

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic hand eczema (CHE) is an inflammation of hand skin that persists for more than three months. CHE is a common inflammatory skin condition that has a significant and negative impact on the affected individual and society1. The lifetime prevalence of CHE in the general population is approximately 15%, with 5% to 7% developing severe CHE23. Mild cases of CHE are typically managed with emollients and topical steroids4. On the other hand, severe CHE can be debilitating because it is often refractory to emollients and topical steroids. There are a few treatment options available for patients who do not respond adequately to topical corticosteroids; however, there is limited evidence from clinical trials on their efficacy. Alitretinoin (9-cis retinoic acid) is a newly developed retinoid with anti-inflammatory properties that received its first national regulatory approval in the UK and recently licensed by the USA Food and Drug Administration as a systemic agent for severe CHE refractory to topical corticosteroid therapy56. Although there have been many studies on the epidemiology of CHE, most of these studies have focused on patients between the ages of 10 and 60 years, with limited data on elderly patients. With increasing adult lifespans, the proportion of the elderly population can be expected to increase, along with a concomitant increase in the incidence of CHE in the elderly. In addition, due to age-associated changes in the skin barrier, the risk of contact dermatitis is likely to increase7. Therefore, there is an emerging need to study CHE in the elderly population. Although alitretinoin has been approved for the treatment of CHE, and several studies have demonstrated its effectiveness in CHE489101112, there is limited data regarding its safety and efficacy in elderly patients. In the present study, we considered that the elderly, a group predisposed to fragile skin and easy bruising, may experience unacceptable side effects from long-term maintenance with potent topical steroids. Alitretinoin may be particularly helpful in this patient population. Thus, the purpose of this study was to investigate the efficacy and safety of oral alitretinoin in elderly patients with CHE in Korea.
Go to : 
MATERIALS AND METHODS
Study design
This retrospective study was conducted in the Department of Dermatology at the Veterans Health Service Medical Center and was approved and monitored by the Institutional Review Board (IRB) of the Veterans Health Service Medical Center, Korea (IRB no. 2018-02-016). CHE was defined as hand eczema that had persisted for at least three months. Patients who were diagnosed with moderate to severe CHE refractory to topical steroid treatment were included in this study. We reviewed the medical records of 46 CHE patients over 60 years old who were treated with alitretinoin between June 2016 and July 2018. Baseline severity was classified into five categories (clear, almost clear, mild, moderate, and severe) according to the Physician's global assessment (PGA)4. Laboratory monitoring was performed for all patients while they were being treated with alitretinoin. Blood lipids, thyroid function, and liver function parameters were used to identify laboratory abnormalities. Eighteen patients with mild hypertriglyceridemia were included in this study and they were carefully monitored for dyslipidemia. One patient who had undergone a thyroidectomy due to thyroid cancer was included in this study. She was treated with alitretinoin during continuous follow-up with regular endocrinology consultation. The recommended start and maintenance dose of alitretinoin was 30 mg/d. If adverse events occurred, a dose reduction to 10 mg/d was allowed. Patients were also permitted to use medium potency topical corticosteroids and emollients while being treated with alitretinoin.
Clinical assessment of efficacy and safety
A medical record review was performed retrospectively utilizing clinical photography. We also investigated treatment characteristics, including prescription period, treatment effectiveness, side effects, and laboratory abnormalities. Treatment efficacy was evaluated retrospectively eight weeks after initiation of treatment according to PGA score, the primary efficacy parameter. A response was defined as a PGA assessment of either “clear” or “almost clear”. Laboratory tests (complete blood cell count, fasting blood chemistry, lipid profile and thyroid function test) were performed before initiation of treatment and after 8 weeks of treatment. Triglyceride concentrations were categorized as lower than 150 mg/dl (normal), 150 to lower than 499 mg/dl (mild hypertriglyceridemia), 500 to lower than 886 mg/dl (moderate hypertriglyceridemia), 886 mg/dl or higher (severe hypertriglyceridemia). Normal low density lipoprotein cholesterol (LDL-C) concentrations were defined as lower than 100 mg/dl13.
Statistical analysis
Data from all available patients were analyzed descriptively. Response rates according to baseline severity and types of hand eczema were analyzed using Fisher's exact test. The statistics program IBM SPSS Statistics ver. 18.0 (IBM Corp., Armonk, NY, USA) was used to analyze data. A p<0.05 was considered statistically significant.
Go to :
RESULTS
Patients
A total of 46 patients aged 60 or older with CHE were included in this study. Among the 46 patients involved in the study, 41 were male and 5 were female. The mean age was 71.0±5.1 years. Patient demographics and characteristics are shown in Table 1. Patients were classified into hyperkeratotic, vesicular (pompholyx), or fingertip hand eczema groups according to the German guidelines14. In total, 71.7% (33/46) of patients presented with hyperkeratotic type hand eczema. Ten patients (21.7%) exhibited vesicular type hand eczema and four patients (8.7%) exhibited fingertip type CHE. One patient had both hyperkeratotic and vesicular type hand eczema. According to the baseline PGA score, 33 patients (71.7%) were classified as moderate and 13 patients (28.3%) were classified as severe.
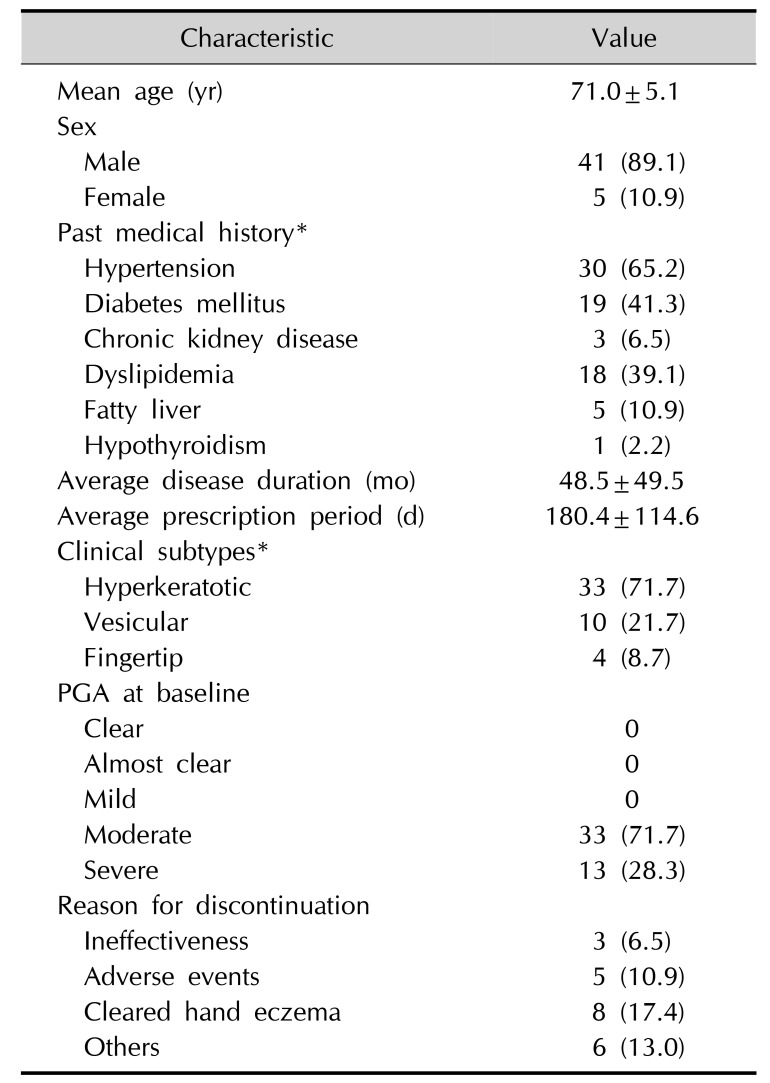
Table 1
Patient demographics
![]()
Efficacy
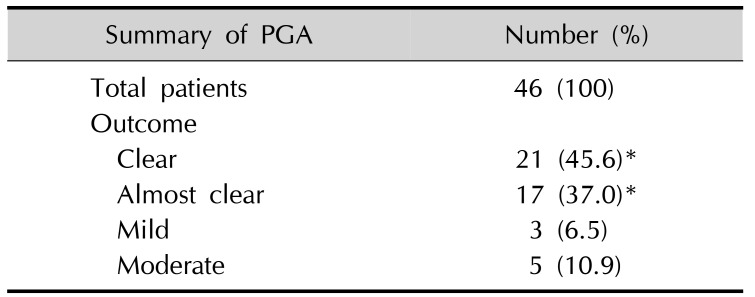
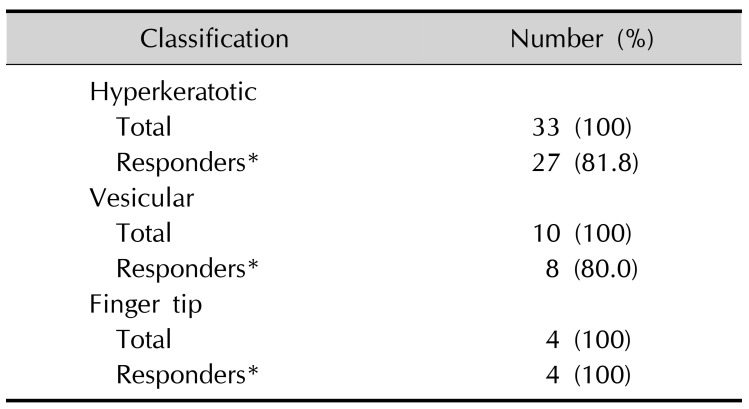
The average treatment period was 180.4±114.6 days. Among a total of 46 patients, 38 (82.6%) responded to treatment, with PGA ratings of ‘clear’ or ‘almost clear’ (Table 2). According to baseline severity (Fig. 1), patients with moderate CHE (84.8%, 28/33) exhibited better clinical improvement than those with severe CHE (76.9%, 10/13), although the difference was not statistically significant (p=0.6689). With respect to CHE type (Table 3), the response rate was highest in the fingertip type (100%, 4/4), followed by hyperkeratotic (81.8%, 27/33) and vesicular types (80.0%, 8/10). However, the response rate to alitretinoin according to CHE type was not statistically significant (p=1). Eight patients (17.4%) discontinued alitretinoin treatment because of cleared HE (clear/almost clear). Three patients (6.5%) stopped treatment because of ineffectiveness.
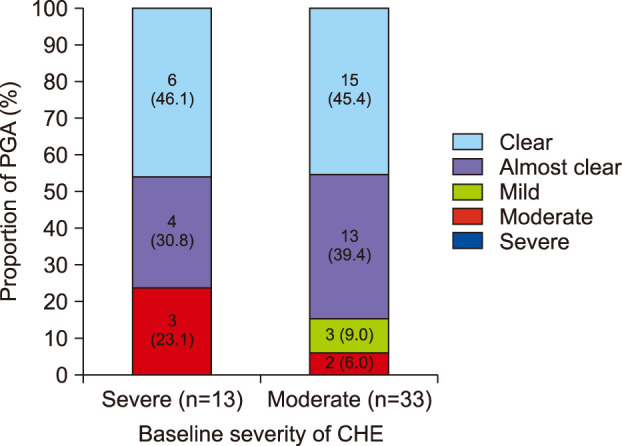 | Fig. 1Evaluation of physician's global assessment (PGA) according to severity of chronic hand eczema (CHE) at baseline.
|
Table 2
Summary of PGA after alitretinoin treatment
| Summary of PGA | Number (%) |
|---|---|
| Total patients | 46 (100) |
| Outcome | |
| Clear | 21 (45.6)* |
| Almost clear | 17 (37.0)* |
| Mild | 3 (6.5) |
| Moderate | 5 (10.9) |
![]()
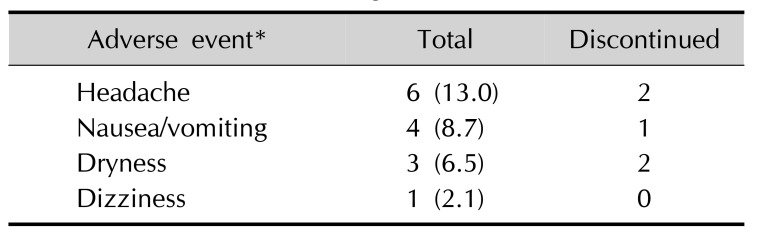
Safety
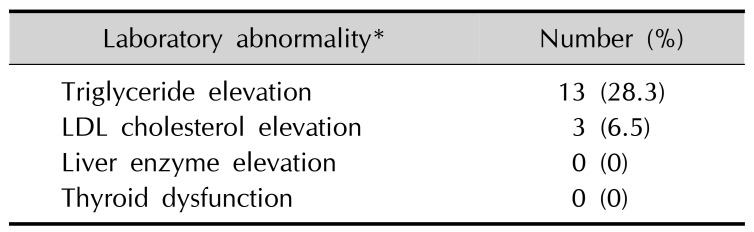
A total of 13 patients experienced an adverse event (28.3%, 13/46). Adverse events resulted in discontinuation of therapy in five patients (10.9%, 5/46), which consisted of headache (4.3%, 2/46), xerosis (4.3%, 2/46), and gastrointestinal (GI) symptoms (2.2%, 1/46) (Table 4). Abnormalities in laboratory tests were limited to typical retinoid effects and were observed in 13 patients (Table 5), all of which exhibited an elevated triglyceride level (28.3%, 13/46), with three of them also exhibiting an elevated LDL-C level range from 46 to 51 mg/dl above their premeasured baseline. In eight patients with a normal triglyceride level at baseline, mild hypertriglyceridemia was observed after alitretinoin treatment. Moderate hypertriglyceridemia was observed in one patient who had a normal triglyceride level at baseline. Four patients with mild hypertriglyceridemia at baseline exhibited an elevated triglyceride level from 240 up to 340 mg/dl above their premeasured baseline. There were no instances of liver enzyme elevation or thyroid dysfunction.
Go to :
DISCUSSION
The efficacy and side effects of alitretinoin have been studied in several large, well-designed trials (Table 6)4911. According to a meta-analysis based on these studies, alitretinoin was well tolerated and showed good efficacy in treatment of CHE15. Although many of these studies have demonstrated a high therapeutic efficacy of alitretinoin in CHE, data on the efficacy and safety of alitretinoin in the elderly is lacking. Indeed, the mean ages of patients in previous studies on alitretinoin have typically been in the 40s to 50s, while the average age in this study was 71 years46111215.
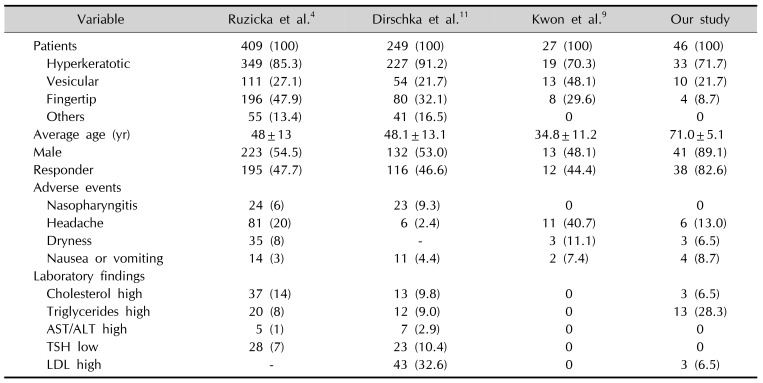
Table 6
Comparison of clinical trials of alitretinoin treatment for chronic hand eczema
| Variable | Ruzicka et al.4 | Dirschka et al.11 | Kwon et al.9 | Our study |
|---|---|---|---|---|
| Patients | 409 (100) | 249 (100) | 27 (100) | 46 (100) |
| Hyperkeratotic | 349 (85.3) | 227 (91.2) | 19 (70.3) | 33 (71.7) |
| Vesicular | 111 (27.1) | 54 (21.7) | 13 (48.1) | 10 (21.7) |
| Fingertip | 196 (47.9) | 80 (32.1) | 8 (29.6) | 4 (8.7) |
| Others | 55 (13.4) | 41 (16.5) | 0 | 0 |
| Average age (yr) | 48±13 | 48.1±13.1 | 34.8±11.2 | 71.0±5.1 |
| Male | 223 (54.5) | 132 (53.0) | 13 (48.1) | 41 (89.1) |
| Responder | 195 (47.7) | 116 (46.6) | 12 (44.4) | 38 (82.6) |
| Adverse events | ||||
| Nasopharyngitis | 24 (6) | 23 (9.3) | 0 | 0 |
| Headache | 81 (20) | 6 (2.4) | 11 (40.7) | 6 (13.0) |
| Dryness | 35 (8) | - | 3 (11.1) | 3 (6.5) |
| Nausea or vomiting | 14 (3) | 11 (4.4) | 2 (7.4) | 4 (8.7) |
| Laboratory findings | ||||
| Cholesterol high | 37 (14) | 13 (9.8) | 0 | 3 (6.5) |
| Triglycerides high | 20 (8) | 12 (9.0) | 0 | 13 (28.3) |
| AST/ALT high | 5 (1) | 7 (2.9) | 0 | 0 |
| TSH low | 28 (7) | 23 (10.4) | 0 | 0 |
| LDL high | - | 43 (32.6) | 0 | 3 (6.5) |
![]()
In our study of 46 patients, 38 (82.6%) responded to treatment with alitretinoin, which was almost twice the response rate of previous studies45911. We explain the superior effectiveness of alitretinoin observed in our study as follows. First, compared with previous studies, the mean age of the patients included in this study was 20 to 30 years older, and most patients were male. As these were the most significant differences between our study and previous studies, they may be at least partially associated with the difference in efficacy. For example, polypharmacy and physiological changes to liver and kidney function, which are commonly seen in elderly patients, might affect alitretinoin metabolism, thereby increasing its efficacy. Although alitretinoin does not exhibit increased efficacy with weight-adjusted dosing, it is possible that decreased lean body mass and increased body fat mass associated with aging may have affected its efficacy16. Second, alitretinoin is an oral agent, and drug adherence is reported to be higher with oral agents than with topical agents in the elderly because it is easier to access regularly1718. Thus, the higher efficacy observed in elderly CHE patients may have been due to better medication adherence. This result is especially important in the context of elderly patients who, as opposed to oral medications, exhibit a relatively low adherence to topical treatment compared with younger patients.
The adverse events of alitretinoin observed in our study were consistent with the well-known class effects of oral retinoids and RXR-agonists, including headache, GI symptoms, mucocutaneous events, dizziness, and hyperlipidemia (Table 4, 5). Six patients experienced headaches (6/46, 13.0%), with two patients discontinuing treatment as a result. However, when these patients resumed treatment with alitretinoin after their headaches had subsided, they no longer complained of the same adverse event. Two others showed improvement of headache without taking analgesics. Compared with the study conducted by Kwon et al.9, which included patients in the youngest age group among previous clinical trials, headaches and mucocutaneous symptom occurred less frequently, however, GI symptoms occurred more in our patients. The patients included in our study were also taking multiple drugs and their medications often included anti-inflammatory drugs, such as NSAIDs. Use of such analgesics by our patients for treatment of unrelated conditions, such as osteoarthritis may have obscured headache incidence while exacerbating GI symptoms. Therefore, when prescribing alitretinoin in elderly patients, it may be important to emphasize that alitretinoin should be taken with food not only to increase efficacy, but also to reduce GI discomfort.
Laboratory abnormalities were frequently observed in our patients, but were limited to dyslipidemia. Specifically, baseline dyslipidemia was observed in 18 (39.1%) of the patients included in our study, and was newly developed or worsened in 14 patients (30.4%). The incidence of dyslipidemia was considerably higher than that seen in previous studies where the mean age was in the late 40s, suggesting that lipid profiles should be monitored more closely in elderly patients being treated with alitretinoin. In 2015, after analyzing clinical data from several previous studies461012, Schmith et al.19 conducted five hundred clinical trial simulations to evaluate the efficacy and safety of alitretinoin treatment. The results of that study showed that elderly patients experience higher efficacy, faster response, and increased probability of hypertriglyceridemia in response to treatment with alitretinoin, which was consistent with the results of our study. Therefore, clinicians should consider utilizing a shorter treatment duration with alitretinoin in elderly patients to avoid the risk of hypertriglyceridemia.
Prescribing medication for elderly patients has several challenges. Pharmacologically, drug absorption through the GI tract decreases with increasing age. However, while hepatic metabolism and glomerular filtration rates also decrease with increasing age, drug bioavailability increases20. In addition, multi-drug regimens and multiple medical problems, which are commonly seen in the geriatric population, expose patients to an increased risk of adverse effects of drug-drug interactions20. Thus, the suitability of systemic alitretinoin treatment in elderly patients is a potential concern. The patients included in this study were all aged 60 years or older, and thus our results suggest that it is safe to use alitretinoin in the elderly.
This study had several limitations. The first and most significant limitation was the retrospective study design, which precluded standardization of regular follow-up, laboratory monitoring, and treatment duration. A second limitation of this study was that the assessment of disease severity was made using only the PGA score. However, a previous study demonstrated that there is good agreement between PGA score and modified total lesion symptom score9. Therefore, we considered that the assessment of severity through PGA score alone should have adequately reflected the severity of the actual disease. Third, our study consisted of a relatively small sample size compared to previous studies. Nevertheless, this study represents the first clinical trial to evaluate the efficacy and safety of alitretinoin treatment in elderly patients over 60 years of age. Additional studies may be needed to confirm the efficacy and side effects of alitretinoin treatment in elderly patients. In conclusion, the results of our study were consistent with previous clinical trials and demonstrated that oral alitretinoin leads to a clinically significant improvement in disease status in elderly patients with moderate to severe CHE refractory to topical corticosteroids. Therefore, alitretinoin should be considered as an effective and safe option for the treatment of moderate to severe CHE in the elderly.
Go to :
 XML Download
XML Download