

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Human papillomavirus (HPV) infection is the main cause of cervical cancer, with an estimated 530,000 cases worldwide in 2012. There were 266,000 deaths due to cervical cancer, accounting for 8% of all cancer-attributed deaths in women that year [1]. In Korea in 2015, 3,582 new cervical cancer cases were reported with 967 cervical cancer deaths. Cervical cancer is a disease associated with significant patient burden, and in 2015, it was the third most common cancer in Korean women aged 15–34 years [23]. Between 2004 and 2015, the prevalence of cervical cancer in Korean women declined; however, the number of patients diagnosed with carcinoma in situ, cervical intraepithelial neoplasia 1, 2, not designated as cervical cancer, increased 2-fold during the same period [4]. Additionally, the overall prevalence of HPV infection in Korean women was 34.2%, with 49.9% of women aged 18–29 years infected [5]. By March 2017, 2 vaccines, Gardasil and Cervarix, had been introduced to prevent cervical cancer as part of a National Immunization Program (NIP) in 71 countries worldwide [6]. In Korea, these vaccines have been available since 2007 after obtaining approval from the Ministry of Food and Drug Safety, and have been included as part of a NIP to vaccinate girls aged 12 years in 2016 [7]. Both vaccines were known to have a preventive effect on the HPV-16/18 genotypes that cause 70% of the cervical cancers [8]. Because insurance providers do not cover the cost of HPV vaccinations and some women prefer to be vaccinated privately (i.e., outside of the NIP) according to the recommendations of their gynecologist, there is a paucity of information regarding HPV vaccination status in Korea.
Because HPV genotype distribution varies according to geographic region and race [9], it is necessary to determine the impact of vaccination. There is limited research on the extent and the status of HPV vaccination in Korea. In light of this, it is necessary to investigate the status of HPV vaccinations among Korean women. Therefore, we analyzed HPV vaccination status among HPV-infected Korean women aged ≥20 years, and the prevalence of vaccine-targeted HPV genotypes according to HPV vaccination before the introduction of NIP.
MATERIALS AND METHODS
1. Materials
We used data collected from the Korea HPV cohort study, which is a multicenter study, undertaken within the obstetrics department at five general hospitals across Korea in 2009 to identify high risk factors of cervical disease progression (until the stage of high-grade squamous intraepithelial lesions [HSILs]) among HPV-infected adult Korean women. The HPV cohort study registered subjects who satisfied the following inclusion criteria. First, the participants were Korean women aged 20–60 years with a DNA test positive for HPV regardless of HPV genotype, and second, HPV-infected women were diagnosed with atypical squamous cells of undetermined significance (ASCUS) or low-grade squamous intraepithelial lesion (LSIL) via a Papanicolaou (Pap) test [10]. From 2010 to 2016, out of 1,325 registered adult women in the cohort study, 1,300 women who responded to questions about their HPV vaccination history were selected as individuals for this study. To compare the prevalence of HPV genotypes by HPV vaccination, we collected data from 1,181 women by carrying out HPV genotyping after HPV vaccination (Fig. 1). Each of the 5 hospitals obtained approval from their Institutional Review Board (IRB) to participate in the HPV cohort study. In addition, we obtained approval from the IRB of the Korea Centers for Disease Control and Prevention for this study (No. 2015-05-EXP-05-P-A).

2. Laboratory methods
For cervical cytology, laboratories at each of the five participating hospitals screened liquid-based Pap smears using Cervex-Brush (Rovers Medical Devices, Oss, The Netherlands) of all subjects enrolled in this cohort study. HPV genotyping was conducted using the DNA microarray technique (DNA chip), which is based on the polymerase chain reaction (PCR) method. Briefly, after amplification, PCR products were analyzed by electrophoresis and hybridized with radiolabeled generic probes specific to HPV [10].
3. Analysis
The study individuals were divided into vaccination and non-vaccination groups. This was based on baseline data from standardized case report forms at the time of cohort registration in each of the 5 hospitals. The cohort study staff interviewed subjects or reviewed their medical chart for vaccination history (vaccine type, vaccine doses, and vaccine date). Women who received at least one dose of HPV vaccine (Gardasil or Cervarix) were classified as being in the vaccination group. Subject characteristics were analyzed by age (20–29, 30–39, 40–49, 50–60 years) at ASCUS or LSIL diagnosis by Pap test, marriage status (married or unmarried), education level (middle school or lower, high school, university, graduate school or higher), monthly income level (<$3,000, $3,000–4,999, $5,000–6,999, ≥$7,000), occupation (housewives, administrator or expert, service or salesman, others), smoking status (non-smoker, ex-smoker, current smoker), alcohol drinking status (non-drinker, ex-drinker, current drinker), the number of sexual partners in the last year (none, 1 person, 2–3 persons, ≥4 persons), family history of cervical cancer (no, yes), and Pap test results (ASCUS, LSIL). HPV genotype at baseline was classified as HPV-16/18 (vaccine-targeted HPV genotypes). Logistic regression analysis was used to analyze the association between the status of vaccination by epidemiological variables with the odds ratio (OR) and 95% confidence interval (CI). For vaccination groups, we analyzed vaccine type, age at vaccine initiation (recommended age; ≤25 years old for Cervarix, ≤26 years old for Gardasil), the period from vaccination to ASCUS or LSIL diagnosis by Pap test (1–12 months, >12 months), Pap result (ASCUS, LSIL), and HPV genotype (HPV-16/18, other genotypes) by HPV vaccine doses (1–3) using the Cochran-Armitage test for trends.
We analyzed the prevalence of the HPV-16/18 genotype, which was the common HPV genotype targeted by both vaccines: Gardasil, a quadrivalent vaccine, and Cervarix, a bivalent vaccine. HPV-16/18 genotype prevalence was defined as the proportion of cases with at least one genotype (HPV 16 or HPV 18) among individuals. To estimate the prevalence of HPV-16/18 according to the period post HPV vaccination prior to ASCUS or LSIL diagnosis, we performed multiple logistic regression analysis by employing a model adjusted for demographic variables. The p-values of <0.05 were regarded as statistically significant. All statistical analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
1. Characteristics of HPV vaccination in Korean adult women with HPV
Among 1,300 Korean adult women with HPV diagnosed ASCUS or LSIL, 25.8% were vaccinated against HPV. The proportion of subjects with HPV vaccination according to demographic variables was significantly different depending on age at ASCUS or LSIL diagnosis, marital status, and education level. The proportion of women who were vaccinated against HPV was higher among younger participants; 53.8%, 36.0%, 14.1%, and 3.6% were vaccinated among women in their 20's, 30's, 40's, and 50's, respectively. Compared to the proportion of HPV vaccinated individuals among women aged 50–60 years, women in their 20's were 11.01 times more likely to be vaccinated (95% CI=5.05–23.98), 7.69 times more likely in their 30's (95% CI=3.70–15.97), and 3.14 times more likely in their 40's (95% CI=1.50–6.57). For marital status, 45% of the unmarried women were more likely to be vaccinated than the vaccinated proportion of the married women (adjusted odds ratio [aOR]=2.08; 95% CI=1.51–2.88). There was a higher likelihood of vaccination among those who had a higher education level; compared with those with a middle school education (2.3%; Table 1), individuals with a high school education (vaccinated proportion 15.0%, aOR=3.50; 95% CI=1.04–11.79), university (35.2%, aOR=5.65; 95% CI=1.69–18.86), and graduated school or higher (34.3%, aOR=7.14; 95% CI=2.01–25.42) were more likely to be vaccinated.
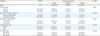
Table 1
Epidemiological characteristics of HPV-infected adult women according to HPV vaccination in Korea

Data shown are number (%) not otherwise specified. Age (Pap): age at ASCUS or LSIL diagnosis by a Papanicolaou test.
aOR, adjusted odds ratio; ASCUS, atypical squamous cells of undetermined significance; CI, confidence interval; HPV, human papillomavirus; KRW, Korean Won; LSIL, low-grade squamous intraepithelial lesion; OR, odds ratio.
*Missing value were excluded in the analysis; †The currency exchange rate of 1 KRW to U.S. Dollar (USD) was approximately 0.0008 (1,000,000 KRW=845.3 USD).
![]()
Among the 335 vaccinated women, 68% and 32% were vaccinated using Gardasil and Cervarix, respectively. Of these, 20.3% were vaccinated with one dose, 16.4% with 2 doses, and 63.3% with three doses.
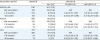
There were no significant differences according to vaccine dose in the vaccination group when comparing vaccine types and clinical diagnosis results (PAP result; ASCUS, LSIL). For HPV-vaccinated individuals by vaccine dose, there was a significant younger age at vaccination initiation (p=0.025). For the duration of vaccination, 72% of 156 individuals with more than 12 months from vaccine initiation were vaccinated with three doses; they were more likely to be vaccinated within 12 months less or equal duration from vaccination (p=0.001). The proportion of HPV-16/18 among individuals with three doses was lower than that of other HPV genotypes (p=0.028; Table 2).
Table 2
Status of HPV vaccination among HPV-infected adult women by vaccine dose in Korea
ASCUS, atypical squamous cells of undetermined significance; HPV, human papillomavirus; LSIL, low-grade squamous intraepithelial lesion.
*Missing value were excluded in the analysis; †Recommended age: ≤25 years old for Cervarix, ≤26 years old for Gardasil; ‡The length of the period from date of HPV vaccination to date of PAP test.
![]()
2. The prevalence of HPV-16/18 genotypes by HPV vaccination
Of the 1,300 study subjects, both the results and date of HPV genotyping were acquired for 263 vaccinated and 918 unvaccinated women. For vaccinated women, the median time from HPV vaccination to ASCUS or LSIL diagnosis was 11.45 months (1.30–26.55; interquartile Q1–Q3 range). The overall prevalence of HPV-16/18 among 1,181 individuals was 17.0% (19.2% with ASCUS; 13.9% with LSIL). Using unvaccinated women as the control group, after adjusting for age at the time Pap test and HPV vaccine doses, we performed a comparison to analyze the prevalence of HPV-16/18 by post vaccination period. For at least 12 months after HPV vaccination, the prevalence of the HPV-16/18 genotypes in the vaccinated group was 11.0%, which was significantly lower than the prevalence for the unvaccinated group (adjusted prevalence ratio [aPR]=0.51; 95% CI=0.29–0.88). Particularly, for LSIL patients, the prevalence of HPV-16/18 genotypes at least 12 months post vaccination was 7.3%, which was significantly lower than the prevalence for unvaccinated patients (aPR=0.35; 95% CI=0.13–0.96). Vaccinated women with ASCUS did not show a significantly lower prevalence for HPV-16/18 genotypes than unvaccinated women (Table 3).
Table 3
The prevalence of HPV-16/18 among HPV-infected adult women with abnormal cervical cytology by the vaccination period
aPR, adjusted prevalence ratio ASCUS, atypical squamous cells of undetermined significance; CI, confidence interval; HPV, human papillomavirus; LSIL, low-grade squamous intraepithelial lesion; PR, prevalence ratio.
*Prevalence of HPV-16/18 genotypes.
![]()
DISCUSSION
Our findings revealed the status of HPV vaccination among Korean adult women with HPV (aged 20–60 years) before the introduction of NIP in 2016. This is the first study to analyze the overall vaccination status among HPV-infected Korean adult women with ASCUS or LSIL.
In this study, the proportion of HPV-infected adult women who received a HPV vaccination was approximately 26%. In a previous study on Korea's National Immunization Survey in 2013, it was revealed that overall, 12.6% of individuals aged 19–59 years were vaccinated. The HPV vaccination status varied with age; 28.7%, 15.9%, and 4.6% individuals were found to be vaccinated in the age groups of 19–26 years, 27–39 years, and 40–59 years, respectively [11]. Compared with the results of this study, we noted that HPV-infected women were more likely to be vaccinated compared to the general population. In this study, the proportion of women aged 20–29 years who received HPV vaccination was 55%. Younger women with higher education levels were more likely to be vaccinated. HPV vaccination was related to higher education in adult Korean women. This could explain by the fact that higher educated women could be better informed regarding HPV vaccination [12]. The HPV vaccination proportion did not differ according to other epidemiological factors, except for age, marital status, and education level. In addition, we found that less than 30% of women who had none to one sexual partner in the last year were vaccinated, whereas 37.5% of women who had 2–3 sexual partners and 75% of the women with ≥4 sexual partners in the last year were vaccinated. This could predict its use as a preventive measure against exposure to HPV infection. However, there was no statistically significant difference in the proportion of vaccinations as few subjects had >1 sexual partners in the last year. The price of 3 vaccine doses for Cervarix or Gardasil was about 500 dollars in Korea. Although both vaccines investigated in this study are expensive and their costs were not covered by Korean health insurance, we did not find any significant difference between the monthly income of vaccinated and non-vaccinated participants.
In Korea, although Gardasil and Cervarix have been in circulation in the market since 2007 and 2008, respectively, NIP has been conducted since mid-2016. In some countries that had initiated NIP earlier than Korea, including Australia, the UK, and the USA, the beneficial effects of these vaccines, such as reduction in HPV infections, genital warts, and cervical cancer lesions, have already been reported. Over 70% of the targeted individuals have been vaccinated, and consequently, the prevalence of vaccine-type HPV and genital warts (HPV-6 and -11) has been reduced by 86% and 93%, respectively [13]. Hence, HPV vaccine is generally administered before the age of sexual initiation, but HPV vaccination has also been recommended for adult women [1415]. HPV vaccine is also known to be effective in preventing HPV persistence and cervical intraepithelial neoplasia (CIN) progression among adult women who were exposed to sexual activities [1617]. In this study, the proportion of women vaccinated according to age recommendations (Cervarix: aged 9–25; Gardasil: aged 9–26) was 25.2%, and their prevalence of HPV-16/18 was 18.5%, which was not significantly different in the prevalence of HPV-16/18 both among vaccinated women over age 26 (16.1%) and non-vaccinated women (17.8%).
The duration of HPV antibody response is critical for prevention of HPV infection. Immunogenicity is highly dependent on the number and timing of vaccine doses. According to several reports, antibody responses to each type were heterogeneous: seroconversion for HPV-16 occurred most frequently between 6 and 12 months and HPV-18 occurred at 12.6 months [18]. Based on these reports, to investigate the prevalence of vaccine targeted HPV genotypes based on vaccination history at the time of ASCUS or LSIL diagnosis, we analyzed the prevalence of HPV-16/18 genotypes according to the common HPV genotypes targeted by HPV vaccines. Consequently, we found that for at least 12 months after HPV vaccination, the prevalence of HPV-16/18 in adult women diagnosed with LSIL was significantly lower. ASCUS or LSIL stage before CIN1 is less associated with cervical cancer than CIN, and the prevalence of HPV-16/18 on ASCUS or LSIL stage is reduced compared with CIN 2+ [919]. According to previous study, vaccine-related genetic patterns (HPV-16/18) are reduced after 24 months in CIN 2+ adult female patients in the USA [20]. Similarly, we found that women diagnosed with LSIL at the stage of progression before CIN 2+ were downed in the prevalence of HPV-16/18 after 12 months from HPV vaccination.
This study has some limitations. Researchers enquired about vaccination history (the type of vaccine; number of vaccinations; and timing of the vaccination), which may have been subject to recall bias. We did not obtain the results of HPV genotypes or Pap test at the time of HPV vaccination; therefore, we do not know the change of vaccine-targeted HPV genotype after vaccination. Another limitation is that our study lacks a sufficient sample size; if a larger sample had been available, then our study could have potentially revealed more significant characteristic of HPV vaccination. However, since our data were analyzed at the start of NIP in mid-2016, we believe it is meaningful to identify the status and characteristics of HPV vaccination of Korean adult women with HPV.
Korea has strengthened its policy for preventing cervical cancer by conducting NIP for girls aged 12 years and providing cervical cancer testing for women aged ≥20 years. The results of our study will be important for confirming vaccination status before the introduction of NIP and can subsequently be used for making future policies related to HPV vaccination in Korea. To evaluate the effectiveness of these preventive projects, HPV infection status and the cervical cancer development rate among NIP recipients should be frequently monitored in this population. Studies involving the examination of populations who were not subjected to NIP, and patients with HSILs, CIN 2+, or other conditions, are warranted.
 XML Download
XML Download