

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
MATERIALS AND METHODS
Objective assessments
Subjective assessments
Voting and consensus
RESULTS
Moderate and severe AD
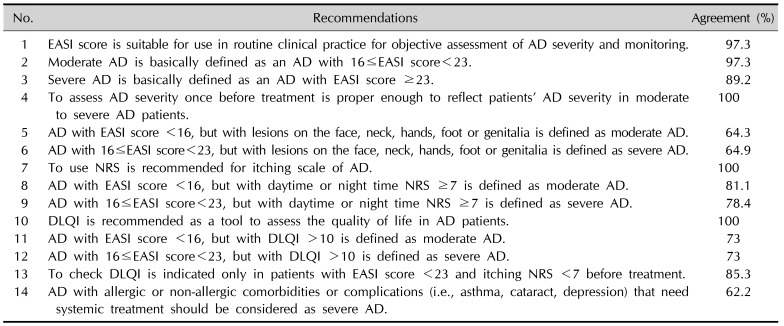
1. Korean AD experts agreed to adopt the EASI to assess and monitor AD severity in routine clinical practice.
2. Our committee members agreed that moderate AD should be basically defined as an AD with 16≤EASI score<23.
3. KADA members agreed that severe AD should be basically defined as an AD with EASI ≥23.
4. AD lesions wax and wane. However, because most patients with moderate to severe AD tend to be persistent in their lesions, Korean AD experts agreed that single static assessment of the EASI score before treatment could properly reflect patients' AD severity in moderate to severe AD patients.
5. The EASI score has a limitation to reflect the severity of several exposed areas such as hand, foot, and genitalia because it gives weight to the extent of certain areas. These lesion locations are directly related to social and functional impairment and low QoL. Thus, they should be separately assessed2324. Large number of committee members agreed that AD with EASI score <16 but with lesions on the face, neck, hands, foot, or genitalia is defined as severe AD, although this was not included in the consensus criteria. These locations are very frequently affected in AD. The presence of lesions only in these locations did not seem to be enough to upstage the disease severity. Because there has been no validated assessment tool that reflects disease severity in these specific area so far. Thus, more validated tools to assess AD severity in critically QoL-related areas needs to be developed in the future.
6. Consistently, the questionnaire that AD with 16≤EASI score<23 but with lesions on face, neck, hands, foot, or genitalia should be defined as severe AD failed to reach an agreement.
7. Korean AD experts agreed that pruritus scale should be included for assessment of AD severity and that pruritus NRS should be adopted as a pruritus scale.
8. KADA committee reached an agreement that AD with EASI<16 but with severe pruritus (daytime or nighttime NRS≥7) should be considered as moderate AD and that such patients should be actively engaged in systemic immunomodulatory treatment.
9. In the same respect, they agreed that AD with 16≤EASI score<23, but with daytime or night time NRS>7 should be defined as severe AD.
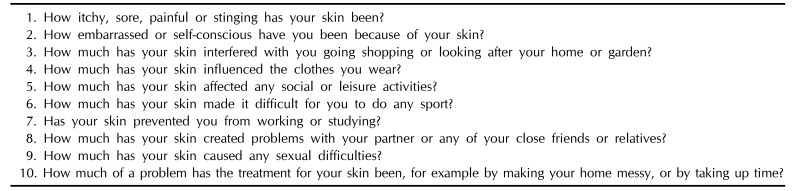
10. Korean AD experts reached a consensus that DLQI should be recommended as a tool to assess QoL of patients with AD.
11. KADA agreed that patients with DLQI >10 should be considered as at least moderate AD even if EASI score was less than 16.
12. They also agreed that AD with DLQI >10 should be considered as severe AD even if EASI score was between 16 and 23.
13. It is not necessary to check DLQI in all typical moderate to severe AD patients. DLQI should be checked in patients with EASI score <16 and itching NRS ≤7. However, for those with low QoL, other therapeutic options should be considered to improve their life quality. For AD with 16≤EASI score<23 and itching NRS ≤7, but with low QoL, DLQI also should be checked. Of all participants, 85.3% agreed that single static measurement for DLQI before treatment would be optimal for defining moderate to severe AD.
14. AD severity usually increases as they have more comorbidity such as asthma. Patients with ocular problem cannot use proper amount of topical steroid although they might have severer clinical manifestation. Psychologic comorbidities such as depression can decrease treatment compliance25. Obsessive behavior can aggravate AD severity by vicious scratching cycle26. However, Korean AD experts failed to reach a consensus on whether AD patients with allergic or non-allergic comorbidities or complications that need systemic treatment should be considered as severe AD. The definition of moderate and severe AD were made on the basis of the agreement above and described in Table 3.
Treatment-refractory AD and recurrent AD
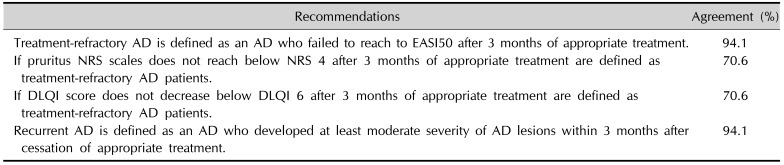
1. Refractory AD should be defined for patients with treatment refractoriness and patients who have not reached EASI 50 after three months of appropriate treatment are defined as treatment-refractory AD patients.
2. If pruritus NRS scales do not reach below NRS <4 after three months of appropriate treatment, such patients should be defined as treatment-refractory AD patients.
3. If DLQI score does not decrease to be below 6 after three months of appropriate treatment, patients should be defined as treatment-refractory AD patients.
4. If patients with AD responded well to treatment, but developed at least moderate severity of AD lesions within three months after cessation of systemic or topical immunomodulatory treatment, such patients should be defined as recurrent AD patients.


 XML Download
XML Download