

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epithelial ovarian carcinoma is often presented in an advanced stage at diagnosis. Maximal debulking surgery followed by platinum- and taxane-based chemotherapy is the current standard treatment for advanced ovarian cancers, which achieves a clinical complete response (CR) rate of 40%–50% [1]. Unfortunately, half of the complete responders will subsequently experience recurrent diseases. Hence, around 75% of patients with advanced diseases require management for persistent or recurrent diseases and further salvage chemotherapy.
Although second-line chemotherapy can provide substantial response rate and control of symptoms after relapse if initial sensitivity of the tumor has been experienced, they are not curative. An effective maintenance therapy that could prevent/delay recurrences after a clinical CR might have potentially greater clinical benefits [2]. Extended cycles of the same platinum-based chemotherapy failed to improve survival [3,4].
A Gynecologic Oncology Group (GOG) study showed a significantly longer median progression-free survival (PFS) of 7 months in International Federation of Gynecology and Obstetrics (FIGO) stages III–IV ovarian cancer patients randomized to maintenance therapy with 12 cycles of paclitaxel after achieving clinical complete remission than that of patients accepting 3 cycles of paclitaxel [5]. However, the overall survivals (OSs) were not different [6]. An Italian multicenter trial compared 4 courses of topotecan with no therapy after response to first-line chemotherapy in patients with FIGO stage I–IV ovarian cancer, which showed no benefit for the treatment group [7]. No benefit was observed using interferon-α 2a as maintenance therapy following surgery and chemotherapy in patients with IC–IV ovarian cancer in a randomized phase III study [8].
Pegylated liposomal doxorubicin (PLD) showed activity in recurrent ovarian cancer [9,10]. In a phase II trial of the Taiwanese Gynecologic Oncology Group which investigated heavily pre-treated recurrent and refractory ovarian cancer patients with distearoylphosphatidylcholine PLD (Lipo-Dox®; TTY Biopharm Co. Ltd., Taipei, Taiwan) alone achieved 23.1% overall response [11]. The GINECO phase II trial used PLD (Caelyx®; TTY Biopharm Co. Ltd.) (30 mg/m2) and carboplatin (area under the curve [AUC] 5) in recurrent ovarian cancer with grade 3–4 neutropenia (23%), anemia (4%) and thrombocytopenia (8%) [12]. This combination was used in recurrent/metastatic cervical and uterine malignancies as carboplatin AUC5 and PLD (Doxil®; TTY Biopharm Co. Ltd.) 35 mg/m2 every 4 weeks with overall response rate of 33% and acceptable toxicity [13].
In the current study, we used PLD in combination with carboplatin 4-weekly as maintenance chemotherapy in advanced epithelial ovarian patients who had achieved clinical complete remission after 5–6 courses of taxane/platinum-based first-line chemotherapy. Carboplatin was chosen because these patients had responded to the platinum-based chemotherapy. It seemed reasonable to continue using them yet at reduced dose intensity. A post hoc translational study was conducted to deep sequence BRCA/homologous recombination deficiency (HRD) genes, because BRCA/HRD mutations (BRCA/HRDm) are known to be associated with better prognosis [14-16].
PATIENTS AND METHODS
1. Eligibility
Patients were eligible if they met the following inclusion criteria: 1) histologically proven epithelial ovarian cancer of FIGO stage III/IV; 2) treatment with 5 to 6 cycles of platinum/paclitaxel regimen and attainment of a clinical defined CR (i.e., no cancer-related symptoms; normal physical examination, computed tomography (CT) scan of the abdominal/pelvis and chest X-ray; cancer antigen (CA)-125 level ≤35 U/mL); 3) performance status of Eastern Cooperative Oncology Group (ECOG) 0–2; 4) adequate organ functions; 5) age 20–75 years old; 6) life expectancy equal or longer than 3 months; and 7) ability to understand and willingness to sign a written informed consent document.
Exclusion Criteria included: 1) presence of CNS metastases (including clinical suspicion); 2) other malignancies with exception of curative treated non-melanoma skin cancer or cervical carcinoma in situ within 5 years prior to entering the study; 3) presence of other serious concomitant illness which can affect or elevate the value of CA-125, e.g. autoimmune disease, sarcoidosis, chronic active hepatitis; 4) presence of other serious concomitant illness which might be aggravated by study medication: uncontrolled infection (active serious infections that are not controlled by antibiotics) such as active cardiac disease (e.g. decompensate myocardial infarction within 6-month period preceding entry into the study, or history of ventricular arrhythmia or congestive heart failure; 5) surgery within 2 weeks prior to entering the study; 6) radiotherapy within 4 weeks prior to entering the study; 7) concurrent chemotherapy, radiotherapy, or other investigational drug except non-disease related conditions (e.g. insulin for diabetes) during study period; 8) mental status is not fit for clinical trial; 9) pregnant or breast feeding women; and 10) potential child-bearing women unless using a reliable and appropriate contraceptive method.
2. Study design
The study was an Asian Gynecologic Oncology Group (AGOG) phase III randomized, controlled, multi-center trial (AGOG06-001). Registration and random assignment was in a 1:1 ratio. Stratification factors were residual tumor size after primary debulking surgery (residual tumor ≤1 cm, or >1 cm), and serum CA-125 level at the time of registration (<10, 10–35 U/mL). The primary end-point was PFS. Secondary end points included OS, safety, and quality of life (QoL). At initial design, a sample size of 131 patients per treatment arm (a total of 262 patients) was required to provide α error and power were 0.05 and 75%, 1-sided to detect an improvement of 6 months in median progression-free interval (PFI) (arm B vs. arm A: hazard ratio [HR]=1.33; PLD/carboplatin: median PFI=24 months; observation: PFI=18 months).
However, referring to the recent maintenance trials such as GOG218 [17], we recalculated sample size based on the median PFS=10 months of the chemotherapy alone group, assuming arm A of HR=0.63 as compared to arm B, by one-sided test under resetting accrual time 60 months and additional 36-month follow-up period to achieve 80% power at 5% significance level. The amendment with sample size of 122 evaluable patients was approved on March 31, 2014.
3. Pretreatment and follow-up evaluations
Pre-random assignment assessment included clinical history, physical examination, blood tests, CT of pelvic and abdomen, chest X-ray, and QoL using EORTC-QLQ-C30 & EORTC-QLQ-OV28 questionnaires. During treatment, toxicity was evaluated on each visit according to the Common Terminology Criteria for Adverse Events (CTCAE version 3.0), and blood tests were performed at baseline and each visit. The patient was followed until the adverse event resolved up to 30 days after lase dose of study medication. Follow-up assessments were performed monthly for 6 months and then 6-monthly after the completion of treatment. QoL was assessed at baseline and repeated before each cycle of treatment until end of treatment, monthly for another 6 months, then 6-monthly for 3 years. Upon suspicion of recurrence, patients underwent histologic confirmation (where feasible), and/or restaging CT/magnetic resonance imaging or positron emission tomography imaging.
4. Treatment
All eligible subjects in arm A received PLD 30 mg/m2 intravenously (IV) over 1 hour on day 1 followed by carboplatin AUC4 IV for 30 minutes in a 28-day cycle. Dose modifications were based on the worst toxicity degree graded by CTCAE version 3.0. Prophylactic hematologic support was permitted (e.g., blood transfusions, granulocyte-colony stimulating factor, etc.) according to the institute site standard.
5. Statistical analysis
Cancer progression was defined as appearance of new lesion(s), malignant ascites or pleural effusion, or by serologic progression as defined by a CA-125 level at least twice the baseline value and the absolute value >35 U/mL, confirmed at least one week later [18]. PFS and OS was calculated from the date of randomization to the date of events or censored at the date of last contact. All eligible patients were analyzed based on intension-to-treat. Survival curves were estimated using Kaplan-Meier method, and log-rank test was used for the comparison of survival between groups. HRs were estimated using Cox regression model. The comparison of clinical characteristics between the 2 groups was based on the Wilcoxon rank sum test for continuous variables, and Fisher exact test for categorical data. A p-value of <0.05 was considered significant. Global health/QoL scores were transformed to a 100-point scale [19] for comparison. Significance of QoL analyses of individual symptoms were evaluated with false discovery rate correction method and repeated measures mixed-model analysis of covariate [20,21].
6. Detection of BRCA1 and BRCA2 variants and HRD-related genes
A post hoc translational study was conducted to deep sequence BRCA/HRD gene panel in the Taiwanese sites after Institutional Review Board approval. For knowing the BRCA/HRDm status, next-generation sequencing (NGS) was used for genotyping of formalin-fixed paraffin-embedded (FFPE) tumor samples. FFPE samples of adequate DNA quality were analyzed by ACTRepair™ Gene Panel Sequencing. Sixty nanograms of genomic DNA were amplified to target all coding exons of 35 HRD-related genes (including BRCA1/2; gene list in Supplementary Data 1). The sequencing and analysis procedures are detailed in the Supplementary Data 1. NGS-identified variants with an allele frequency >10% were confirmed by Sanger sequencing. To distinguish between germline and somatic mutations, Sanger sequencing was also performed for normal tissues (for all BRCA/HRD variants) [22]. Pathogenicity of BRCA/HRD variants were categorized as pathogenic, likely pathogenic, variants of uncertain significance, likely benign, and benign, according to guidelines and terminology published by the American College of Medical Genetics and Genomics and the Association for Molecular Pathology in 2015 [23]. Only BRCA/HRD variants of pathogenic or likely pathogenic were designated mutations.
RESULTS
Between June 2007 and September 2014, 45 patients were enrolled and randomized (1:1) with stratification factor of residual tumor at primary surgery and CA-125 serum level at enrollment. Enrollment was slow, therefore a decision of closing accrual was made by the AGOG board meeting when 7+ years had lapsed. We ended the study after the last enrolled patient had completed 3-year follow-up. The final analysis was performed despite the fact that the number of patients needed had not yet been reached. Data collection was completed on December 31, 2017, and the database was locked on June 1, 2018. The CONSORT flow diagram is shown in Fig. 1. One arm A patient was found ineligible shortly after randomization and was excluded without treatment. The safety and efficacy populations exclude this ineligible patient. The remaining 44 patients started the allocated treatment (arm A, n=23, received a median of 6 courses, range 2–6) or observation (arm B, n=21). Characteristics of the patients are summarized in Table 1. The clinical characteristics were well balanced. In arm A, 2 patients withdrew consent after the 3rd and 4th cycle, respectively. Two patients both stopped treatment because of intolerability after the 5th cycle, while one patient progressed after 2nd cycle and was off study. In arm B, 1 patient progressed at the 5th monthly visit, the remaining 20 patients completed 6 visits during treatment period.

Table 1
Patient demographics and clinical characteristics

Data are presented as number (%) unless otherwise indicated. Age (years) is presented as median (range), which tested by Wilcoxon rank sum test. Categorical variables tested by Fisher's exact test.
CA, cancer antigen; ECOG PS, Eastern Cooperative Oncology Group performance status; FIGO, International Federation of Gynecology and Obstetrics.
1. Survival outcomes
With a median follow-up of 88.9 months, 28 patients experienced cancer progression (12 [52.1%] for arm A and 16 [76.2%] for arm B), and 21 died of disease (9 [39.1%] for arm A and 12 [57.1%] for arm B). The median PFS was significantly better in arm A (55.5 months) than arm B (9.2 months) (p=0.017 by log-rank; HR=0.40; 95% confidence interval [CI]=0.19–0.87; p=0.020) (Fig. 2A), yet the median OS was not significantly different in arm A (not reached) than arm B (95.1 months) (p=0.148 by log-rank; HR=0.53; 95% CI=0.22–1.27; p=0.154) (Fig. 2B).

2. Safety
Toxicities are summarized in Table 2. Overall rates of grade 3/4 adverse events on a patient basis were 60.9% for arm A and 0.0% for arm B (p<0.001). Grade 3/4 neutropenia were significantly more frequent in arm A than arm B with 43.5% (10/23, all were in treatment period) and 0% (0/21), respectively (p=0.001).
Table 2
Adverse events

3. QoL
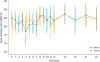
QoL compliance was similar between patients on the two arms. QoL results were available for 95.5%, 93.2%, 84.1%, 59.1%, 50% at baseline and 12 weeks and 6, 12, 24 months, and 3 years after completion of treatment, respectively. Those met the primary end-point (cancer progression) tends to stop QoL recording. Therefore, longitudinal modeling was analyzed for the first 6 months (during protocol treatment), and the remaining 2.5 years. Global health/QoL scores showed a non-significant overall difference between the 2 treatment arms based on mixed-model analysis (Fig. 3), and specifically no difference between arms at baseline, 6th month, 12th month (Supplementary Table 1). In the QLQ-C30 symptom scores for the arm A during the first 6 months were worse than baseline; however, the scales reported differences of ≤10 points, except dyspnea and appetite loss (Supplementary Table 1). QLQ-OV28 symptom scores changes are summarized in Supplementary Fig. 1 and Supplementary Table 2, which showed comparable recovery of peripheral neuropathy from randomization in spite of carboplatin use in arm A.
4. BRCA mutation (BRCAm) status and HRD-related genes
Thirty-one patients had FFPE specimens available for BRCA/HRDm status analysis. Thirteen BRCA1/2 variants of 10 (32.3%) patients were identified. Of these 13 variants, 5 variants were pathogenic (Table 3, Supplementary Table 3, and Supplementary Fig. 2). Among the 26 patients with wild-type BRCA (BRCAw), 19.2% (5/26) had pathogenic/likely pathogenic mutations in HRD-related genes (ATM, PTEN) other than BRCA1/2 (Table 3). Overall, 16.1% (5/31) and 32.3% (10/31) of the tumors were BRCAm and BRCA/HRDm, respectively. Clinicopathological features and variant descriptions of the cases with BRCA/HRDm are summarized in Table 3. Distribution of BRCA1/2m on both arms (arm A: 1/15 [6.7%] versus arm B: 4/16 [25%], p = 0.333) or BRCA/HRDm on both arms was not significantly different (arm A: 2/15 [13.3%] versus arm B: 8/16 [50%], p = 0.054), but marginally favored arm B. The PFS or OS was not different according to BRCA/HRDm status in arm B or arm A or both arms combined (Supplementary Figs. 3, 4, 5, 6, 7, 8).
Table 3
Clinicopathological features and variant descriptions of the cases with BRCA1/2 or HRD mutations

5. Exploratory subgroup analyses
Forest plots of the treatment effect on subgroups are shown in Supplementary Figs. 9 and 10, a trend of PFS benefit with maintenance therapy was seen across performance status, residual tumor, and baseline CA-125, but age >50 years (p=0.003), BRCAw/non-HRD (HR=0.35; 95% CI=0.11–1.18; p=0.091) subgroups seemed to fare better with maintenance therapy. However, patients with BRCAw/non-HRD tumors were significantly older than those with BRCA/HRDm (p=0.027; Supplementary Tables 4 and 5).
DISCUSSION
In this randomized trial, maintenance chemotherapy using 4-weekly carboplatin AUC4 and PLD 30 mg/m2 for six cycles after achieving clinical complete remission significantly improved PFS (arm A: median 55.5 months) than observation (arm B: 9.2 months) (HR=0.40; 95% CI=0.19–0.87; p=0.020) in patients with advanced ovarian cancer, yet the median OS was not significantly different. Although we deliberately chose a lower dose level with a 4-weekly interval, 60.9% (14/23) experienced grade 3/4 toxicities, but 78.3% (18/23) completed 6 cycles without significantly increasing peripheral neuropathy (Supplementary Fig. 1 and Supplementary Table 2). Besides, BRCAw/non-HRD (p=0.091) subgroup seemed to fare better with maintenance therapy (Supplementary Fig. 9).
The AGOG06-001 trial lasted 11 years. Between the commencement and conclusion of our trial, several maintenance trials after chemotherapy have been published [17,24-29]. Adding bevacizumab to standard paclitaxel-carboplatin followed by maintenance bevacizumab, two trials (GOG218 and ICON7) using different doses (15 and 7.5 mg/kg) and duration of maintenance (17 and 12 cycles) both achieved significantly prolonged PFS (3.8 months, p<0.001 and 1.7 months, p=0.04 by log-rank test, respectively) compared with no bevacizumab [17,24]. Using CA-125-specific murine monoclonal antibody, oregonomab [25] or an anti-idiotypic antibody against OC125, abagovomab [26], failed to prolong PFS or OS. A serine/threonine kinase inhibitor, enzastaurin, was added on to standard paclitaxel and carboplatin followed by maintenance enzastaurin (PCE) compared to chemotherapy alone without maintenance (PC) in stage IIB–IV ovarian, fallopian tube or peritoneal cancer in a phase II trial. A 3.7-month longer but not significant PFS was seen in the PCE arm (HR=0.8; 95% CI=0.5–1.29; p=0.37) [27]. A randomized phase III study of erlotinib versus observation in high-risk stage I, stages II–IV ovarian cancer patients who were non-progressive after first-line chemotherapy did not improve PFS or OS [28].
In the AGO-OVAR16 trial, maintenance pazopanib significantly prolonged PFS (HR=0.77; 95% CI=0.64–0.91, p=0.002) compared with placebo for those with FIGO stage II–IV ovarian cancer patients non-progressive after first-line platinum-taxane chemotherapy. However, OS was not significantly different in the whole study cohort, while a detrimental effect was seen in the East-Asian population (HR=1.71; 95% CI=1.01–2.89, p=0.047) [29]. To further interrogate efficacy and safety of pazopanib maintenance therapy in the East-Asian population, a study enrolled 145 patients and combined the East-Asian subgroup of AGO-OVAR 16 (n=209), in which a significant imbalance was seen in distribution of BRCA1/2 mutation carriers (pazopanib 10%, placebo 22%, p=0.010) [30]. BRCA1/2 mutation carriers are known to have better prognosis in ovarian cancer patients treated with chemotherapy [14,15]. BRCA/HRDm is associated with significantly better outcome in platinum-treated serous ovarian cancer [16]. Our post hoc BRCA/HRD analysis of genomic profiling of the AGOG06-001 trial tumor samples showed no bias in the distribution of BRCAm or BRCA/HRDm between the 2 arms.
The GOG 212 study was presented in 2017 Society of Gynecologic Oncology Annual Meeting as a late breaking abstract [31]. Patients with stage III–IV ovarian, tubal, or peritoneal cancer with clinical CR (n=1,157) were randomized to surveillance (S), paclitaxel (P) 4-weekly for 12 cycles, or paclitaxel poliglumex (PP) on the same schedule. Patients were followed for a median of 71 months; small but significant benefits were seen in P-arm (HR=0.783; 95% CI=0.666–0.921) or PP-arm (HR=0.847; 95% CI=0.721–0.995) than S-arm for PFS (median PFS: S, 13.4; P, 18.9; and PP, 16.3 months), but not OS. The difference between their results and ours may be due to our using carboplatin (which was proven more important than paclitaxel in treating advanced ovarian cancer [32], and adding another new active agent PLD. A recently published phase III randomized, double-blind placebo-controlled trial (SOLO1) showed that maintenance olaparib significantly improved PFS or death compared with placebo (HR=0.30; 95% CI=0.23–0.41; p<0.001) in women with deleterious BRCA1/2 mutations with advanced ovarian cancer responding to first-line chemotherapy. After a median follow-up of 41 months, the rates of freedom from death or progression at 3 years were 60% versus 27%, and the median time to subsequent therapy or death of olaparib group was 51.8 months as compared with the placebo group (15.1 months) [33]. Several trials for patients with BRCAw tumors incorporating poly (ADP-ribose) polymerase inhibitors and/or immune checkpoint inhibitors have been launched, yet the results need years to know.
We acknowledge the limitations of our study due to the small sample size, which makes the results unstable. However, this study did show that maintenance chemotherapy (4-weekly carboplatin AUC4 and PLD 30 mg/m2 for 6 cycles) after complete remission to first-line chemotherapy could be beneficial improving PFS in stages III/IV ovarian cancer with CR to front-line chemotherapy. It might be a pharmacoeconomic option especially for BRCAw/non-HRD subgroup.
 XML Download
XML Download