

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The goal of surgery for advanced ovarian cancer is to remove intraperitoneal tumors without leaving any macroscopic residual tumors [123]. Cytoreductive surgery for advanced ovarian cancer is usually complicated and difficult as it requires removal of several organs and resection of extensive amounts of the peritoneum to achieve complete cytoreduction. Therefore, several studies have reported that the surgery should be performed by gynecologic oncologists specialized in treating advanced ovarian cancer who understand the specific behavior of the disease [45678].
However, resection of extra-gynecological lesions, such as intestinal and upper abdominal lesions, is performed by specialized gynecologic oncologists in only limited numbers of institutions [89]. Especially in Japan, gynecologic oncologists in many institutions rarely perform bowel resection and upper abdominal surgery. One reason is that they cannot take responsibility for potential complications. When the need to resect extra-gynecological organs arises, Japanese gynecologic oncologists often entrust surgery to surgeons in other departments who are experienced in resecting the specific organ. For example, they rely on gastrointestinal surgeons for bowel resection, hepatobiliary-pancreatic surgeons for splenectomy, and thoracic surgeons for resection of the diaphragm. However, multidisciplinary surgery sometimes results in inconsistent strategies, inappropriate resection lines, failure of en bloc resection, or prolonged surgical time. In addition, the time taken to schedule surgery dates between departments increases the risk of cancer progression and opportunities for cytoreductive surgery may be missed. Therefore, our previous study [10] and other reports [4] indicated that patients with resection performed by surgeons in other departments had poorer prognosis than those in whom gynecologic oncologists performed all resections.
Therefore, we implemented a monodisciplinary surgical team consisting of specialized gynecologic oncologists for advanced ovarian cancer in our institution. In the initial learning period, a gynecologic oncologist who had a certification as a general surgeon trained 2 other gynecologic oncologists in bowel resection and upper abdominal surgery for 4 years. After the initial learning period, the trained gynecologic oncologists performed surgeries for advanced ovarian cancer without the certificated general surgeon. We examined the safety of bowel resection and upper abdominal surgery in patients with advanced ovarian cancer performed by gynecologic oncologists after training in a monodisciplinary surgical team.
MATERIALS AND METHODS
1. Patients
This study was approved by the Institutional Review Board of Chiba University Graduate School of Medicine (approval number: 1163). We prospectively evaluated consecutive patients with International Federation of Gynecology and Obstetrics (FIGO) III/IV ovarian, fallopian tube, or primary peritoneal carcinoma treated at Chiba University Hospital between April 2008 and December 2017. All provided consent to undergo cytoreductive surgery performed by a surgical team consisting of gynecologic oncologists.
Patients were divided into 2 groups for the analysis. Patients in the initial learning period were treated by a monodisciplinary surgical team consisting of a gynecologic oncologist who had a certification as a general surgeon (K.K.) and 2 gynecologic oncologists (S.T. and K.N.) between April 2008 and March 2012. K.K. initially trained as a general surgeon for 10 years before receiving 4 years of training as a gynecologic surgeon. During the initial learning period, S.T. and K.N. were coached by K.K. on extra-gynecological procedures, such as bowel resection with anastomosis, stoma creation, liver mobilization, and splenectomy with distal pancreatectomy, through hands-on experience. Patients in the post-learning period were treated by a monodisciplinary surgical team consisting of three gynecologic oncologists (S.T., K.N., A.M.) without general surgeons between April 2012 and December 2017. During the post-learning period, the 2 gynecologic oncologists (S.T. and K.N.), who had acquired skills for extra-gynecological procedures from the general surgeon, passed on their training to the other gynecologic oncologist (A.M.). The members of the surgical team were fixed to the 3 surgeons during both periods.
2. Surgeons and surgery
All surgical procedure was performed by the surgical team consisting of gynecologic oncologists described above. There were exceptional cases in which hepatic parenchymal resection and cholecystectomy with severe adhesion were performed by hepatobiliary-pancreatic surgeons, and nephrectomy with atrophic kidney and total cystectomy with ileal conduit were performed by urologists.
Surgical strategies such as the range and the order of resection were decided by the surgical team through discussions. The extent of disease was preoperatively assessed using transvaginal and transabdominal ultrasonography, computed tomography, and magnetic resonance imaging. However, the timing of cytoreductive surgery was decided at the initial laparotomy as described in our previous report [10] because the extent of disease was often under or overestimated by the aforementioned imaging modalities. Briefly, primary debulking surgery was performed when the surgical team determined that complete cytoreduction was achievable at initial laparotomy. When the team determined that complete cytoreduction was not achievable as the patient required gastrectomy, resection of the hepatic hilum, resection of the head of the pancreas, massive intestinal resection, or total colectomy, and/or the patients had massive ascites caused coagulopathy, the surgeons only performed diagnostic biopsy of the ovary, fallopian tube, omentum, or peritoneum. In these cases, the surgeons marked the margins of the residual tumors (>1 cm in diameter) with nonabsorbable sutures. After neoadjuvant chemotherapy, interval debulking surgery was performed to remove the regions in which the tumors were disseminated at the initial laparotomy. Even when initial tumors were invisible, they were removed using the suture marks as landmarks. Patients in poor general condition (performance status ≥3 or ileus) and/or those aged ≥80 years received neoadjuvant chemotherapy without undergoing initial laparotomy.
Protective ileostomy after rectosigmoid resection with anastomosis or a Hartmann procedure was performed in patients using long-term steroids for autoimmune diseases or in patients with severe intestinal edema observed intraoperatively.
3. Surgical outcome
The surgical outcomes, including residual disease, operation time, estimated intraoperative blood loss and hospital days were evaluated. The complexity and extent of the surgical procedures performed were evaluated using the surgical complexity score [1112]. Based on the surgical complexity score, the surgical procedures performed were scored from 1 to 3 as follows: score 1=total hysterectomy with bilateral salpingo-oophorectomy, omentectomy, pelvic lymphadenectomy, para-aortic lymphadenectomy, pelvic and abdominal peritoneal stripping, and small bowel resection/s, score 2=large bowel resection, diaphragm stripping/resection, splenectomy, and liver resection/s, score 3=recto-sigmoidectomy with anastomosis. Based on the cumulative score, patients were stratified into the low (scores ≤3), moderate (scores 4–7), and high (scores ≥8) groups.
Perioperative complications occurring within 90 days of surgery were graded using the Clavien-Dindo classification [13]. The most severe complication, regardless of type, was defined as the grade of complications for each patient. In addition, we focused on perioperative complications related to rectosigmoid resection with anastomosis, right diaphragm resection, and splenectomy with distal pancreatectomy. These surgeries are not typically performed by general gynecologists but are frequently required in cytoreductive surgery for ovarian cancer. We excluded grade I complications related to these surgical procedures because they are not clinically problematic. Anastomotic leakage after rectosigmoid resection was defined as fecal discharge from the drain placed at cytoreductive surgery in the pelvis [14]. Symptomatic pleural effusion or pneumothorax was defined as dyspnea with pleural effusion or pneumothorax appearing on chest X-rays. Pancreatic fistula was defined as clinical symptoms (fever or left upper abdominal pain) in addition to drainage via the operatively placed drain (or a subsequently placed percutaneous drain) of any measurable volume of fluid on or after postoperative day 3, with an amylase content greater than three times the upper normal serum level: grade B or C classified by International Study Group on Pancreatic Fistula Definition [15].
Based on previous reports [161718], the cumulative sum (CUSUM) technique was used to chart the change in anastomotic leakage after rectosigmoid resection and pancreatic fistula to assess the learning curve for rectosigmoid resection and splenectomy with distal pancreatectomy. CUSUM was defined as Sn=∑(Xi-X0), where Xi was an individual attempt, and X0 was the predetermined acceptable failure rate for the procedure. Xi was assigned the following scores: score 1=failure (development of anastomotic leakage after rectosigmoid resection or pancreatic fistula) and score 0=success (no anastomotic leakage after rectosigmoid resection or pancreatic fistula). In this study, the acceptable failure rate was set at 10% (X0 was set at 0.1) for anastomotic leakage and 20% (X0 was set at 0.2) for pancreatic fistula, using previous reports as a reference [1920212223242526272829303132]. After each attempt, the score was sequentially added to the cumulative score, and the results were plotted graphically. A positive slope indicated that a failure rate exceeded the acceptable failure rate, and a negative slope indicated that a failure was within the acceptable rate.
4. Prognosis
Progression-free survival (PFS) and overall survival (OS) periods were analyzed in the 2 periods.
5. Statistics
Patient characteristics, surgical outcomes, and perioperative complications were compared between the 2 periods using the Mann-Whitney U test, Fisher's exact test, and Pearson's test. All statistical analyses were performed using JMP ver. 11 (SAS, Cary, NC, USA). The PFS and OS periods were analyzed based on the Kaplan-Meier survival curves using IBM SPSS Statistical ver. 22 (IBM Japan Services Co., Ltd., Tokyo, Japan). In all analyses, p<0.05 was taken to indicate statistical significance.
RESULTS
1. Patient characteristics
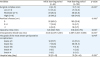
A total of 260 patients were included in this study: 65 were treated during the initial learning period, and 195 were treated during the post-learning period. Patient characteristics are summarized in Table 1. Age, FIGO stage, histology, timing of cytoreductive surgery, the initiation day of adjuvant chemotherapy and the completion rate of adjuvant chemotherapy were not significantly different between the 2 periods. The peritoneal cancer index [3334] was significantly higher in the post-learning period than the initial learning period. Performance status was significantly better during the post-learning period than during the initial learning period. The fallopian tube was identified as the primary site of the lesion in a greater number of patients during the post-learning period than during the initial learning period because the fallopian tubes were sampled using the Sectioning and Extensively Examining the Fimbriated End Protocol [35] in the pathology department during the post-learning period. Thus, the number of patients diagnosed with fallopian tube carcinoma (based on histopathological examination) was greater during the post-learning period, although the tumor macroscopically resembled an ovarian carcinoma in these patients.
Table 1
Patients characteristics

Values are presented as median (interquartile range) or number (%).
FIGO, International Federation of Gynecology and Obstetrics.
*Mann-Whitney U test; †Pearson's test; ‡FIGO 1988 classification; §Fisher's exact test for comparison between the number of high-grade serous carcinoma and those of non high-grade serous carcinoma; ∥The patients with no cytoreductive surgery were excluded.
![]()
2. Step-by-step learning approach during the learning period
During the learning period, a certificated general surgeon with additional sub-specialty training as a gynecologic oncologist (K.K.) performed rectosigmoid resection in the first 14 cases with gynecologic oncologists (S.T. and K.N.) as first assistants. After the 15th case, S.T. and K.N. worked as operating surgeons, and K.K. took over as the first assistant, or the surgeons randomly performed surgeries by rotation. K.K. performed distal pancreatectomy with splenectomy in the first 7 cases with S.T. and K.N. as first assistants. After the 8th case, S.T. and K.N. worked as operating surgeons, and K.K. took over as the first assistant, or the surgeons randomly performed the surgeries by rotation. Owing to K.K.'s limited experience with diaphragm resection, the 3 surgeons performed these surgeries as the operating surgeon by rotation. From the viewpoint of including trained experts in the team, the number of surgeons in the surgical team was fixed at three gynecologic oncologists. The three gynecologic oncologists focused on patients with ovarian cancer and avoided treating patients with other gynecological cancers (e.g., cervical and endometrial cancer) as far as possible. The gynecologic oncologists performed surgeries twice a week.
3. Surgical procedures
The surgical procedures performed in the patients in the 2 periods are summarized in Table 2. Extra-gynecological procedures were performed in 50 (76.9%) of the 65 patients in the initial learning period and 164 (84.1%) of the 195 patients in the post-learning period. The most frequently performed extra-gynecological procedure was rectosigmoid resection with anastomosis; 34 (52.3%) of 65 patients in the initial learning period and 147 (75.4%) of 195 patients in the post-learning period. In these patients, protective ileostomy was created in 5 (14.7%) and 4 (2.7%) patients, respectively (p=0.013). This was followed by right diaphragm resection (33 [50.8%] in the initial learning period and 118 [60.5%] in the post-learning period) and splenectomy (15 [23.1%] in the initial learning period and 84 [43.1%] in the post-learning period). Of 84 cases with splenectomy in the post-learning period, 82 were performed with distal pancreatectomy. Enlarged cardiophrenic lymph node resection was performed 0 during the initial learning period and in 7 (3.6%) of the 195 patients during the post-learning period.
Table 2
Surgical procedures performed

Values are presented as number (%).
*The percentage of the patients with protective ileostomy among the patients with rectosigmoid resection with anastomosis; †Two patients underwent splenectomy without distal pancreatectomy; ‡Performed by hepatobiliary-pancreatic surgeons in 4 patients; §Performed by hepatobiliary-pancreatic surgeons in 3 patients; ∥Performed by urologists in 4 patients; ¶Performed by urologists in 1 patient.
![]()
4. Surgical outcome
The rate of achieving complete removal of all gross disease after cytoreductive surgery during the post-learning period was 83.6%, which was not significantly different from the initial learning period (80.0%) (p=0.560). Although the surgical complexity score in the post-learning period was higher than that in the initial learning period (median, initial learning period: 8, post-learning period: 11, p<0.001), the operative time was not significantly different (median, initial learning period: 645 min, post-learning period: 616 min, p=0.190) and estimated intraoperative blood loss during the post-learning period was less than in the initial learning period (median, initial learning period: 3,545 mL, post-learning period: 2,087 mL, p<0.001). The rate of most severe perioperative complications with grade IIIb≥ was not significantly different between the 2 periods (initial learning period: 10.8%, post-learning period: 5.1%, p=0.140). Two patients died within 90 days of surgery during the post-learning period. One of these was a 73-year-old patient who died of multiple organ failure 57 days after primary debulking surgery, which completely resected all visible tumor. The multiple organ failure occurred following bleeding from the right external iliac artery on the 10th postoperative day, and was probably caused by the pancreatic fistula. The other was an 82-year old patient who died of aspiration pneumonia on the 4th day after diagnostic laparotomy (Table 3).
Table 3
Surgical outcome
Values are presented as median (interquartile range) or number (%).
*Mann-Whitney U test; †Pearson test; ‡Fisher's exact test for comparison between the number of grade I/II/IIIa and those of grade IIIb/IV/V.
![]()
5. Perioperative complications related to the rectosigmoid resection with anastomosis, right diaphragm resection, and splenectomy with distal pancreatectomy
Anastomotic leakage after rectosigmoid resection with anastomosis occurred in 2 (6.0%) of the 34 patients in the initial learning period, and in 12 (8.2%) of the 147 patients in the post-learning period. The rate of anastomotic leakage after rectosigmoid resection with anastomosis was not significantly different between the 2 periods (p=0.270). The decision to perform re-operation in the event of anastomotic leakage was determined by the development of peritonitis. Re-operation was also indicated in patients in whom anastomotic leakage was not adequately treated with percutaneous drainage. During the initial learning period, both patients with anastomotic leakage required re-operation to perform transverse colostomy by the colorectal surgeons. In contrast, only one patient required re-operation to create an ileostomy performed by the gynecologic oncologist and colorectal surgeons during the post-learning period. The remaining 11 patients were treated with antibiotics and percutaneous drainage by the gynecologic surgical team but did not require re-operation. Median drainage duration was 24 days after cytoreductive surgery in patients who developed anastomotic leakage with conservative management. Median interval between cytoreductive surgery and the initiation of adjuvant chemotherapy in these patients was 48 days. Both patients who developed anastomotic leakage during the initial learning period did not undergo multiple bowel resections. However, 7 of 12 patients who developed anastomotic leakage during the post-learning period underwent multiple bowel resections.
Symptomatic pleural effusion or pneumothorax after right diaphragm resection occurred in one patient in each group (initial learning period: one patient, 3.0%; post-learning period: one patient, 0.8%). The difference between the 2 periods was not significant (p=0.440).
There were also no significant differences in rates of pancreatic fistula after splenectomy with or without distal pancreatectomy between the 2 periods (initial learning period: 3 patients, 20.0%; post-learning period: 11 patients, 13.1%, p=0.520) (Table 4).
Table 4
The rate of complications related to the rectosigmoid resection with anastomosis, right diaphragm resection, and splenectomy with distal pancreatectomy

Values are presented as number (%).
*Fisher's exact test; †Two patients underwent splenectomy without distal pancreatectomy; ‡International Study Group on Pancreatic Fistula Definition.
![]()
The CUSUM curve plotted for anastomotic leakage after rectosigmoid resection showed no particular trend in the learning curve was observed over the entire study period (Fig. 1A). The CUSUM curve showed that the occurrence of anastomotic leakage was acceptable because the curve remained below the 0 line over the entire study period. The CUSUM curve plotted for pancreatic fistula showed a gradual decline over the entire study period indicating the occurrence of pancreatic fistula was acceptable (Fig. 1B).
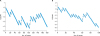 | Fig. 1(A) CUSUM curve for anastomotic leakage after rectosigmoid resection with anastomosis. The acceptable failure rate was set at 10%. No particular trend in the learning curve was observed over the entire study period. The CUSUM curve showed that the occurrence of anastomotic leakage was acceptable because the curve remained below the 0 line over the entire study period. (B) CUSUM curve for pancreatic fistula after splenectomy with distal pancreatectomy. The acceptable failure rate was set at 20%. The CUSUM curve plotted for pancreatic fistula showed a gradual decline over the entire study period indicating the occurrence of pancreatic fistula was acceptable.CUSUM, cumulative sum.
|
6. Prognosis
The median follow-up durations were 65 months (range, 0.8–130 months) in the initial learning period and 34 months (range, 0.2–85 months) in the post-learning period. The PFS for patients in the post-learning period was significantly longer than that in the initial learning period (initial learning period: 21 months, post-learning period: 34 months, median, p=0.042, log-rank, p=0.017, Wilcoxon). The OS period was not significantly different between the 2 periods (initial learning period: 68 months, post-learning period: not reached, median, p=0.186, log-rank, p=0.203, Wilcoxon) (Fig. 2).
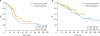 | Fig. 2Comparison of prognosis between the patients in initial learning period and post-learning period. (A) PFS, (B) OS. The PFS for patients in the post-learning period was significantly longer than that in the initial learning period (initial learning period: 21 months, post-learning period: 34 months, median, p=0.042, log-rank, p=0.017, Wilcoxon). The OS period was not significantly different between the 2 periods (initial learning period: 68 months, post-learning period: not reached, median, p=0.186, log-rank, p=0.203, Wilcoxon).PFS, progression-free survival; OS, overall survival.
|
DISCUSSION
In this study, we showed that bowel resection and upper abdominal surgery for advanced ovarian cancer can be safe when performed by gynecologic oncologists. The incidence of complications associated with bowel resection and upper abdominal surgery for advanced ovarian cancer performed by a monodisciplinary surgical team consisting of three gynecologic oncologists without general surgeons was acceptable. Although these surgical techniques are uncommon for general gynecologists, we showed that they can be performed safely by gynecologic oncologists.
Rectosigmoid resection is an important procedure for advanced ovarian cancer. In this study, among 147 patients undergoing rectosigmoid resection with anastomosis during the post-learning period, 12 patients (8.2%) experienced anastomotic leakage after surgery. This incidence rate was within the acceptable range in comparison to patients described in the literature. In previous reports, the incidence of anastomotic leakage after rectosigmoid resection did not differ significantly according to the primary tumor site or specialty of the surgeons: 0%–10% when gynecologists performed resection of ovarian cancer [81920]; 1.0%–9.8% when general surgeons performed resection of ovarian cancer [82122]; 1%–19% when colorectal surgeons performed resection of rectal cancer [232425]. As rectosigmoid resection is performed as part of the surgery for advanced ovarian cancer, total surgical time is longer and total intraoperative blood loss volume is higher than in rectal cancer surgery. Furthermore, multiple bowel resections are more commonly required in patients undergoing cytoreductive surgery for advanced ovarian cancer than in patients undergoing colon cancer surgery. Some surgeons believe that the risk of anastomotic leakage after ovarian cancer surgery is higher than the risk in patients undergoing colon cancer surgery and that protective ileostomy should therefore be performed [2136]. In the present study, however, only one patient (1/147; 0.7%) experienced aggravation of anastomotic leakage and required re-operation, even though the rate of protective ileostomy after rectosigmoid resection with anastomosis was low at 2.7% (4/147 patients). The remaining 11 patients who developed anastomotic leakage recovered completely with drainage and did not require re-operation. The number of patients who did not require re-operation was higher during the post-learning period than during the initial learning period. This observation could be attributed to the fact that intraoperative positioning of the drain and drainage management may have improved during the post-learning period. Notably, the rate of multiple anastomoses was higher during the post-learning period than during the initial learning period. However, the rate of anastomotic leakage was not significantly different between the 2 periods, and the rate of protective ileostomy was lower during the post-learning period than during the initial learning period because the intraoperative blood loss in post-learning period was less than in initial period. We showed that rectosigmoid resection with anastomosis for advanced ovarian cancer can be performed safely even without routine performance of protective ileostomy and that multiple bowel resections did not increase the risk of anastomotic leakage, which is compatible with previously reported studies describing this subject [3738].
Splenectomy is also a necessary surgical procedure for cytoreductive surgery of advanced ovarian cancer. We also performed splenectomy with distal pancreatectomy in most patients to completely remove tumors at the splenic hilum, with the incidence of pancreatic fistula being within the acceptable range at 13.1%. The reported incidence rates of pancreatic fistula following cytoreductive surgery of ovarian cancer are 13%–24% [25262728], whereas pancreatic fistula following pancreatic cancer surgery was reported to occur at rates of 30%–50% [15303132]. However, it is difficult to make a simple comparison, i.e., resection of a diseased vs. a normal pancreas and under different conditions. Pancreatic fistula is often asymptomatic and can be cured by drainage in most cases but may be aggravated. During the post-learning period, one patient experienced postoperative bleeding from the right external iliac artery that may have occurred due to pancreatic fistula. This patient had undergone left hemicolectomy along with splenectomy with distal pancreatectomy at the same time to resect bulky omental cake. We assumed that because no adhesions were formed around the resection margin of the pancreatic tail in the left upper abdominal area, the leaked pancreatic fluid flowed directly into the pelvic cavity and damaged the arteriosclerotic right external iliac artery. In the case of pancreatic cancer, hepatobiliary-pancreatic surgeons usually do not perform left hemicolectomy and splenectomy with distal pancreatectomy at the same time. Therefore, in most cases, even if pancreatic fistula develops, the pancreatic fluid will be localized by the surrounding adhesion and pancreatic fistula will consequently improve by drainage. Gynecologic oncologists should understand that cytoreductive surgery for ovarian cancer can induce complications that are beyond the experience of general surgeons or hepatobiliary-pancreatic surgeons because several organs at several sites must be removed.
Resection of the right diaphragm is also required at a high frequency for debulking surgery of advanced ovarian cancer. The incidence of complications was low, and no severe complications were observed. We believe that gynecologic oncologists can perform resection of the right diaphragm if they are well aware of the methods of liver mobilization.
Not only the incidence of complications was within the acceptable range but also prognosis during the study period was favorable. Many studies indicated that prognosis of advanced ovarian cancer is better when treated by specialized gynecologic oncologists than by general obstetricians, general gynecologists, or general surgeons [45678]. This is because specialized gynecologic oncologists are highly familiar with the characteristics of ovarian cancer and can decide on the appropriate surgical strategy by observing the entire dissemination status in the abdominal cavity. PFS of patients during the post-learning period was better than that during the initial learning period, and this finding could be attributed to the following features: 1) During the post-learning period, 64% of patients received bevacizumab as first-line treatment, whereas no patient received this medication during the initial learning period. Bevacizumab could be administered only after the Japanese public insurance system approved its use in November 2013. 2) Performance status of patients was better during the post-learning period than during the initial learning period. 3) Our hospital was categorized as a high-volume center for advanced ovarian cancer treating 32 cases/year during the post-learning period (we treated 16 cases/year during the initial learning period). Several studies have reported that high-volume centers can provide optimal treatment owing to more experienced and skilled personnel to ensure better patient care [739].
The skills required for optimal and safe bowel resection and upper abdominal surgery were acquired by performing a significant number of operations to gain experience. The gynecologic oncologists developed these skills during the initial learning period after performing rectal resection in 34 cases, diaphragm resection in 33 cases, and splenectomy with distal pancreatectomy in 15 cases. Following this course, the complication rate did not increase during the post-learning period. Rectosigmoid and diaphragm resection, as well as splenectomy with distal pancreatectomy are commonly performed during cytoreductive surgery to treat advanced ovarian cancer. Surgeries that are commonly performed are easier to learn owing to the experience gained by performing these procedures in a large number of patients. In contrast, rare surgeries are performed in a small number of patients and require a longer learning period owing to limited surgical experience. During the study period, surgeons from other departments performed procedures such as hepatic parenchymal resection, cholecystectomy, and total cystectomy with ileal conduit. These rare surgeries are required only for anatomical sites that show low rates of tumor dissemination; thus, these procedures are perhaps not required at the time of interval debulking surgery after neoadjuvant chemotherapy. Our study emphasizes that acquiring the mandatory skills to effectively and safely perform common surgeries will enable gynecologic oncologists to improve the overall quality and outcomes of cytoreductive surgery. Notably, the operative times and perioperative complication rates did not significantly differ between the 2 periods in this study. However, estimated intraoperative blood loss was lesser during the post-learning period than during the initial learning period. Moreover, we observed that the surgical complexity score was higher during the post-learning period than during the initial learning period.
The process of developing a training program to teach surgical procedures, such as bowel resection and upper abdominal surgery, to gynecologic oncologists is still under consideration internationally [940]. Our team was fortunate to have a certificated general surgeon with 4 years of experience in the gynecologic cancer department. This surgeon shared hands-on experience of bowel resection with anastomosis, stoma creation, and liver/spleen mobilization with our gynecologic oncologists. We collaborated to explore an appropriate procedure not for gastrointestinal, hepatic, or pancreatic cancer treatment but for ovarian cancer treatment. In our view, gynecologic oncologists need not receive training at the department of colorectal surgery or hepatobiliary-pancreatic surgery because surgeons at these departments do not treat ovarian cancer. Instead, it would be beneficial if a colorectal surgeon or a hepatobiliary-pancreatic surgeon join the department of gynecology because this specialty treats patients with advanced ovarian cancer. Based on the results of this study, we recommend a step-by-step approach to learning, which includes the following course: 1) initially, a gynecologic oncologist acquires specialty training in bowel resection with reconstruction or upper abdominal surgery by working as a surgical assistant under the mentorship of a colorectal surgeon or a hepatobiliary-pancreatic surgeon, 2) the gynecologic oncologist performs surgeries as an operating surgeon with the colorectal surgeon or hepatobiliary-pancreatic surgeon as an assistant and finally, 3) the gynecologic oncologist performs surgeries independently. Gynecologic oncologists are specialists who possess the skills required to perform gynecologic cancer surgery. Therefore, it is expected that a gynecologic oncologist is already familiar with basic surgical skills. Thus, learning specific bowel resection and/or upper abdominal surgery techniques is not difficult for such individuals. We also recommend that the members of the surgical team should be fixed to maintain the skills and to share the appropriate surgical strategy based on understanding of the disease-specific behavior of ovarian cancer.
It is observed that many gynecologic oncologists in Japan do not usually perform bowel resection and upper abdominal surgery, which is attributable to the medicolegal issues observed in patients who develop complications. However, anastomotic leakage and/or pancreatic fistula cannot be considered complications specific to procedures performed by gynecologic oncologists because these complications can be associated with procedures performed by surgeons from any specialty. We propose that to safeguard these surgeons against medicolegal issues, it is necessary to establish a system whereby the gynecological oncology association in each country provides certification to gynecological oncologists to treat patients with ovarian cancer. Gynecologic oncologists should be evaluated with respect to the following attributes before they are certified to treat women with ovarian cancer: a thorough understanding of ovarian cancer such as disease-specific behaviors, as well as biological characteristics, epidemiology, diagnosis, and treatment strategies available for this condition. Additionally, the surgeon's experience and technical skills need to be confirmed. General, colorectal, and hepatobiliary-pancreatic surgeons are not trained to treat ovarian cancer. Therefore, in our view, gynecologic oncologists with considerable experience in treating ovarian cancer should be certified to perform bowel resection and upper abdominal surgery in patients with ovarian cancer.
There were some limitations in this study. First, the number of patients required to confirm its safety was not clarified. It must be mentioned that the initial study period included only 65 patients over a period of 4 years because Dr. K.K. left the hospital in March 2012. We emphasize that gynecologic oncologists can learn the skills required for extra-gynecological procedures and successfully perform such operations, as was shown in this study. Second, we are still unable to predict long-term prognosis because of the short observation in the post-learning period.
In conclusion, our findings showed that surgical procedures, such as rectosigmoid resection, diaphragm resection, and splenectomy with distal pancreatectomy, are safe even when performed by gynecologic oncologists. Specialists in ovarian cancer treatment should be gynecologic oncologists and not general, colorectal, hepatobiliary-pancreatic, or respiratory surgeons. This report will be helpful for gynecologic oncologists who would like to but are currently unable to perform bowel resection and upper abdominal surgery.
 XML Download
XML Download