

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Malignancies are an important risk factor for venous thromboembolism (VTE), which includes pulmonary embolism and/or deep vein thrombosis [12]. Many patients with gynecologic cancers undergo surgery and chemotherapy, which present an additional risk for VTE [3]. Because VTE is associated with poor prognosis and decreased quality of life, adequate management is essential [456]. Although direct oral anticoagulants (DOACs) are used as one of the standard therapies for VTE in the general population, low-molecular weight heparin (LMWH) has become the standard therapy for cancer-associated VTE, following the results of the landmark CLOT trial [789]. Although there is no firm evidence supporting the use of DOACs, the convenience of use means that these agents have been increasingly used in cancer patients [810].
In 2 randomized controlled studies, which compared edoxaban and rivaroxaban with dalteparin, non-inferior safety and efficacy were seen in patients with cancer-associated VTE, although clinically relevant non-major bleeding events were higher in the edoxaban and rivaroxaban groups [1112]. However, because patients with gynecologic cancers represented only 10% of the patient population in these studies, it is difficult to apply the non-inferiority data relating to DOACs to gynecologic cancers.
Several studies have reported higher rates of uterine and/or other genital tract bleeding in patients treated with DOACs when compared with other anticoagulants [131415]. DOACs also cause more clinically relevant bleeding in women than in men during the treatment of acute VTE [1617]. In addition, mucosal lesions in visceral malignancies are associated with increased bleeding risk [18]. Considering these factors, the use of DOACs should be further evaluated in patients with gynecologic cancers, which are associated with several bleeding risk factors. Among direct factor Xa inhibitors, rivaroxaban is associated with a greater risk of bleeding [1920].
In this study, we compared the incidence of composite events, including clinically relevant bleeding and recurrence, in patients with primary gynecological cancers who were prescribed either rivaroxaban or dalteparin for the treatment of cancer-associated VTE. In addition, the incidence of bleeding events, recurrence, and all-cause mortality was assessed.
METERIALS AND METHODS
1. Study design and patients
This study was performed at the Asan Medical Center in Korea and involved a review of the electronic medical records of patients diagnosed with gynecologic malignancy and VTE who were prescribed dalteparin or rivaroxaban therapy. Because there is no standardized protocol for anticoagulant selection, the decision to prescribe rivaroxaban or LMWH is the responsibility of the individual clinician at the study center.
Inclusion criteria were as follows: 1) diagnosis of ovarian, cervical, uterine, vaginal, vulvar, endometrial, or fallopian tube cancer; 2) presence of VTE, as diagnosed via computed tomography or lower extremity Doppler ultrasonography by certificated radiologists; and 3) treatment of VTE with a standard dose of rivaroxaban or dalteparin between January 1, 2012, and December 31, 2017. Exclusion criteria were as follows: 1) anticoagulant therapy initiated at another institution; 2) rivaroxaban or dalteparin use for ≤7 days without bleeding events; 3) patients lost to follow-up after the first visit; and 4) venous thromboembolic lesions removed by surgery.
The Institutional Review Board of the Asan Medical Center (IRB No. 2017-0652) approved this study. The requirement for informed consent was waived due to the retrospective nature of the analysis.
2. Measurements
Baseline patient characteristics and outcomes were obtained by review of the electronic medical records. The score for bleeding risk factors was calculated as the sum of the number of risk factors, including surgery, in the 2 weeks prior to anticoagulant therapy, concurrent use of antiplatelet agents, presence of a primary or metastatic brain tumor, regionally advanced or metastatic cancer, coexisting gastrointestinal or urothelial cancer, and bevacizumab use in the 6 week period before anticoagulant treatment [11].
The primary outcome in this study was a composite event, which included any one of the following: recurrence, major bleeding, or clinically relevant non-major bleeding events during the therapeutic period. Recurrence of VTE was confirmed by computed tomography or ultrasonographic evidence of an occurrence or increase in pulmonary embolism or deep vein thrombosis at new sites during anticoagulant therapy [11]. Major bleeding was defined as any bleeding event during the therapeutic period that 1) was associated with death; 2) occurred at the fatal site (including intracranial, intraocular, retroperitoneal, intraspinal, or pericardial area); or 3) required a transfusion of at least 2 units of packed red blood cells or led to a decreased hemoglobin level of at least 2.0 g/dL [21]. Any overt bleeding events during the therapeutic period with rivaroxaban or dalteparin that did not meet the criteria for major bleeding but resulted in medical attention, unappointed visits, discontinuation of anticoagulants, or a decrease in daily activities were defined as clinically relevant non-major bleeding [22]. Recurrence, any bleeding events, clinically relevant non-major bleeding, major bleeding, and all-cause mortality were analyzed as secondary outcomes. Recurrence, any bleeding events, clinically relevant non-major bleeding, and major bleeding events were analyzed during therapeutic periods, and all-cause mortality was analyzed until March 31, 2018. Clinically relevant bleeding events included both major bleeding events and clinically relevant non major bleeding events.
3. Data collection and statistical analysis
Categorical variables are presented as number (%) number and continuous variables as the mean and standard deviation. Differences between the 2 treatment groups were analyzed by the χ2 test or Fisher's exact test and Student's t-test. Time-to-event curves were calculated by Kaplan-Meier analysis with a log-rank test.
A Cox proportional hazard model was used for univariate and multivariate analysis. Covariates that showed a significant difference between the study groups (p<0.2) were selected. All analyses were performed using SPSS software (version 24.0; IBM, Armonk, NY, USA). The p-values <0.05 were considered as indicative of statistical significance.
RESULTS
1. Study flow and baseline characteristics
Between January 2012 and December 2017, 186 patients with gynecologic cancers were diagnosed with pulmonary embolism and/or deep vein thrombosis. Of these, 24 were excluded: 11 patients were prescribed rivaroxaban or dalteparin for <7 days, 7 patients were transferred to other hospitals after the first prescription, 5 patients were first prescribed anticoagulants at other hospitals, and one patient underwent surgery to remove a thromboembolic lesion (Fig. 1).

Of the remaining 162 eligible patients, 60 patients were treated with dalteparin and 102 patients received rivaroxaban. The baseline characteristics and bleeding risk factor scores of patients treated in the 2 treatment groups are shown in Table 1. No significant differences in baseline characteristics were seen, with the exception of pulmonary embolism, which was more common in patients receiving dalteparin than in those receiving rivaroxaban (88.3% vs. 47.1%, p<0.001).
Table 1
Baseline characteristics of the study cohort
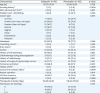
Values are presented as number (%) or mean±standard deviation. Differences between both groups were analyzed by the χ2 test, Fisher's exact test, or independent 2-sample t-test.
GFR, glomerular filtration rate; IVC, inferior vena cava; VTE, venous thromboembolism.
*Variables analyzed by Fisher's exact test.
![]()
2. Study outcomes
During the treatment period, composite events were more common in the rivaroxaban group, but without statistical significance (29.4% in the rivaroxaban group vs. 20.0% in the dalteparin group, p=0.187; Table 2). Although patients in the rivaroxaban group experienced more bleeding events of any type (24.5% vs. 15.0% in the dalteparin group, p=0.151), no statistically significant differences were seen in major bleeding events (7.8% vs. 5.0% in the dalteparin group, p=0.748) or clinically relevant non-major bleeding events (16.7% vs. 10.0% in the dalteparin group, p=0.240). Recurrence, symptomatic recurrence, and all-cause mortality also showed no significant differences between the 2 groups. No patient deaths due to VTE or bleeding were reported. In the dalteparin group, patients with a history of surgery for gynecologic cancer showed an incidence of 7.0% for major bleeding and 18.6% for clinically relevant bleeding. Patients with no history of surgery for gynecologic cancer showed an incidence of 5.9% for clinically relevant bleeding and no major bleeding events. In the rivaroxaban group, patients with a history of surgery for gynecologic cancer showed an incidence of 6.2% for major bleeding and 24.7% for clinically relevant bleeding. Patients with no history of surgery for gynecologic cancer showed an incidence of 14.3% for major bleeding and 23.8% for clinically relevant bleeding (Supplementary Table 1).
Table 2
Primary and secondary endpoints in both groups
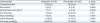
Values are presented as number (%). Differences between both groups were analyzed by the χ2 test or Fisher's exact test.
CRNM, clinically relevant non-major.
*Variables analyzed by Fisher's exact test.
![]()
Fig. 2 shows Kaplan-Meier curves of time to composite events among patients treated with either rivaroxaban or dalteparin, compared using the log-rank test. There was no significant difference in time to composite events between the 2 groups (p=0.360). Using a Cox proportional hazards models, univariate and multivariate analyses of the incidence and timing of the composite events during the therapeutic period were performed (Table 3). A history of radiotherapy and pulmonary embolism were included as covariates, which showed significant differences between the study groups with p-values <0.2. The hazard ratio (HR) for composite events among patients receiving rivaroxaban vs. patients receiving dalteparin was 1.369 in the univariate analysis (95% confidence interval [CI]=0.697–2.688; p=0.362) and 1.576 in the multivariate analysis (95% CI=0.752–3.305; p=0.229). Covariates, including a history of radiotherapy and accompanying pulmonary embolism, also showed no significant differences.
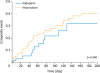 | Fig. 2Kaplan-Meier cumulative event rates for the composite event. There was no significant difference in time to composite events between dalteparin and rivaroxaban (p=0.360).
|
Table 3
HR for the composite event in the Cox proportional hazards model

![]()
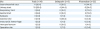
Table 4 shows the HRs for the clinically relevant bleeding events using a Cox proportional hazards model. In this analysis, rivaroxaban was associated with an increased HR of clinically relevant bleeding vs. dalteparin in univariate (HR=1.450; 95% CI=0.673–3.126; p=0.343) and multivariate analysis (HR=1.445; 95% CI=0.614–3.398; p=0.399). However, there was no statistically significant difference between the groups.
Table 4
HRs for clinically relevant bleeding events using the Cox proportional hazards model

![]()
Table 5 shows the sites of bleeding events. Nine patients receiving dalteparin presented with clinically relevant bleeding events; of these, the urinary tract (44.4%) was the most common, followed by the injection site (22.2%). Among patients receiving rivaroxaban, 25 patients developed clinically relevant bleeding events; the gastrointestinal tract was the most common bleeding site (44.0%), followed by the urinary tract (24.0%).
Table 5
Location of bleeding sites in patients treated with either dalteparin or rivaroxaban
![]()
DISCUSSION
Two randomized controlled studies comparing the outcome of DOACs and LMWH treatment for cancer-associated VTE have previously been performed [1112]. Following these studies, several guidelines were published recommending that DOACs could be considered as an alternative to LMWH for the treatment of cancer-associated VTE [810]. However, patients with a variety of cancer types were included in these studies and additional studies are required to evaluate the efficacy and safety of DOACs for VTE in each cancer type. As the urinary tract is commonly invaded by gynecologic cancer and one of the most important bleeding risk factors associated with DOACs in cancer patients is visceral lesions in the urinary or gastrointestinal tracts, it is important to determine the safety of DOACs in patients with gynecologic cancer [18].
To our knowledge, only one pilot analysis has compared the risk of rivaroxaban and enoxaparin for the treatment of VTE in gynecologic cancers [23]. Although there was no significant difference in effectiveness or safety between the 2 drugs, the authors urged caution when drawing any conclusions due to the small sample size, which included 18 patients in the rivaroxaban group and 26 in the enoxaparin group. In the current study, we compared rivaroxaban and dalteparin in a larger number of patients with gynecologic cancers.
In the current study, the dalteparin group included more patients with accompanying pulmonary embolism than the rivaroxaban group. However, other baseline characteristics did not differ. A history of radiotherapy and accompanying pulmonary embolism were selected as covariates for the multivariate analysis; although rivaroxaban presented a 1.576 (95% CI=0.752–3.305)-fold increase in risk for the composite event when compared with dalteparin, this difference did not reach statistical significance.
There are 2 previous studies of rivaroxaban for the treatment of patients with gynecologic cancers and VTE [2324]. Although the current study included a larger number of patients than these, we found no significant differences in bleeding incidence and recurrence rates between rivaroxaban and dalteparin, which is standard therapy for cancer-associated VTE. These data indicate that rivaroxaban can be regarded as a reasonable option for the treatment of cancer-associated VTE in patients with gynecologic cancers.
In other previous studies, concern has been raised that rivaroxaban is associated with an increased risk of bleeding in comparison with other DOACs therapies [1920]. In the current study, clinically relevant bleeding occurred in 24.5% of patients receiving rivaroxaban and 15.0% of patients receiving dalteparin. However, after adjustment, rivaroxaban was not associated with an increased HR for clinically relevant bleeding. Although other DOACs were not included in this study, these results suggested that other DOACs, which have less bleeding tendency than rivaroxaban, may also be used for cancer-associated VTE.
Concern has also been raised that DOACs may increase gastrointestinal bleeding compared with other anticoagulants [252627]. While the exact mechanism for increased gastrointestinal bleeding is not fully understood, several hypotheses have been proposed. DOACs are actively secreted into the gastrointestinal tract via the P-glycoprotein transport system [28]. Part of the DOACs have low bioavailability, and secreted and unabsorbed DOAC compounds are activated in the gastrointestinal tract [29]. Continued exposure of the gastrointestinal tract to active DOAC compounds can increase the risk of gastrointestinal tract bleeding. In the current study, among the 25 patients with bleeding in the rivaroxaban group, 11 (44.0%) presented with gastrointestinal bleeding. By contrast, there were no patients with gastrointestinal bleeding in the dalteparin group. These findings are similar to those of previous studies of rivaroxaban [252930], and suggest that clinicians should consider other gastrointestinal bleeding risk factors before prescribing rivaroxaban, such as concomitant use of ulcerogenic agents, patient age, the presence of renal impairment or peptic ulcers, or high hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalized ratio, elderly, drugs/alcohol concomitantly (HAS-BLED) scores [31].
There are several limitations to the current study. First, the retrospective design may have introduced selection bias, although the similarity in baseline characteristics between the 2 groups may reduce this risk. Secondly, most clinicians did not prescribe imaging studies for the evaluation of VTE recurrence and information regarding clinically relevant bleeding events was collected through electronic medical records. Therefore, it is possible that asymptomatic recurrences or clinically relevant non-major bleeding events were underestimated. Finally, this study included a relatively small number of patients. Therefore, a large, randomized, controlled study would be required to confirm the effectiveness and safety of rivaroxaban for the treatment of VTE in patients with primary gynecologic cancers.
In conclusion, no significant differences in effectiveness or safety were seen between patients with gynecologic cancers receiving rivaroxaban or dalteparin for the treatment of cancer-associated VTE. Rivaroxaban may, therefore, be regarded as a suitable treatment option for VTE associated with gynecologic cancers. However, as rivaroxaban treatment was associated with a higher incidence of the composite event and clinically relevant bleeding, clinicians should be cautious when prescribing rivaroxaban for cancer-associated VTE in gynecologic cancers and bleeding events and recurrence should be carefully monitored. Further prospective studies in larger patient groups will be required to clearly evaluate the safety and effectiveness of DOACs and LMWH for the treatment of VTE in patients with gynecologic cancers.
 XML Download
XML Download