

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Glaucoma is the second-leading cause of irreversible visual impairment worldwide, affecting more than 70 million people.12 Primary angle closure glaucoma accounts for about a quarter of worldwide glaucoma and, in East Asian people, is a major form of glaucoma.1345 Despite its importance, there is a paucity of data addressing nationwide, population-based incidence estimates as well as prevalence estimates regarding primary angle closure glaucoma.567 Incidence data is meaningful in assessing the number of symptomatic patients, that is the number of patients with acute angle closure glaucoma (AACG), which is essential for estimating socioeconomic costs and planning healthcare policy as well as investigating pathophysiology.
Korea is an ideal country for studies investigating nationwide incidence rate of AACG. As the all Korean residents (about 50 million people) are obligatorily registered under the National Health Insurance (NHI) system, all healthcare utilization are recorded including diagnosis of AACG and all received prescriptions and treatments related to AACG.8910111213 Therefore, we conducted this nationwide, population-based study to estimate the incidence rate of AACG using the national health claim database from the Korean NHI system.
METHODS
Study population
We used data from the National Health Insurance Service (NHIS) database which has covered the entire Korean population of 50 million individuals from 2009 to 2015. The NHI scheme started in Korea in 1977 and achieved universal coverage of the population by 198914; therefore, all Koreans are covered by the NHI. The database contains all information regarding health care utilization for approximately 50 million Koreans, including claims for diagnoses, procedures, prescription records, demographic information, and direct medical costs. Diagnoses were coded according to the International Classification of Diseases, 10th edition (ICD-10) for the Korean healthcare system. The validation study showed the overall positive predictive value of the diagnosis to be 83.4% by comparing the diagnoses in the database with those in patient medical records.15 Detailed information regarding the NHIS and the database has been reported elsewhere.8910111213 The NHIS database is open to researchers whose study protocols are approved by the official review committee.
Eligible criteria for patients with incident AACG
We identified all AACG cases claimed during 2011–2015 according to the first AACG diagnostic code (H40.20) in the ICD-10. We defined the index date as the earliest claim related to the AACG diagnostic code. To define the incident AACG cases and exclude prevalent AACG cases and cases having other glaucoma subtypes before diagnosed as AACG, we excluded cases having any following diagnoses: primary open angle glaucoma (H40.1), angle closure glaucoma (H40.2), secondary glaucoma due to trauma (H40.3), uveitic glaucoma (H40.4), pseudoexfoliation glaucoma (H40.5), secondary glaucoma due to drugs (H40.6), other glaucoma (H40.8), unspecified glaucoma (H40.9), glaucoma in diseases classified elsewhere (H42), and congenital glaucoma (Q15.0). We defined these eligible individuals as a presumed incident AACG case based on their diagnosis only. Of these presumed AACG cases, to validate the diagnosis of AACG, we included cases only when the case underwent laser iridectomy or cataract surgery during the period from 2 weeks before to 4 weeks after the index date. Then, we defined these cases as the incident AACG cases. Of these, we included individuals aged 20 years or older on the index date in the statistical analysis.
Statistical analysis
First, we calculated crude incidence rates for each study year from 2011 to 2015 in accordance with 5-year age groups and gender using the mid-year population of each year based on the Resident Registration Data in Korea (available at: http://kosis.kr; accessed July 1, 2019). Then, we applied the direct standardization method to each estimated crude incidence rate from 2011 to 2015 for age group and gender in reference to the 2015 Census Population as the standard population (available at: http://kosis.kr; accessed July 1, 2019). Using these standardized incidence rates from 2011 to 2015, we lastly calculated the average standardized annual incidence rates during the 5-year study period (2011–2015). We presented incidence rates in per 1,000,000 person-years throughout the present study. We also calculated average incidence rates in population aged 30 years or over and in those aged 40 years or over. We determined 95% confidence interval (CI) of incidence rates based on the Poisson distribution. We also estimated the female-to-male ratios in each age group. In addition, we also provided incidence estimates from the presumed incident AACG cases to compare the previous studies that defined AACG cases by the use of diagnosis only from claims database. All statistical analyses were performed using SAS version 9.3 (SAS Institute Inc., Cary, NC, USA) and R version 3.1.0 (The R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org).
RESULTS
We identified 15,094 (9,899 women, 65.6%) presumed incident AACG cases, and of these, we included a total of 11,049 patients (8,022 women, 72.6%) who had laser iridectomy or cataract surgery during the period from 2 weeks before to 4 weeks after the index date in the analysis as incident AACG cases. Of these, we excluded 6 cases aged under 20 years old during the 5-year study period, and therefore, a total of 11,043 patients aged ≥ 20 years old (8,020 women, 72.6%) were included in the analysis of incidence rate. The number of AACG cases aged ≥ 20 years old who identified in 2011, 2012, 2013, 2014, and 2015 was 1,921, 2,131, 2,131, 2,461, and 2,399, respectively. The corresponding standardized incidence rates were 56.57 (95% CI, 54.22–58.91), 60.21 (95% CI, 57.79–62.62), 58.00 (95% CI, 55.63–60.38), 64.45 (95% CI, 61.95–66.95), and 60.52 (95% CI, 58.10–62.94), respectively (Table 1). We provide detailed data regarding the number of incident AACG cases, estimated crude incidence rate, and the estimated standardized incidence rates according to age groups and gender in each study year from 2011 to 2015 in the Supplementary Tables 1, 2, 3, 4, 5, respectively.
Table 1
Number of cases, crude incidence rates, standardized number of cases, and standardized incidence rates of AACG in each year from 2011 to 2015
AACG = acute angle closure glaucoma, CI = confidence interval, F:M ratio = female to male ratio.
aWe standardized the crude incidence rates in each year using the 2015 Census Data as a reference population.
![]()
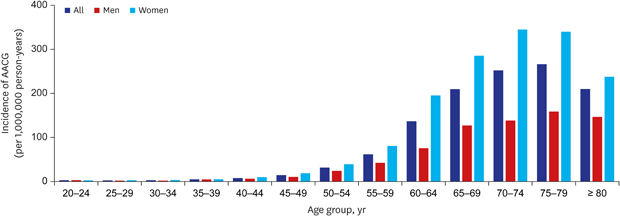
The average standardized incidence rate during the 5-year study period from 2011 to 2015 was 59.95 (95% CI, 58.87–61.03). The incidence rates increased sharply as age of population increased and peaked at individuals aged 75–79 years; in men, those peaked at the same age group, however, in women, those peaked at individuals aged 70–74 years (Fig. 1), which were similar in each 5 years. Women has a 2.56 folds higher incidence rate (85.84 [95% CI, 84.03–87.66]) than men (33.48 [95% CI, 32.33–34.62]), which was observed across most age groups. Table 2 shows detailed numbers and average standardized incidence rates according to age groups and gender during the 5-year study period. In addition, Table 2 also presents the average incidence rates in population aged 30 years or over and in those aged 40 years or over.
 | Fig. 1Average ang- and gender-standardized incidence rate (per 1,000,000 person-years) of acute angle closure glaucoma in Korea between 2011 and 2015.AACG = acute angle closure glaucoma.
|
Table 2
Average standardized incidence rate of AACG during 2011–2015 in reference to the 2015 Census Data
![]()
In addition, the average standard incidence rate in reference to the presumed incident AACG cases was 80.29 (95% CI, 79.04–81.54). We provide detailed data regarding the number of presumed incident AACG cases, estimated crude incidence rate, and the estimated standardized incidence rates according to age groups and gender of the presumed incident AACG cases in the Supplementary Table 6.
DISCUSSION
We estimated the nationwide, population-based incidence rate of AACG in Korea over a 5-year period. To our best of knowledge, this study is the largest nationwide, population-based study of the AACG incidence rate to date. We could minimize selection bias and omission of the AACG cases by using the database covering the entire Korean population, and therefore, the present results provide reliable, detailed data regarding the AACG incidence according to age groups and gender. Throughout the 5-year study period, the incidence rate of AACG among individuals aged 20 years or older was 59.95 per 1,000,000 person-years in the present study, which is similar to or somewhat lower than the reported rates from Asian populations and is slightly higher than those from Western populations. In old literature, the standardized incidence rates for Finland, Croatia, Israel, Thailand, and Japan were 47, 56, 107, 70, and 114 per 1,000,000 person-years in individuals aged ≥ 30 years old, respectively, although they were not population-based studies.161718 In Singapore, Wong et al.19 showed primary angle closure glaucoma in the population aged ≥ 40 years old according to the three common ethnic groups in East Asia using the Hospital discharge data; the rates were 122, 60, and 63 per 1,000,000 person-years in Chinese, Malay, and Indian people, respectively. After that, two prospective studies also reported similar results of AACG rates, 155 and 107 per 1,000,000 person-years, in Singapore and Hong Kong, respectively.1720 However, in Scotland, Gillan et al.5 reported quite lower incidence rates of AACG; AACG incidence rates in Scotland has continued to decrease from 46.7 per 1,000,000 person-years in 1998 to 25.0 per 1,000,000 person-years in 2008. Interestingly, Chiu et al.7 reported incidence rates of angle closure glaucoma ranged 495.4 to 635.1 per 1,000,000 people in the Taiwanese population of all ages, which was quite higher than any other rates reported in literature. Unlike the present study, they identified patients with angle closure glaucoma based only on the AACG diagnostic codes using the claims database; therefore, we additionally conducted the analysis estimating the incidence rates based only on diagnosis as Chiu et al.7 did, with a results of 80.29 per 1,000,000 person-years (Supplementary Table 6 provides detailed information). However, the rates of 80.29 per 1,000,000 person years in this additional analysis were also quite lower than that by Chiu et al.7 When identifying incident AACG cases, we excluded all cases having any other glaucoma diagnosis before they diagnosed as AACG, whereas Chiu et al.7 did not. This might be one of the reasons why Taiwanese study showed a higher incidence rate than all other previous studies as well as the present results.
Interestingly, the results of the presumed incident AACG cases shows slightly higher proportion of patients in age groups under 40 years compared to those in age groups over 40 years. The tendency is more pronounced in the younger age group. It is thought that the younger the patient with AACG diagnosis, the more likely that they would not receive treatment of laser iridectomy or cataract surgery. As we cannot review the medical records, we have no way to confirm the reason of this observed discrepancy in young ages. Possible explanations might be for the following reasons. First, young patients diagnosed with AACG might have plateau iris syndrome, which is often treated with argon laser peripheral iridoplasty or pilocarpine. Second, younger AACG patients could be associated with the use of drugs such as topiramate, which is approved as an anti-convulsant for treatment of seizure disorders and for prevention of migraine headaches, and, however, is commonly used in obesity therapeutics.21222324 Those drugs are known to cause secondary angle closure, and treated with medications. Lastly, there are possibilities of misdiagnosis in young patients with trauma or uveitis-related intraocular pressure increasement (e.g., glaucomatocyclitic crisis) as AACG. Further study is warranted to elucidate this observed discrepancy.
Unlike previous studies, we could include over 11 thousand patients with incident AACG through the 5-year study period from 50 million people in the analysis. Therefore, we could provide detailed incidence estimates according to 5-year age groups and gender in addition to the standardized incidence rate. The present study shows that the incidence rate of AACG increased exponentially with age, peaked in the 75–79 age group, and decreased in the age group over 80 years. Advanced age is a well-known risk factor for developing AACG,67171925 it might not be surprising that we found a higher incidence of AACG in Korean elderly population. However, the interesting finding is that the incidence decreases at the age of 70s after the peak incidence in the present study. Further studies are warranted. As the population rapidly ages around the world, public burden of AACG might rapidly increase and the present results might help estimating the global burden of AACG. The present study also presents that the incidence of AACG in women was 2.56 times higher than in men, and this trend was observed across all the age groups except for twenties and throughout the study period, which was concomitant with previous studies.67171925
The present study has the following limitations that should be taken into account during interpretation. First, we may have underestimated the AACG incidence in Korea. As stated, we excluded patients who had been diagnosed as other type of glaucoma before diagnosed as AACG from the incident AACG patients. In addition, we confined the incident AACG patients only who received laser iridectomy or cataract surgery in relation to AACG diagnosis. These eligible criteria might allow us to define more accurate AACG patients, but might underestimate the AACG incidence. Therefore, we also provided the incidence estimates of presumed incident AACG cases, which was defined only by diagnostic codes as the study by Chiu et al.7 Second, we identified the AACG cases using only claims data including diagnostic and treatment codes and could not validate the diagnosis of AACG through direct review of medical records, which is an inherent limitation of studies using the claim database. Lastly, lack of clinical information including intraocular pressure, axial length, anterior chamber depth, or other related factors is another limitation of the present study. Further investigation is warranted to investigate underlying risk factors and ethnic differences in incidence and prevalence of AACG.
In conclusion, the incidence rate of AACG in the Korean population 20 years of age or older were 59.95 per 1,000,000 person-years and 2.56 times higher in women. The incidence rates increase sharply with age and peaked in 70s. These results can provide better understanding of the characteristics of AAGG incidence in East Asian population.
 XML Download
XML Download