

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In Korea, the incidence of cervical cancer has decreased steadily to a rate of 9.1 per 105 in 2015, compared to 16.3 per 105 in 1999, with an estimated annual percentage change of −3.7%, but 3,582 cervical cancers were newly diagnosed in 2015 [1]. The Korean Society of Gynecologic Oncology guidelines had indicated that radical hysterectomy (RH) could be performed via either laparotomy or minimally invasive surgery (MIS) [2]. Systematic reviews of early-stage cervical cancer patients showed that laparoscopic RH (LRH)/robotic RH was associated with less blood loss, fewer postoperative complications, and longer hospital stays compared with the abdominal RH (ARH), with no significant difference in the oncologic outcomes [34]. Thus, MIS RH in early cervical cancer has been adopted as the standard approach.
Recently, the phase III Laparoscopic Approach to Cervical Cancer (LACC) trial revealed that women undergoing MIS RH for early cervical cancer had worse survival than those who received ARH [5]. The results of the LACC trial are likely to change early cervical cancer treatment guideline. However, before adopting the results of the LACC trial, we must consider several factors affecting disease recurrence in MIS RH. In January 2016, we suggested that women with early cervical cancer who underwent MIS RH may have higher rates of disease recurrence than women who received ARH [6]. In particular, laparoscopic intracorporeal colpotomy under CO2 pneumoperitoneum may carry a risk of intraperitoneal tumor spreads. Thus, the colpotomic approach in MIS RH may itself be a risk factor for disease recurrence.
Selection of optimal surgical candidates without parametrial invasion (PMI) is of paramount importance in MIS RH because occult malignant cells in the parametrial tissues can be exposed to the circulating CO2 during MIS RH, and metastatic parametrial disease is randomly located in the lateral and medial parametria in early-stage cervical cancer patients [7]. It is well known that a disruption of the cervical stromal ring on T2-weighted MRI was the strongest predictor of pathologic PMI [8]. Also, International Federation of Gynecology and Obstetrics (FIGO) stage IB–IIA cervical cancer patients (the last FIGO cervical cancer staging in 2009) who did not show clinically definite evidence of PMI may have a disruption of the hypointense cervical stromal ring on MRI (pathologic PMI, stage IIB based on the revised 2018 FIGO staging) [9]. In addition to the colpotomic approach, therefore, pathologic PMI may also be an important factor for disease recurrence in MIS RH. Thus, selection of optimal MIS RH candidates using preoperative PMI prediction criterion may reduce disease recurrence.
The aim of this study was to evaluate oncologic outcomes of MIS RH in FIGO stage IB–IIA cervical cancer patients before and after the application of PMI criterion on MRI and vaginal colpotomy (VC). In addition, risk factors associated disease recurrences after MIS RH were analyzed.
MATERIALS AND METHODS
1. Data acquisition and subgrouping
We retrospectively reviewed clinicopathologic data of 117 patients with FIGO stage IB–IIA cervical cancer treated with MIS RH between April 2006 and November 2013 at Ajou University Hospital. In these patient cohorts, we experienced intraperitoneal recurrences and laparoscopic intracorporeal colpotomy represented a prognostic factor related to disease recurrence [6]. In addition, we analyzed treatment outcomes in FIGO stage IB–IIA cervical cancer patients with a focally disrupted cervical stromal ring on MRI, using a propensity score matching study [10]. Primary chemoradiation showed comparable survival outcomes, but fewer treatment-related complications, compared to primary radical surgery. Based on our findings, 99 consecutive patients have been prospectively collected, using the PMI criterion of cervical stromal ring on MRI, and all patients received VC only (December 2013–October 2018). The clinicopathologic data were obtained from medical records following approval of the center's Institutional Review Board (AJIRB-MED-MDB-18-548). All patients were diagnosed with invasive cervical cancer including squamous cell carcinoma, adenocarcinoma, or adenosquamous cell carcinoma. Patients who had a history of primary radiotherapy, neoadjuvant chemotherapy, or chemoradiation were excluded. Patients were classified into the pre-PMI intracorporeal or VC (IVC) (n=117) and post-PMI VC groups (n=99). In the pre-PMI IVC group, PMI criterion on MRI was not used and the patients received IVC. In the post-PMI VC group, no patients had a disruption of the cervical stromal ring on MRI and received VC only.
Uterine cervical cancer staging was based on 2018 FIGO criteria using MRI [9]. In the pre-PMI IVC group, patients who had definite evidence of PMI on pelvic examination, or lymph node (LN) metastasis on pelvic MRI and positron emission tomography-computed tomography received primary chemoradiation. In the post-PMI VC group, strict MRI criterion for PMI was applied to all patients. In the post-PMI VC group, patients who had definite evidence of PMI on pelvic examination or disrupted stromal ring on MRI, or LN metastasis on pelvic MRI or positron emission tomography-computed tomography received primary chemoradiation.
2. Surgery and adjuvant therapy
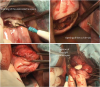
All patients underwent Piver type III RH with pelvic and/or para-aortic lymphadenectomy. In premenopausal woman, the Rowden uterine manipulator injector with the Koh colpotomizer and pneumo-occluder (CooperSurgical, Lake Forest, CA, USA) was used. In postmenopausal woman, however, the Cohen cannula in combination with a single-toothed tenaculum or 2 tenacula were used to grasp the anterior and/or posterior lip of the cervix because the uterus is usually less than 7 cm in length and perforation of the uterus may occur when the uterus is being sounded. In particular, 3 techniques for the prevention of intraoperative tumor spillage were conducted. First, closing the fallopian tubes via cautery or clipping was performed prior to the insertion of a uterine manipulator. Second, a copious irrigation of the vagina with povidone-iodine and sterile saline solution was conducted after the insertion of a uterine manipulator and before the VC. Third, the reverse Trendelenburg position were used during VC. In the case of robotic surgery, side-docking was done to manipulate the uterus more easily. Briefly, pelvic lymphadenectomy was performed, then the uterine artery, ureter, and paracervix were separated. After development of the paravesical and pararectal spaces, the uterosacral ligaments were cut with bipolar coagulation and harmonic shears as close to the pelvic sidewall as possible, and the remaining parametria and paracolpos were divided. Once the cervix and vagina were freed from their vascular and suspensory attachments, vaginal cuff was resected intracorporeally in the laparoscopic environment (Fig. 1) or the laparoscopic procedure was temporarily terminated via the vaginal route to delineate an adequate vaginal cuff margin (Fig. 2).

Fig. 2
Prevention of intraperitoneal tumor spillage using vaginal colpotomy after laparoscopic parametrectomy and dissection of paracolpos.
Adjuvant radiotherapy was given to patients who had ≥2 intermediate-risk pathological factors. Adjuvant chemoradiation using a 5-fluorouracil and cisplatin was administered to patients who had ≥1 high-risk pathological features [11]. All patients were followed at least 3 months for the first 2 years and every 6 months for the next 3 years.
3. Definition of variables
Based on MRI findings, cervical stromal ring status was classified into 2 groups. Intact cervical stromal ring was defined as partial or nearly full-thickness involvement of hyperintense cervical tumors without disrupting the hypointense stromal ring (Supplementary Fig. 1A). Disruption of cervical stromal ring was defined as focal disruption or full-thickness loss of hypointense stromal ring with nodular or irregular mass extending to the paracervix (Supplementary Fig. 1B).
Disease recurrences were classified into 3 sites, including pelvis (vaginal cuff, bladder, rectum, pelvic LN, or ovaries), extra-pelvis (para-aortic LN, lung, liver, or bone), and intraperitoneum. Intraperitoneal recurrence was defined as peritoneal carcinomatosis or disease recurrence in a dependent compartment and peritoneal surface (subhepatic/subsplenic spaces, paracolic gutters, bowel serosa, and pelvic recesses) without definite evidence of LN or distant recurrences.
4. Statistical analysis
Normality testing (Kolmogorov-Smirnov test) was performed to determine whether the data were drawn from a Gaussian distribution. Clinicopathologic characteristics and oncologic outcomes were compared between the 2 groups, with the Pearson χ2 test or the Fisher's exact test (2-tailed) for categorical data and the Student t test and the Mann-Whitney U test for continuous data according to normality. When the subject was alive at the time of analysis, or alive at the time last seen, survival time was censored. Disease-free survival (DFS) was defined as the time, in months, from the date of MIS RH to the date of relapse or censoring. DFS was estimated using the Kaplan-Meier method, and groups were compared by univariate analysis, employing the log-rank test. Based on Cox proportional hazard regression model with a backward elimination method were used to determine prognostic factors for DFS. A p-value <0.05 was considered significant. Data were analyzed using SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Table 1 shows the clinicopathologic characteristics of the pre-PMI IVC group and post-PMI VC group in FIGO stage IB–IIA cervical cancer patients. There were no differences in preoperative clinicopathologic factors between the 2 groups. However, 68 patients (58.1%) in the pre-PMI IVC group received total intracorporeal colpotomy. Ten patients (8.5%) in the pre-PMI IVC group showed a disruption of the cervical stromal ring on MRI. In contrast, no patients in the post-PMI VC group showed a disruption of the cervical stromal ring on MRI. There were no significant differences in postoperative pathologic factors including histology, tumor grade, stromal invasion, PMI, and pelvic LN metastasis between the 2 groups. However, there was a decreasing trend of tumor size on MRI (median value, 2.5 cm vs. 2.2 cm, p=0.083) and an increasing trend of an earlier FIGO stage on MRI (IB1r, 17.9% vs. 35.4%, p=0.073) in the post-PMI VC group. The rate of positive vaginal cuff margins in the pre-PMI IVC group was higher than that in the post-PMI VC group (11.1% in pre-PMI IVC group vs. 1.0% in post-PMI VC group, p=0.003). The rate of lymphovascular space invasion in the pre-PMI IVC group was higher than that in the post-PMI VC group (48.7% in the pre-PMI IVC group vs. 33.3% in the post-PMI VC group, p=0.022). The rates of disease recurrence and disease-specific mortality in the pre-PMI IVC group were higher than those in the post-PMI VC group (recurrence, 16.2% vs. 2.5%, p=0.002; death, 8.5% vs 0.0%, p=0.006). Two patients were lost to follow-up (1/117 in pre-PMI IVC group; 1/80 in post-PMI VC group).
Table 1
Comparison of clinicopathologic characteristics before and after the application of parametrial invasion criterion on magnetic resonance imaging and vaginal colpotomy in International Federation of Gynecology and Obstetrics stage IB–IIA cervical cancer patients treated with minimally invasive radical hysterectomy

Values are presented as number (%).
AC, adenocarcinoma; ASC, adenosquamous cell carcinoma; FIGO, International Federation of Gynecology and Obstetrics; IC, intracorporeal colpotomy; IVC, intracorporeal or vaginal colpotomy; LN, lymph node; LRH, laparoscopic radical hysterectomy; MD, moderately differentiated; MRI, magnetic resonance imaging; PD, poorly differentiated; PMI, parametrial invasion; RRH, robotic radical hysterectomy; SCC-Ag, squamous cell carcinoma-antigen; SCC, squamous cell carcinoma; VC, vaginal colpotomy; WD, well-differentiated.
*An enzyme-immunoassay termed CYFRA 21-1, that measures serum fragments of cytokeratin-19.
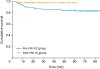
Fig. 3 shows Kaplan-Meier analysis of 2-year DFS between the pre-PMI IVC and post-PMI VC groups in FIGO stage IB–IIA cervical cancer patients. DFS are significantly different between the 2 groups (84.5% in pre-PMI IVC group vs. 98.0% in post-PMI VC group, p=0.005).
Fig. 3
Kaplan-Meier analysis of 2-year disease-free survival between the pre-PMI IVC and post-PMI VC groups in International Federation of Gynecology and Obstetrics stage IB–IIA cervical cancer patients treated with minimally invasive radical hysterectomy.
IVC, intracorporeal or vaginal colpotomy; PMI, parametrial invasion; VC, vaginal colpotomy.
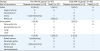
In multivariate analysis, disruption of the cervical stromal ring on MRI (hazard ratio [HR]=20.321; 95% confidence interval [CI]=4.903–84.218; p<0.001) and intracorporeal colpotomy (HR=3.059; 95% CI=1.176–7.958; p=0.022) were associated with DFS in FIGO stage IB–IIA cervical cancer patients treated with MIS RH (Table 2).
Table 2
Multivariate analysis of clinicopathologic factors for disease-free survival in patients with International Federation of Gynecology and Obstetrics stage IB–IIA cervical cancer treated with minimally invasive radical hysterectomy (n=197)

Table 3 shows the recurrence pattern and disease-specific mortality between the pre-PMI IVC and post-PMI VC groups in FIGO stage IB–IIA cervical cancer patients. Of the 10 patients with pelvic recurrence in the pre-PMI IVC group, 8 patients (80.0%) responded to additional surgery or chemoradiation and are still alive. Of the 6 patients with intraperitoneal recurrence, however, 5 patients (83.3%) showed disease progression with peritoneal carcinomatosis despite additional surgery or chemoradiation and died. Two (66.7%) of the 3 patients with distant recurrence (lung and liver) in the pre-PMI IVC group showed disease progression and died despite addition chemotherapy. In the post-PMI VC group, 2 patients who had high-risk pathologic features showed vagina (IB1r) and para-aortic LN (IB2r) recurrences. After disease recurrence, additional chemotherapy was given, and they are still alive.
Table 3
Comparison of recurrence pattern and disease-specific death before and after the application of PMI criterion on MRI and VC in International Federation of Gynecology and Obstetrics stage IB–IIA cervical cancer patients treated with minimally invasive radical hysterectomy
Values are presented as number (%).
IVC, intracorporeal or vaginal colpotomy; LN, lymph node; MRI, magnetic resonance imaging; PMI, parametrial invasion; VC, vaginal colpotomy.
*In the pre-PMI IVC group, PMI criterion was not applied, and the patients received IVC; †In the post-PMI VC group, no patients had a disruption of the cervical stromal ring on MRI and received VC only.
DISCUSSION
Several authors have suggested that CO2 pneumoperitoneum can cause several adverse peritoneal effects including peritoneal acidosis, hypoxia, decreased apoptosis, and environmental desiccation with peritoneal damage [121314]. Also, overexpression of hypoxia-inducible factor-1 alpha is correlated with cancer progression [15]. An experimental animal study showed that intraperitoneal tumor spread may be connected to accidental presentations of cancerous tumor cells to the circulating CO2 pneumoperitoneum [16]. As a consequence, these peritoneal changes could potentially result in an environment favorable for cancer cells to implant and proliferate. In our study, 8 (80.0%) of the 10 patients with pelvic recurrence in the pre-PMI IVC group responded to additional surgery or chemoradiation and are now alive. However, 5 (83.3%) of the 6 patients with intraperitoneal recurrence showed disease progression with peritoneal carcinomatosis despite additional surgery or chemoradiation and are dead.
Randomized controlled trials (RCTs) have established that MIS results in survival rates comparable to open surgery for endometrial, colonic, and gastric malignancies [171819]. In the case of early-stage disease, these tumors are organ-confined and tumor exposure during MIS rarely occurs. With regard to the resection margin in rectal cancer, however, 2 recent RCTs failed to show the non-inferiority of laparoscopic surgery to open surgery [2021]. In addition, an RCT comparing robotic radical cystectomy to open radical cystectomy showed that the open surgery group had significantly less local recurrence including peritoneal recurrence, compared to the robotic surgery group [22]. Similarly, the LACC trial showed that women undergoing MIS RH for early cervical cancer had worse survival than those who received ARH [5]. Poor oncologic outcomes of MIS in pelvic organ malignancies may result from the anatomical location of the uterine cervix, bladder, and rectum because these organs are contiguous to each other and meticulous dissection of adherent neighboring structures in pelvic organ is required. Unlike an open surgery, tumor cells can be easily exposed into the laparoscopic environment if the paracervical area is involved by metastatic tumors. Tumor exposure in MIS RH can occur during 2 surgical steps, such as parametrectomy and colpotomy. Therefore, we should make strategies to minimize or avoid tumor exposure during these procedures.
Metastatic parametrial disease can be exposed to the circulating CO2 pneumoperitoneum and pathologic PMI may be a risk factor for disease recurrence in MIS RH. In the pre-PMI IVC group, one patient with a disrupted cervical stromal ring on MRI and pathologic PMI received a colectomy 16 months after MIS RH because of intestinal obstruction; a metastatic adenocarcinoma of pericolic tissues and bowel serosa surfaces were found. This case alone cannot explain that pathologic PMI may be a risk factor for disease recurrence in MIS RH because the rates of pathologic PMI were not significantly different between the 2 groups. Thus, more extensive PMI might be associated with the disease recurrence in MIS RH, not the isolated tumor cells or micrometastasis in the parametrium. Also, the rates and extents of pathologic PMI will be decreased if more patients in the post-PMI VC group are collected. However, prognostic significance of pathologic PMI in MIS RH should be further investigated. Clinical tumor diameter has been used as a PMI prediction criterion. The reported accuracy of a rectovaginal examination for tumor diameter, however, is approximately 65% in pathologic correlation [23]. Two reports found that the rate of microscopic PMI was approximately 1% in patients with tumors smaller than 2 cm in diameter on MRI or as assessed by cone biopsy [2425]. However, a linear change in uterine cervical size were found according to parity and menopause [26]. For example, a premenopausal woman with 4-cm sized exophytic tumor and intact stromal ring on MRI did not show a pathologic PMI. On the contrary, a postmenopausal woman with an endophytic tumor 2 cm or less and disrupted stromal ring on MRI showed a pathologic PMI. Therefore, the status of the cervical stromal ring on MRI may be a simple and objective criterion for PMI and can be easily used to select optimal candidates for MIS RH, irrespective of tumor size. In our study, 7 (70.0%) of 10 patients with a disruption of cervical stromal ring on MRI had a pathologic PMI and the disease recurred in 6 patients (60.0%). Based on these results, every effort should be made to localize the tumor and select the patients with carcinoma strictly confined to the cervix preoperatively and MIS RH should be performed in optimal surgical candidates with intact cervical stromal ring on MRI.
Relapses in early cervical cancer after ARH are primarily restricted to the pelvis. Distant metastases occur in the LN, liver, and lungs. Unfortunately, several cases of intraperitoneal dissemination after laparoscopic management of cervical cancer have been reported [2728]. It is possible that intraperitoneal tumor spreads may occur when the vagina is opened and the tumor surface is exposed to the circulating CO2 during laparoscopic intracorporeal colpotomy (Fig. 1). In addition, it is often difficult to determine the optimal length of the vaginal resection margin during laparoscopic intracorporeal colpotomy. Some authors have also suggested that vaginal cuff incision and closure after CO2 evacuation via vaginal route can determine the optimal vaginal resection margin and minimize tumor spillage [29]. Therefore, MIS RH using VC should be performed because tumor spillage under CO2 pneumoperitoneum during laparoscopic intracorporeal colpotomy may contribute to tumor recurrence in unusual intraperitoneal sites.
The Rowden uterine manipulator injector with the Koh colpotomizer and pneumo-occluder confer many benefits when performing MIS RH. The manipulator allows good exposure to the paravesical and pararectal spaces around the cervix and thus a faster and safer procedure. By lateralizing the uterus and increasing the distance between the cervix and ureter, the manipulator facilitates a perpendicular dissection of the uterine artery and allow safer dissection around the cervix. However, several authors have raised concerns that the use of a uterine manipulator may cause tumor fragmentation and artificial displacement of tumor cells to fallopian tubes [3031]. Moreover, the steep Trendelenburg position during intracorporeal colpotomy may lead to the possibility of increasing the intraperitoneal tumor spread through colpotomy site. Thus, 3 techniques for the prevention of intraoperative tumor spillage can be suggested. First, closing the fallopian tubes via cautery or clipping prior to the insertion of a uterine manipulator can prevent the spread of tumor cells into the intraperitoneal cavity. Second, a copious irrigation of the vagina with povidone-iodine and sterile saline solution after the insertion of a uterine manipulator and before the VC can eradicate or minimize the fragmented tumor cells in the vagina. Third, the reverse Trendelenburg position during VC can help prevent inadvertent exposure of tumor cells into the intraperitoneal cavity.
Although the rates of PMI were not significantly different between the 2 groups, there was a decreasing trend of tumor size on MRI (2.5 cm vs. 2.2 cm, p=0.083) and an increasing trend of an earlier FIGO stage on MRI (IB1r, 17.9% vs. 35.4%, p=0.073) in the post-PMI VC group. Also, the pathologic tumor size was significantly different between the 2 groups (mean value, 2.9 cm vs. 2.4 cm; p=0.022). Thus, the statistical significance of difference in tumor size, pathologic PMI, and FIGO stage between the 2 groups will be increased if more patients in the post-PMI VC group are collected. Also, there was a decreasing trend of serum squamous cell carcinoma antigen (SCC-Ag) level (mean value, 2.1 ng/mL in the pre-PMI IVC group vs. 1.3 ng/mL in the post-PMI VC group, p=0.067) in the post-PMI VC group. It is well-known that SCC-Ag levels are related to tumor size and pathologic PMI [32]. Thus, the higher levels of SCC-Ag in early-stage cervical cancer may reflect the extents of pathologic PMI and lymphovascular space invasion. In addition, the intact cervical stromal ring on MRI might correlate with favorable pathologic features including smaller tumor size, less lymphovascular space invasion, superficial stromal invasion, and less extensive PMI. Therefore, the intact cervical stromal ring on MRI might identify the low-risk group of patients in terms of PMI, lymphovascular space invasion, and stromal invasion in early-stage cervical cancer.
Surgical proficiency is another consideration for MIS RH. Most learning curve analyses of MIS RH have focused on operating times, pathologic outcomes, and complications. However, speed is not a fair reflection of the entire learning process and surgical proficiency. In addition, the median follow-up period in the late phase of LRH was relatively too short to draw any conclusions about survival outcomes [3334]. Several authors have also suggested that over 40 cases were required to achieve adequate oncologic outcomes, and that the recurrence rates in the early and late phases of LRH were comparable for tumor sizes less than 2 cm [333435]. Likewise, improved survival outcomes in the post-PMI VC group may result from the gain of surgical proficiency. But more importantly, postgraduate gynecologic oncologists should start MIS RH in highly selected patients, considering the status of cervical stromal ring and tumor size on MRI, during their training period because the patient should not experience disease recurrence in the early phase of learning a MIS RH.
There are some limitations displayed by RCTs relating to surgical interventions. In surgical trials, no matter how reproducible the procedure is, the results are not similar for all surgeons [36]. Unlike pharmacological trials, thus, surgical trials may not be objective and reproducible because anatomical differences in patients exist, and surgeons do the same surgical procedure differently. For example, some surgeons do medial to lateral dissection while others lateral to medial mobilization of the colon in laparoscopic colectomy [37]. Similarly, each surgeon might have a different approach in colpotomy and uterine manipulation in the LACC trial [5]. In the pre-PMI IVC group, the rate of DFS (84.5%) were consistent with the 4.5-year rate of DFS (86.0%) reported in the LACC trail. The rate of DFS (98.0%) in the post-PMI VC group were similar to that of the open surgery group in the LACC trial (96.0%). These survival outcomes in our study may result from the gain of surgical proficiency in the post-PMI VC group. However, tumor size tended to decrease from the pre-PMI IVC group to post-PMI VC group, which may reflect inappropriate patient selection in the pre-PMI IVC group and the effects of applying the PMI criterion in the post-PMI VC group. Thus, the application of PMI criterion on MRI and VC may contribute the improved oncologic outcomes. In addition, the sample size calculation was performed using Power and Sample Size Software version 15 [38]. In multivariate analysis, the status of cervical stromal ring on MRI (HR=20.321; p<0.001) was the most significantly associated risk factor with DFS in early-stage cervical cancer patients treated with MIS RH. Under the assumption that MIS RH will be performed using VC, the 3 key components including HR of 20.0, type 1 error (α) of 0.05, and power (1-β) of 0.8 were considered. Finally, a total sample size of 349 patients was calculated. Thus, 349 patients are needed to confirm our findings in future RCTs.
Our study has several limitations. First, the study population number was relatively small. Second, PMI prediction criterion is not 100% accurate. Thirty-two (15.5%) of 206 patients with an intact cervical stromal ring on MRI had a pathologic PMI. However, the status of the cervical stromal ring on MRI can provide valuable guidance for physician regarding the primary management of early-stage cervical cancer patients. Third, the median duration of follow-up in the post-PMI VC group was relatively short (25.0 months), and long-term follow-up is necessary to draw conclusions about survival outcomes. In our study population, however, most of the disease recurrence (81.0%, 17/21) occurred within 2 years after surgery, and the median follow-up period was over 2 years in the post-PMI VC group. Also, the number of patients who were lost to follow-up in the post-PMI VC group was very small (1.0%, 1/99). In the pre-PMI IVC group, 4 patients (21.0%) experienced relapse ≥2 years after surgery (2 patients, vaginal stump; 1 patient, ovary; 1 patient, liver), and most of the disease recurrence (79.0%, 15/19) occurred within 2 years after surgery (Supplementary Table 1). Previous studies have reported that the median recurrence-free interval in cervical cancer patients with a pelvic recurrence who received RH was 14 months, 77% of recurrence were detected within 3 years after RH, and 35% of recurrent cervical cancer patients were asymptomatic [3940]. In the LACC trial, however, disease recurrence from cervical cancer occurred at a constant rate throughout the follow-up period. Therefore, the pattern, timing, and predictors of disease recurrence in the MIS group of LACC trial should be further investigated. In addition, the methods of post-treatment surveillance will affect the detection timing of disease recurrence. With the aim of early detection of recurrence where there is the possibility for curative resection, all patients who received MIS RH in our institution were observed every 3 months, using history, physical examination, cytology, and tumor biomarkers, and every 6 months, using computed tomography, during the first 2 years. Thus, asymptomatic recurrence in our study might be detected earlier.
The real culprit in poorer prognosis of early-stage cervical cancer should not be the surgeon. Therefore, strategies to avoid tumor exposure during parametrectomy and colpotomy should be implemented in MIS RH. Two factors mentioned so far such as anatomical location of the uterine cervix and CO2 pneumoperitoneum are uncontrollable factors in MIS RH. However, both selection of optimal surgical candidates and colpotomic approach are correctable factors in MIS RH. In conclusion, MIS RH should be performed in optimal surgical candidates with an intact cervical stromal ring on MRI to obtain en bloc resection without positive margin and tumor exposure to the CO2 pneumoperitoneum, using VC. Our efforts to avoid tumor exposure during parametrectomy and colpotomy have enabled us to perform a safe MIS RH.
 XML Download
XML Download