CI: 1.433~3.875). Moreover, when we categorized eosinophilia into three groups: moderate (<700), high (700~1,500) and higher (>1,500), high levels of eosinophilia proved to be a poor prognosis factor of SCAR, with 2-fold higher risks of longer lesions' withdrawal time (high, OR: 2.709, 95% CI: 1.283~5.721; higher, OR: 2.133, 95% CI: 1.059~4.296), compared with moderate eosinophilia level. Furthermore, interval from onset to standard treatment with adequate corticosteroids was proved to be a protective factor for the prognosis of SCAR (OR: 0.963, 95% CI: 0.943~0.983). However, mucosal involvement, internal organ involvement, co-treatment with IVIG and SCAR causative drug types were not independent prognostic factors for SCAR.
DISCUSSION
Previous studies showed conflicting results about the incidence of SCAR in different genders. In our study, DRESS occurred more common in male than female. It might be due to the fact that 40.4% DRESS cases had underlying hyperuricemia or gout, which is much more prevalent in men as well11. Whereas in SJS/TEN and AGEP, infection (28.1% for SJS/TEN and 45.0% for AGEP) was the most common underlying disease, which was consistent with previous study12.
According to our data, internal organ involvement (98%), facial edema (86%), eosinophilia (77%), high fever (75%), leukocytosis (63%), and lymphadenopathy (63%) were characteristic for DRESS. As for SJS/TEN, the main features next to the ubiquitous exanthema were mucosal involvement (94%), internal organ involvement (89%), fever (83%), and neutrophilia (33%). As for AGEP, the main features were pustules (100%), neutrophilia (80%), leukocytosis (75%), and fever (50%). Notably, our findings revealed that 46 SJS/TEN patients (48%) had facial edema, which was quite different from the traditional concept that facial edema was the warning signal for DRESS and rarely occurred in other SCAR6. We considered that diffuse erythema on face in combination with mucosal involvement like conjunctivae or lips13 could manifest as facial edema in severe SJS/TEN cases. Additionally, 17 DRESS patients (30%) had mucosal involvement, which was similar as previous reported3. Nine SJS/TEN patients (9%) had increased peripheral eosinophil counts, which highlighted that eosinophilia could occur in SCAR other than DRESS14. Some studies even reported that eosinophilia was associated with poor SCAR outcomes151617. Higher percentage of lymphadenopathy in DRESS (63%) than other SCAR was similar to previous studies, which would be explained by the potential activation of virus infections, such as Epstein-Barr virus, cytomegalovirus or human herpesvirus 6 in DRESS181920. Six AGEP (30%) had internal organ involvement, which was similar to previous studies that AGEP-specific hepatitis, nephritis or pneumonia were rare but sometimes occurred2122. Thus, systemic investigations were recommended for all SCAR types.
Over the past few decades, important progress has been made in understanding the pathogenesis of SJS/TEN, especially the role of human leukocyte antigen (HLA) alleles2324. Antiepileptic agents (phenobarbital, carbamazepine, phenytoin, and lamotrigine), minocycline, allopurinol, dapsone, and sulfonamides are the most frequently reported causative drugs of DRESS2526. In our study, the most common culprit drug for DRESS was allopurinol. HLA-B *58:01 has been reported to be associated with allopurinol-induced SCAR27. As for carbamazepine, the leading causative drug for SJS/TEN in our study, HLA-B *15:02 was responsible for carbamazepine-induced SJS/TEN28, and HLA-A *31:01 showed a stronger correlation with carbamazepine-induced DRESS29. Antibiotics were the leading cause of AGEP in our findings, which was also in agreement with previous reports30. However, further studies are required with regard to the limited number of AGEP patients in our study. Notably, 5.3% DRESS, 8.3% SJS/TEN, and 30.0% AGEP cases were caused by traditional Chinese medicine (TCM) use. The associated TCMs were radix isatidis, propolis, scolopendra, salvianolate, sophora flavescens, berberine, paraquat, Leonurus artemisia, bezoar, berberine, notoginseng triterpenes, Cordyceps sinensis, and Platycarya strobilacea. Among those listed, only paraguat has been reported to cause TEN31, and propolis has been reported to cause fixed drug eruption32. All other TCMs were newly reported. Considering the popular application of TCM treatment in Asian cultures, connection between TCM and SCAR needs to be further clarified. In our study, there were still a small number of SCAR cases with no culprit drugs, which was in accordance with previous studies that SCAR could attribute to exposures other than medications, such as infection, foods or transplantation33.
Systemic corticosteroids have long been regarded as the mainstay treatment for SCAR. However it is still controversial how much benefit patients would get from this treatment. Some case series have concluded that the use of systemic steroids were beneficial in reducing morbidity and mortality3435, whereas others suggesting minimal or no benefit in terms of outcome363738. Some earlier observational studies even indicated an increased mortality and a higher frequency of complications for TEN patients treated with systemic steroids394041. Here, we reveal that early steroids therapy could alleviate the severity (p=0.01) and progression (p=0.000) of SCAR without influencing the mortality rate. These results suggest that early shortcourse steroids use is helpful in the initial phase management of SCAR at least in a modern well-equipped tertiary care hospital. Since more than 98.2% SCAR cases received systemic steroids, we could not demonstrate the difference of outcomes with and without systemic steroids use. Further studies with different therapy are required to answer this question.
SCARs are associated with significant morbidity, mortality, and socioeconomic costs. Predicting outcomes for each specific SCAR patient at an early stage would be extremely helpful for physicians to formulate appropriate treatment strategy. However, very few clinical researches have focused on the prognostic factors of SCAR1516174243. According to our results, lymphadenopathy and eosinophilia were associated with a poor outcome. The role of eosinophilia in the outcomes of SCAR has been reported before151617, while lymphadenopathy as a poor prognostic factor for SCAR was reported for the first time. This can be explained by the potential activation of virus infections, such as Epstein-Barr virus, cytomegalovirus or human herpesvirus 6181920.
Limitations of the study included the retrospective design and a predominance of Asian population. Since most SCAR patients in our study had received systemic corticosteroids in combination with IVIG, further case-control studies with larger sample size are required for more detailed research. In addition, there have been no universal rules that could determine the causative drug of SCAR with certainty, and the rule used in this study is imperfect as well. Moreover, the long-term follow-up of SCAR patients post-discharge was lacking. However, due to the fact that the ultimate prospective blinded study needed to provide a more definitive answer to the questions about steroid use in SCAR management is extremely difficult to do, our study is of significance in guiding clinical practice. In conclusion, allopurinol, carbamazepine, and antibiotics were the most frequent implicated drugs for DRESS, SJS/TEN, and AGEP respectively. Hyperuricemia or gout was the most frequent cause of administration in DRESS, and infection was that in SJS/TEN and AGEP. Selection and prescription of those drugs should be more cautiously. Additionally, early initiation of steroids might help prevent the progression of skin lesions and decrease the severity of skin lesions or skin detachment, but had no correlation with mortality. Lymphadenopathy and eosinophilia were the independent poor prognostic factors of SCAR. For SCAR patients with lymphadenopathy and eosinophilia, physicians may consider taking a more aggressive therapeutic approach.
 XML Download
XML Download