

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Lymphatic dissemination to the regional lymph nodes (LNs) has been defined as the major route of metastasis in cervical carcinoma [12]. However, nodal status has recently been included in the 2018 International Federation of Gynecology and Obstetrics (FIGO) classification system which currently assigns women with positive pelvic LNs only as stage IIIC1, and women with para-aortic nodal disease as stage IIIC2 [3]. Accurate information about LN status has become a crucial clinical issue for assigning patients into proper stages in order to report realistic survival outcomes in the light of the new FIGO staging system for carcinoma of the cervix.
LN involvement is the strongest independent prognosticator of decreased survival for women with cervical cancer receiving radical surgery [4567]. Lymph node ratio (LNR) has been described as the percentage of metastatic LNs to total nodes recovered and it has been suggested as a newly emerging prognostic factor in cervical cancer during the last decade [891011121314151617]. Ratio-based nodal disease seems to be a relatively more objective measure of nodal tumor burden compared to number-based nodal category, and LNR may obviate possible confounding effect related to the number of regional LNs that varies in each individual [18]. Additionally, LNR has been shown to be more discriminative than the number of metastatic LNs in order to predict overall survival (OS) in node-positive cervical cancer [911]. However, nodal count stands as the most important parameter that needs to be satisfied in order to yield LNR as a reliable product [12]. LNR has been reported to be most meaningful in the case of performing systematic LN dissection [19].
Previous reports focusing on the prognostic value of LNR in cervical cancer seem to suffer from limited number of patients [891314], low median number of LNs recovered [913], heterogeneous patients and adjuvant treatment characteristics [891011121314151617], performance of para-aortic lymphadenectomy in selected cases [111213141617], and lack of para-aortic LN dissection in some studies [1015]. Hence, it is hard to claim that LNR was determined as a reliable measure of nodal tumor burden in previous studies since LNR is mainly dependent on the extent of LN dissection. Additionally, in several studies defining LNR as an independent prognostic factor, univariate and multivariate analyses included node-negative patients as well as node-positive patients [10121415]. As far as we know, no data have been published to show the prognostic significance of LNR in node-positive cervical cancer patients triaged to primary surgery including both pelvic and para-aortic LN dissection uniformly.
In this background, this dual-institutional retrospective study was carried out for clarifying the prognostic value of LNR in node-positive cervical cancer based on a cohort of women who had been uniformly treated with radical hysterectomy plus systematic retroperitoneal LN dissection followed by standard radiochemotherapy. The objective of the current study was to evaluate the prognostic significance of LNR in 2018 FIGO stage IIIC carcinoma of the uterine cervix.
MATERIALS AND METHODS
Consecutive cases with 2009 FIGO stage IB1–IIA2 cervical cancer those had undergone radical hysterectomy with systematic retroperitoneal LN dissection between January 1st, 2006 and September 30th, 2018 at 2 high-volume gynecologic cancer centers Ankara, Turkey. All cases were reviewed retrospectively after receiving Institutional Review Board approval (60401.02/8021). At admission, an informed consent that permitted the use of clinical data for research purposes was obtained from each patient included in the study.
The inclusion criteria were as follows: node-positive cervical cancer patients according to the final pathology report, lymphadenectomy sites including both pelvic and para-aortic chains, histological type diagnosed as squamous cell carcinoma, adenosquamous cell carcinoma or adenocarcinoma, no neoadjuvant chemotherapy as well as no synchronous malignancies at diagnosis. We excluded women with rare histologies, patients with incomplete medical records and those who received inadequate lymphadenectomy (less than 10 pelvic and 5 para-aortic nodes according to the final pathology reports). Women who received pelvic lymphadenectomy only, those who did not complete standard adjuvant treatment, and women with intraperitoneal disease detected during surgery were also excluded.
The following data were abstracted from the patients' medical records: age, histologic type, primary tumor size in greatest dimension (cm), depth of stromal invasion, lymphovascular space invasion (LVSI) (absent/present), microscopic parametrial invasion (yes/no), vaginal involvement (yes/no), vaginal surgical margins (negative/positive), ovarian metastasis (yes/no), uterine corpus invasion (either myometrial or endometrial) (yes/no), number of LNs removed (total/pelvic/para-aortic), number of metastatic LNs, and stage of disease. The date of surgery, adjuvant treatment types (external beam radiation therapy [EBRT] with concurrent chemotherapy ± brachytherapy, extended field radiotherapy with concurrent chemotherapy ± brachytherapy), recurrent disease, duration of follow-up and final status of the patients were recorded.
Gynecologic oncologists performed all of the operations. All of the patients underwent open surgery consisting of radical hysterectomy with pelvic and para-aortic LN dissection. Radical hysterectomy was performed in accordance with Piver's type III hysterectomy. The surgical procedure was terminated if intraperitoneal disease was detected during surgery. However, the operation was not abandoned in case of detecting any bulky LNs during surgical exploration. Pelvic LN dissection was performed in a standard fashion and the LNs in the obturator, external, common iliac, and presacral nodal stations were removed. Para-aortic LN dissection was performed using the same method at both centers whereby the pre-aortic, lateral aortic, interaortico-caval, lateral caval and pre-caval nodes up to the left renal vein were removed.
Conventional pathology was used for diagnosis in both of the centers. We retrieved all of histological data from the report of the primary pathologist, and we did not centrally review that pathologic data. No ultra-staging was performed. The depth of cervical stromal invasion was measured in terms of millimeters, and then fractioned into thirds. We defined deep cervical stromal invasion as a tumor that invaded the outer third of the cervical stroma. We considered LVSI to be positive when the tumor cells were noted within endothelium-lined spaces [20]. Stage was retrospectively assessed according to the revised 2018 FIGO staging system in the light of pathological findings.
Multidisciplinary tumor boards at each institution decided about adjuvant treatment options. Women with pelvic LN metastasis received adjuvant radiotherapy of whole pelvic EBRT at a dose of 45–50 Gy plus cisplatin 40 mg/m2 weekly, administered systemically during the period of EBRT. All patients with documented para-aortic LN metastasis received chemoradiation. Extended-field radiotherapy delivered 45–50 Gy to the pelvis and para-aortic area over 5 weeks at 1.8–2 Gy per fraction, using a 4-field arrangement in the pelvis and anterior and posterior fields in the para-aortic area. Concurrent cisplatin (40 mg/m2) was administered on a weekly basis. Vaginal brachytherapy was added when there is vaginal involvement or the vaginal margin was insufficient or positive. Vaginal brachytherapy was delivered by cylinders to the upper 4 cm of the residual vagina and included 3 fractions of high dose rate (HDR) brachytherapy of 7 Gy every other day, each prescribed to 5 mm from the vaginal cylinder surface.
Recurrent disease was defined as documentation of metastasis with physical examination and/or imaging techniques after a disease-free survival (DFS) > 3 months. DFS was defined as the duration in months between the date of surgery and the date of first recurrence or the date of death from any cause, whichever occurred first, or the date of last visit for patients alive without recurrence. Patients alive with no evidence of disease were censored at the date they were last known to be alive in DFS analyses. The duration in months between the date of surgery and the date of death from any cause or the date of last contact was defined as OS. Patients alive at the last known follow-up were censored in OS analyses.
LNR, described as the number of metastatic LNs divided by the total number of LNs harvested, was classified into 2 groups as LNR <0.05, and LNR ≥0.05. A cut-off value of 0.05 was chosen for LNR because it represented the median LNR of the cohort. Hence, the patients were classified as women with LNR <0.05 and those with LNR ≥0.05.
Statistical Package for Social Sciences version 23.0 (IBM Corp., Armonk, NY, USA) was used for performing all statistical analyses. Continuous variables were expressed in terms of medians and ranges, whereas binary variables were reported in terms of counts and percentages. The Kaplan-Meier method was used in order to generate survival curves, and the log-rank test was applied for detecting differences between survival curves. To determine prognostic factors for DFS and OS, a univariate Cox-regression analysis was performed. Statistically significant variables with a p-value <0.05 in univariate analyses were included in a backward conditional stepwise Cox proportional hazard model for multivariate analysis. A p-value <0.05 was considered to indicate statistical significance.
RESULTS
Two hundred-thirteen women diagnosed with 2018 FIGO stage IIIC cervical cancer were treated at two participating institutions during the study period. We excluded nine women who received neoadjuvant chemotherapy, 4 patients with inadequate lymphadenectomy, one with synchronous renal cell carcinoma, 2 women with rare histologies (1 with glassy cell carcinoma, and 1 with neuroendocrine small cell carcinoma) and three women with incomplete medical records. Six women who were unable to complete adjuvant radiochemotherapy because of medical comorbidities and 3 patients who received pelvic lymphadenectomy only were also excluded. Finally, 185 women with node-positive cervical cancer fulfilled the inclusion criteria.
One hundred thirty-eight (74.6%) women were diagnosed with stage IIIC1 disease whereas 47 (25.4%) had stage IIIC2 cervical cancer. At diagnosis, the median age of the participants was 50 (range, 31–81) and the median duration of follow-up for survivors was 45.5 months (range 3–135 months). The clinicopathological characteristics of the cohort are summarized in Table 1.
Table 1
Clinicopathological characteristics of 185 cervical cancer patients with 2018 FIGO stage IIIC cervical carcinoma

Values are presented as median (range) or number of patients (%).
FIGO, International Federation of Gynecology and Obstetrics; LN, lymph node; BSO, bilateral salphingo-oopherectomy; USO, unilateral salphingo-oopherectomy; EBRT, external beam radiation therapy; LNR, lymph node ratio.
![]()
The median number of total dissected LNs was 43.0 (range, 17–138). The median number of pelvic and para-aortic LNs recovered was 30.0 (range, 10–97) and 11.0 (range, 5–52), respectively. Concurrent pelvic and para-aortic LN metastases were found in 43 (23.2%) women, while pelvic LN involvement only was detected in 138 (74.6%) women and isolated para-aortic LN metastasis in 4 (2.2%) women. The median number of positive LNs was 2.0 (range, 1–73).
The median LNR of the study population was 0.054 (range, 0.008–1.0). A total of 88 (47.5%) women had LNR <0.05 and 97 (52.5%) women had LNR ≥0.05. The 5-year DFS rate for LNR <0.05 was 78.2%, whereas this figure was 48.8% for women with LNR ≥0.05 (p<0.001) (Fig. 1). Additionally, the 5-year OS rates for LNR <0.05 and LNR ≥0.05 were 80.6%, and 61.2%, respectively (p=0.007) (Fig. 2). Decreased survival outcomes were significantly associated with increased LNR values.
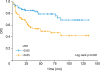 | Fig. 1DFS analyses with regard to LNR (LNR ≤0.05, n=88; vs. LNR >0.05, n=97).DFS, disease-free survival; LNR, lymph node ratio.
|
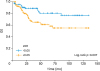 | Fig. 2OS analyses with regard to LNR (LNR ≤0.05, n=88 vs. LNR >0.05, n=97).OS, overall survival; LNR, lymph node ratio.
|
Univariate analysis revealed that decreased 5-year DFS was significantly associated with non-squamous histology (p<0.001), microscopic parametrial involvement (p<0.001), primary tumor diameter ≥4.0 cm (p=0.010), vaginal involvement (p=0.004) and LNR ≥0.05 (p<0.001), FIGO stage IIIC1 vs. IIIC2 (p=0.007) (Table 2). On multivariable analyses, non-squamous histology (hazard ratio [HR]=2.33; 95% confidence interval [CI]=1.38–3.94; p=0.002), and LNR ≥0.05 (HR=2.12; 95% CI=1.15–3.90; p=0.015) were defined as independent prognostic factors for decreased DFS in women with 2018 FIGO stage IIIC cervical cancer (Table 2).
Table 2
Univariate and multivariate analyses of 185 women with 2018 FIGO stage IIIC cervical cancer with regard to DFS

FIGO, International Federation of Gynecology and Obstetrics; DFS, disease-free survival; HR, hazards ratio; CI, confidence interval; SCC, squamous cell carcinoma; AC, adenocarcinoma; ASC, adenosquamous carcinoma; LVSI, lymphovascular space invasion; LN, lymph node; BSO, bilateral salpingo-oophorectomy; USO, unilateral salpingo-oophorectomy; LNR, lymph node ratio.
![]()
Univariate analysis revealed that decreased 5-year OS was significantly correlated with non-squamous pathology (p=0.021), microscopic parametrial involvement (p=0.012), primary tumor diameter ≥4.0 cm (p=0.04), vaginal involvement (p=0.002) and LNR ≥0.05 (p=0.007) (Table 3). On multivariate analysis, vaginal involvement (HR=2.09; 95% CI=1.05–4.13; p=0.034), and LNR ≥0.05 (HR=1.95; 95% CI=1.01–3.77; p=0.046) appeared to be independent prognostic factors for decreased OS (Table 3).
Table 3
Univariate and multivariate analyses of 185 women with 2018 FIGO stage IIIC cervical cancer with regard to OS

FIGO, International Federation of Gynecology and Obstetrics; OS, overall survival; HR, hazards ratio; CI, confidence interval; SCC, squamous cell carcinoma; AC, adenocarcinoma; ASC, adenosquamous carcinoma; LVSI, lymphovascular space invasion; LN, lymph node; BSO, bilateral salphingo-oopherectomy; USO, unilateral salphingo-oopherectomy; LNR, lymph node ratio.
![]()
When LNR was considered as a continuous variable, there was a significant association between LNR and DFS in univariate analysis (p<0.001). The HR of LNR for DFS is 1.014 (95% CI=1,003–1,025; p=0.012); so, 1% increase in LNR associates with 1,014-fold increase in the hazard in multivariant analysis. We could not present a significant association between LNR and OS in univariant analysis (p=0.059).
During the study period, there were 40 (21.6%) recurrences and 45 (24.3%) deaths in our cohort. The 5-year DFS rate was 62.5% (95% CI=77.1–95.9 months= standard error [SE]=4.78) whereas the 5-year OS rate was 70.4% (95% CI=90.4–108.0 months; SE=4.49) for the entire cohort.
DISCUSSION
Our findings indicated LNR ≥0.05 as an independent prognostic factor for both DFS and OS in node-positive cervical cancer patients triaged to primary surgical treatment by radical hysterectomy with systematic pelvic and para-aortic LN dissection followed by adjuvant chemoradiation. A LNR ≥0.05 seems to be associated with a nearly two-fold increased risk of recurrence and death in this specific patient population.
The reader should note that the current study is limited inherently by its retrospective nature. Performance of routine rather than selective para-aortic lymphadenectomy might have caused over-treatment in most of our patients. Lack of a centralized histologic analysis as well as lack of ultrastaging seems to be the major shortcomings of the present study. However, to the best of our knowledge, this is the first study focusing on the prognostic value of LNR in node-positive cervical cancer patients who had undergone systematic pelvic and para-aortic LN dissection uniformly.
Theoretically, the number of metastatic LNs directly depends on the number of LNs removed [17] and a higher number of examined LNs can assess nodal status more accurately [21]. However, the minimum number of LNs that should be harvested in order to qualify a lymphadenectomy as “adequate” is still a matter of debate [2]. Removal of more than 11 pelvic LNs has been suggested as one of the quality indicators of pelvic lymphadenectomy [22] whereas Benedetti Panici et al. [23] reported the number of LNs needs to be removed ranging from 25 to35 during cervical cancer surgery. Kesic [24] reported the nodal involvement rate as 10.5% when less than 20 nodes were removed, whereas it increased up to 26.5% when more than 50 nodes were examined. However, the total number of LNs removed is not only dependent on the thoroughness of LN dissection but also on the comprehensiveness of the pathological examination as well as the nodal yield of the specific patient [25]. Nonetheless, it should be emphasized that all of the patients in our study received systematic pelvic and para-aortic LN dissection with a median of 43 (range, 17–138) LNs recovered.
Although LNR has been recognized as a parameter which has the advantage of reflecting the number of metastatic LNs as well as the extent of LN dissection [17], LNR may appear relatively high in the case of a limited nodal count although it is actually far away from reflecting the real nodal tumor burden. For example, a woman diagnosed with 2 metastatic LNs with a total nodal count of 4 would have a LNR of 0.50 though the quality of lymphadenectomy is still questionable in this clinical scenario. In such a case, it seems impossible to guess whether the probable poor survival outcomes are associated with a high LNR or metastatic foci left behind. For this reason, we only included women who had at least 10 pelvic and at least 5 para-aortic LNs removed on their final pathology reports in our study. It should be highlighted that all of the previous studies focusing on the prognostic value of LNR in cervical carcinoma[891011121314151617] reported the range of LNs recovered with a minimum of “1” or “2” nodes whereas this figure was “17” in the present study.
On the contrary, more extensive LN dissection may cause low LNR which has been correlated with better survival outcomes. Zhou et al. [21] included 11,830 women with stage IA2–IIA cervical cancer in their study and evaluated the impact of the removed LN count on the prognosis of cervical cancer. The Zhou study revealed that removed LN count was an independent prognostic factor for survival, especially in node-positive patients. The authors [21] showed that higher number of removed LNs was associated with better cause-specific survival (HR=0.981; 95% CI=0.973–0.990; p<0.001) and OS (HR=0.985; 95% CI=0.978–0.992; p<0.001) in cervical cancer patients with metastatic LNs. Also, it was suggested that the risk of LN metastasis significantly increases in women with more than 30 LNs examined, and the authors reported that a higher number of examined LNs may reduce the risk of occult metastasis. Adequate assessment of LNs in cervical cancer is crucial because the decision and extent of adjuvant therapy are guided by the LN status [16].
The major characteristic of our study that distinguishes it from previous studies [891011121314151617] is the performance of para-aortic lymphadenectomy uniformly for the entire cohort. Although performance of para-aortic LN dissection is optional with no concrete recommendations for para-aortic LN dissection at the time of radical hysterectomy [26], it seems unacceptable not to take para-aortic chain into account, which is a potential site of metastasis, while evaluating the prognostic significance of LNR in node-positive cervical cancer. In most of the previous studies [111213141617] para-aortic lymphadenectomy was performed in selected cases, whereas it was totally omitted in some studies [1015]. However, it is well known that para-aortic LN involvement generally occurs as a consequence of pelvic LN metastases [2728]. Additionally, the rate of para-aortic LN involvement among cervical cancer patients undergoing radical hysterectomy has been reported to range from 8% to 10% [293031]. In this background, ignorance of para-aortic nodal status [1015] or slicing LNR into pelvic or para-aortic components [16] seem to have no rationale while evaluating the prognostic significance of LNR in node-positive cervical carcinoma.
LNR has been shown to be significantly correlated with survival in cervical cancer [911131516]. Polterauer et al [9] reported LNR >0.1 to be an independent prognosticator for both DFS (HR=2.2; 95% CI=1.1–4.7; p=0.01) and OS (HR=2.2; 95% CI=1.0–4.8; p=0.05). However, their cutoff value of 0.1 was based on a study of esophageal cancer. It should be emphasized that node-positive cervical cancer patients with locally-advanced disease (2009 FIGO stages IIB to IVA) were also included in their cohort of 88 patients. Inclusion of patients with locally-advanced disease might have affected their findings.
Chen et al. [11] found that the 5-year OS rate of patients with a LNR >0.1 was significantly worse than that of women with LNR ≤0.1 (11.8% vs. 42.9%, respectively) in a series of 120 node-positive women who had received type III hysterectomy and pelvic LN dissection. It should be noted that 75% of their patients had received neo-adjuvant chemotherapy before surgery. To what extent their treatment outcomes might have been affected by neoadjuvant chemotherapy seems to be the major shortcoming of that study.
In a series of 95 node-positive patients [13], it has been reported that a LNR>0.66 is associated with an approximately 3-fold increased risk of recurrence (HR=2.97; 95% CI=1.26–7.02; p=0.01) whereas a LNR>0.76 is associated with an approximately 4-fold increased risk of death (HR=3.96; 95% CI=1.31–11.98; p=0.01). It should be emphasized that 45 (47%) out of 95 patients received para-aortic LN dissection in that study.
Li et al. [15] reported on 198 women with node-positive squamous cell cervical carcinoma and suggested that a LNR >0.2 was an independent prognostic factor for both DFS (HR=2.4; 95% CI=1.2-4.8; p=0.01) and OS (HR=2.56; 95% CI=1.27–5.14; p=0.008). The median number of recovered LNs was 16 (range, 2–31) in that series whereas none of their patients underwent para-aortic lymphadenectomy.
In the current study of 185 consecutive node-positive women who had undergone radical hysterectomy with systematic retroperitoneal LN dissection followed by adjuvant chemoradiation, we have shown that a LNR ≥0.05 was an independent prognostic factor for both DFS (HR=2.12; 95% CI=1.15–3.90; p=0.015) and OS (HR=1.95; 95% CI=1.01–3.77; p=0.04). The inclusion of women receiving para-aortic lymphadenectomy in the present study might have led to the low cutoff determined for LNR (0.05) when compared with previous studies [910111516]. However, we have performed statistical analyses for LNR cutoff values chosen as 0.1 and 0.15 in order to compare our survival outcomes with previous studies. It was not surprising to find out that the 5-year DFS rate for LNR ≤0.1 was significantly better than that of LNR >0.1 (70.5% vs. 43.0%, respectively; p<0.001) in our cohort. Moreover, the 5-year OS rate for LNR ≤0.1 was significantly better than that of LNR >0.1 (76.1% vs. 56.4%, respectively; p=0.02). When a cutoff value of 0.15 was chosen, the 5-year DFS rates for LNR ≤0.15 and LNR >0.15 were 69.3%, and 36.2%, respectively (p<0.001), whereas the 5-year OS rates were 74.8% vs. 53.6%, respectively (p=0.01). Although our findings were in line with previous studies [910111516], we were able to show a lower LNR cutoff (0.05) as an independent prognosticator for survival outcomes when a systematic retroperitoneal lymphadenectomy was performed. That is to say; if the percentage of involved nodes is ≥5% to total nodes removed for a cervical patient with stage IIIC disease, she seems to have a two-fold increased risk of recurrence and death.
The current study includes one of the largest retrospective cohorts in the literature focusing on the prognostic value of LNR in node-positive cervical cancer patients. A systematic lymphadenectomy rate of 100% and inclusion of a homogenous patient population in terms of surgery and adjuvant treatment characteristics are the major strengths of the current study.
Estimating risk of recurrence on the basis of LNR may be an emerging prognostic factor in node-positive cervical cancer patients that had received systematic LN dissection. In conclusion, LNR ≥0.05 seems to be an independent prognosticator of both decreased DFS and OS in stage IIIC cervical cancer patients who had been treated with radical surgery followed by adjuvant chemoradiation. When the two-fold increased risk of recurrence is taken into account in women with a LNR ≥0.05, these women may be usual candidates for consolidation chemotherapy at the expense of treatment-related toxicities. After completion of adjuvant chemoradiation, clinicians should pay attention to LNR as a newly emerging prognostic factor in stage IIIC cervical cancer.
 XML Download
XML Download