

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Spontaneous Intracerebral hemorrhage (ICH) accounts for about 15% of all strokes and has a 30-day mortality rate of up to 50%16)18). Several reports have proposed the computed tomography angiography (CTA) ‘spot sign’ as a predictive radiological marker of hematoma expansion3)5)6).
The ‘spot sign’ on CTA was first described in 2007 by Wada et al., and is defined as “tiny, enhancing foci within hematomas, with or without contrast extravasation”18). This is generally interpreted as focal sites of extravasation, a focus of arrested bleeding, or a microvascular abnormality6); however, the exact pathophysiology of the spot sign unknown.
In this study, we assessed digital subtraction angiography (DSA) when a patient's CTA showed the spot sign and analyzed the correlation between the spot sign and the existence of a possible vascular lesion that would lead to hematoma expansion and other factors.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of our institution (VC16RISI0019). Between December 2009 and May 2014, DSA was performed in 52 ICH patients with atypical lobar ICH or abnormalities on CTA findings. Twenty-six of these patients, whose initial CTA showed the spot sign, were analyzed. The spot sign was defined as a 1- to-2 mm high-density lesion within the hematoma on maximum intensity projection (MIP) CTA images. All studies were evaluated by 2 more neuroradiologists and/or neurosurgeons to assess the presence or absence of the CTA spot sign. Cerebral DSA was performed on a SIEMENS biplane neuroangiographic unit (Artis Zee SIEMENS, Germany) by one or two neurointerventionists.
Cases with a hematoma greater than 60 ml, midline shifting of over 10 mm, unstable vital signs, or poor mental status (Glasgow coma scale (GCS) < 6) that needed emergency operations were excluded from the analysis. We also excluded that tumor bleeding, subarachnoid hemorrhage (SAH) due to ruptured aneurysm, and hemorrhage from previously known vascular abnormalies such as arteriovenous malformation (AVM), dural arteriovenous fistula (AVF), and Moyamoya disease.
Data on each patient were collected retrospectively, including: sex, age at presentation, type of hemorrhage, location of the spot sign, antiplatelet use, history of hypertension, diabetes mellitus (DM) and dyslipidemia, GCS score, blood pressure, clotting profile, platelet count at presentation, result of DSA, and type of treatment.
We performed statistical analyses using SPSS version 18.0 (IBM Corporation, Armonk, NY, USA). Continuous variables are presented as means and standard deviations, and variables were compared between the two subgroups with the Chi-squared test and Mann-Whitney U test, as appropriate. A p value of < 0.05 was considered statistically significant.
RESULTS
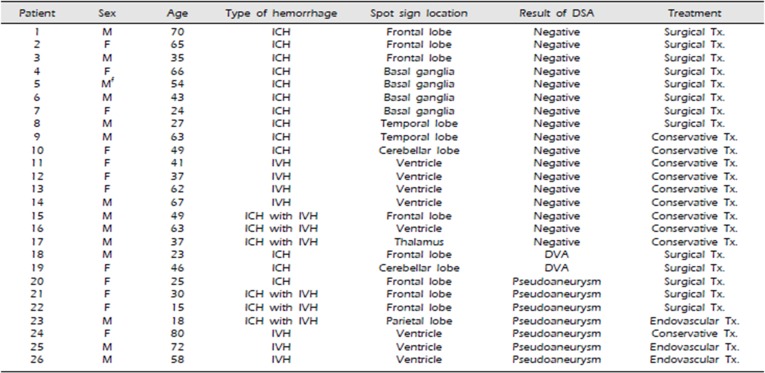
Patients characteristics and ICH location
We collected data on these 26 patients over the course of 54 months (Table 1). As shown in Tables 2 and 3, the mean age of the study subjects was 46.9 years (range, 15 to 80 years) and the percentage of males was 53.8%. Thirteen of 26 (50%) patients had ICH without any kind of hemorrhage and 6 patients (23.1%) had coexisting intraventricular hemorrhage (IVH). Pure IVH was detected in 7 patients (26.9%).
The ICH locations of total 19 patients were distributed as shown in Table 2. ; 8 cases (42.1%) in supratentorial lesion, 3 cases (15.8%) in infratentorial lesion, 5 cases (26.3%) in the deep seated portions (basal ganglia and thalamus) and 3 case (15.8%) in atypical location.
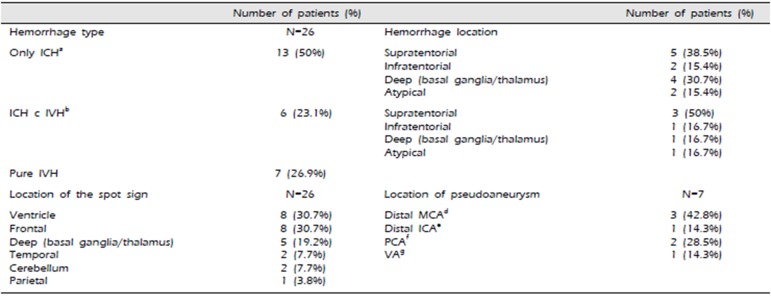
Spot sign and DSA finding
In each 8 patients (30.7%), the location of the spot sign was the ventricle and the frontal area, and in 5 patients (19.2%), the location of the spot sign was the deep location (basal ganglia and thalamus). In two patients each had the spot sign in the cerebellum and the temporal area. In one patient, the location of the spot sign was the parietal area. In 17 of 26 cases (65.4%), the DSA results were negative. Seven patients (26.9%) were diagnosed with pseudoaneurysms, defined as a saccular dilation in the distal portion of the vessels, and two cases showed developmental venous anomalies (DVA). Of the 7 patients with pseudoaneurysm, Each 3 patients (42.8%) presented with pure IVH and ICH with IVH, and one was seen in only ICH. but most (10/17 58.8%) of the patients with negative findings on angiography were in the only ICH group, pure IVH was 4 patients and the remaining 3 patients were in the ICH with IVH.
Half (13/26) of the patients were treated surgically. Three patients underwent endovascular treatment and the other patients (10 of 26) received conservative care, such as medical therapy and extraventricular drainage.
Subgroup analysis
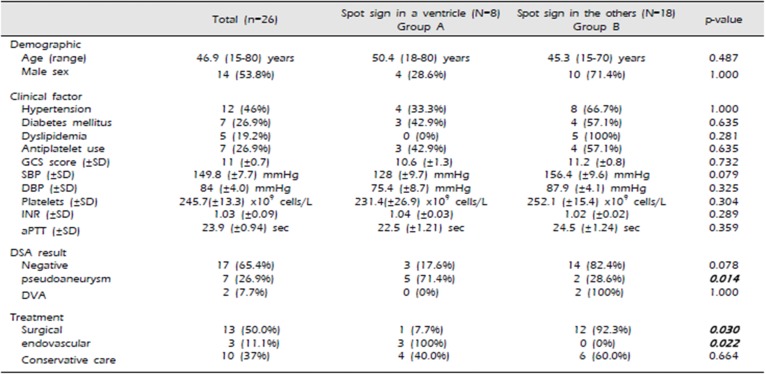
The patients were divided into 2 groups based on initial radiographic features: Group A (8 patients) had a spot sign in the ventricle, and Group B (18 patients) had a spot sign in another site. The characteristics of the patients in Groups A and B are presented in Table 2.
Mean age and the percentage of males were 50.4 years (range, 18 to 70 years) and 28.6% in Group A, respectively, versus 45.3 years (range, 15 to 70 years) and 71.4% in Group B. There were no statistically significant differences between the two groups in terms of past history, initial status, and laboratory findings.
The majority (5/8) of the patients in Group A had significant pseudoaneurysms on DSA (P = 0.014), and three of those five patients required endovascular treatment (P = 0.022). however, only two of 18 patient showed pseudoaneurysms and none underwent the endovscualr treatment in Group B. Most of surgical treatment was performed significantly in Group B (P = 0.030). In the present of spot sign in the ventricle, there were often vascular lesions that could be treated with endovascular procedure and the surgical approach was not easy anatomically from brain cortex to deep in the ventricle.
ILLUSTRATIVE CASES
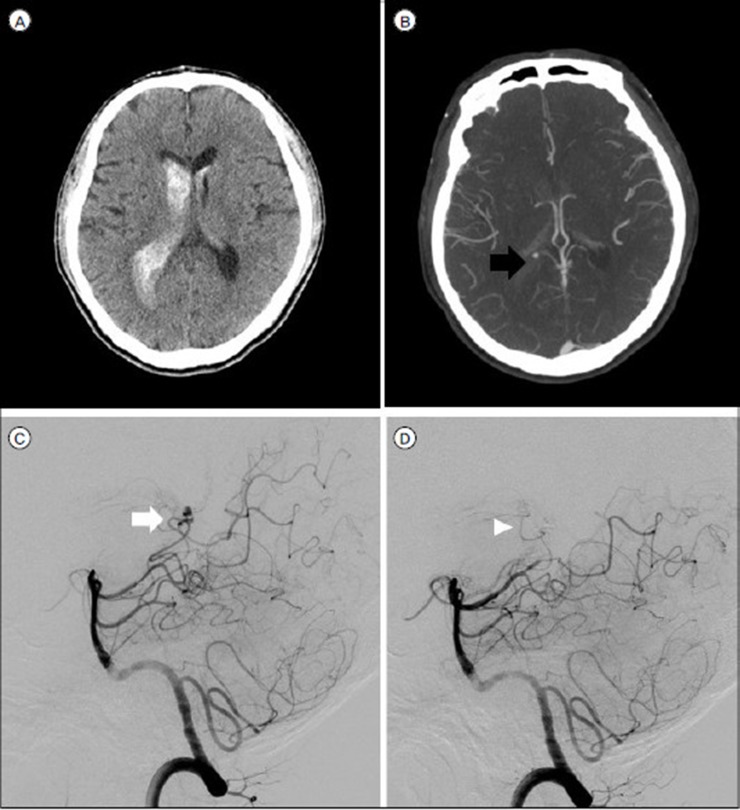
Case 1.
A 54-year-old man presented with ICH in the left basal ganglia with the spot sign on CTA (Fig. 1). The DSA findings were negative, but a follow-up brain CT scan showed expansion of hematoma. The patient's neurological deterioration aggravated; hence, he underwent surgical treatment.
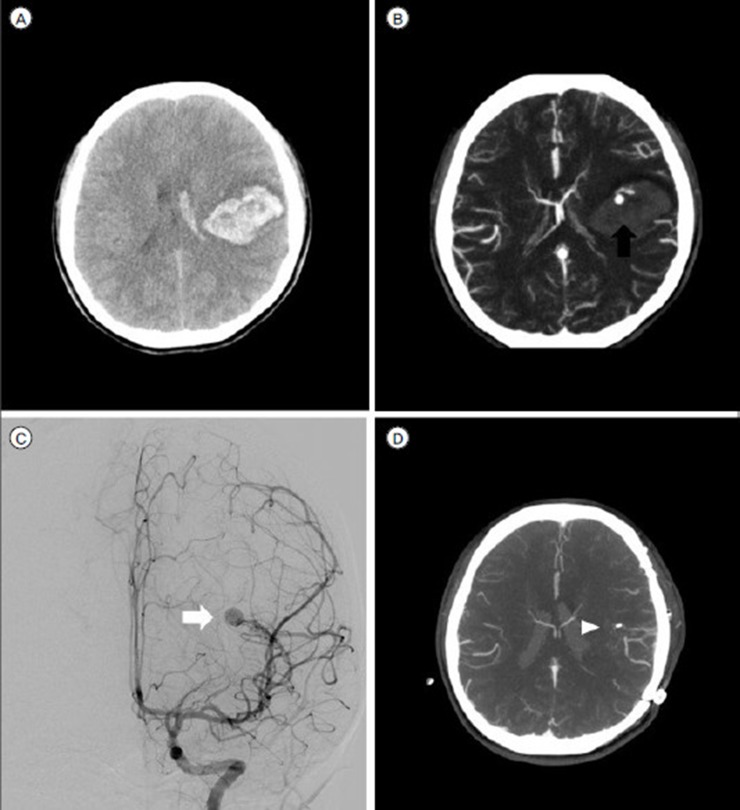
Case 2.
A 46-year-old woman presented with ICH in the left cerebellum with no intraventricular expansion (Fig. 2). The diagnostic angiogram showed DVA. After conservative care for a few days, the hematoma enlarged and her symptoms worsened; she underwent a surgical procedure.
Case 3.
A 58-year-old man presented with IVH with the spot sign on CTA (Fig. 3). DSA showed a saccular pseudoaneurysm in the right posterior choroidal artery. It was successfully treated endovascularly.
Case 4.
A 15-year-old girl presented with ICH and IVH with the spot sign on CTA (Fig. 4). DSA showed an AVM with a round pseudoaneurysm in the left distal middle cerebral artery. The patient was treated surgically.
DISCUSSION
This is the first study to assess the correlation between the CTA spot sign and the existence of a possible vascular lesion using digital subtraction angiography. CTA is rapid, accessible, and widely available and can be used to predict prognosis and to decide upon a treatments on the basis of an initial emergency diagnosis. American Heart Association (AHA) guidelines suggest that CTA can be used to help identify patients at risk and catheter angiography can be useful to search for underlying vascular structural lesions9). Hence, we focused on the information obtained from the two diagnostic tools when patients who had spontaneous ICH with the spot sign were initially seen in the emergency room.
Previous studies reported that the spot sign may have important implications for hematoma expansion3)5) with sensitivity, specificity, positive, and negative predictive values of 91, 89, 77 and 96%, respectively18). Chunyan Lei et al. reported that the presence of IVH is an independents predictors of mortality in ICH patients11). In this study, DSA was performed to identify the cause of bleeding in the patients with the spot sign. Patients were divided into two groups according to the location of the spot sign and the results were compared clinically.
Steve Gazzole et al. assessed the prevalence of the CTA spot sign in cases of primary ICH and secondary ICH. They described mimics of the CTA spot sign and classified them as having vascular or nonvascular causes7). In their study, the causes of secondary ICH were defined as follows: AVM, dural AVF, tumor, aneurysm and Moyamoya disease. They reported 7 spot signs in 30 secondary ICH patients and three cases of tumoral hemorrhaging among those spot sign cases. However, in our study, tumor and aneurysm were excluded and we focused solely on the vascular lesions of the spot sign in the hemorrhages.
In our paper, as per the result of DSA in many cases (17/26), there were no vascular lesions. Pseudoaneurysms and DVAs were detected by cerebral angiography in 7 cases and 2 cases, respectively. The current medical literature indicates an increased prevalence of incidental or asymptomatic DVAs with a low prevalence of ICH and a low morbidity and negligible mortality rate (ICH prevalence, 0–3%, morbidity, 0–10%)12)14)15), but all DVAs in this study required surgical treatment. Presumably, predictive hematoma expansion and high mortality and morbidity are associated with ICH with the spot sign, separately accompanied by DVAs.
Various pathological or idiopathic states, including trauma, rupture of true aneurysms or AVMs, surgical and endovascular procedures, neoplasms, Marfan's syndrome, fibromuscular dysplasia, and vasculitis, which may lead to disruption of the arterial wall are possible causes of intracranial pseudoaneurysms1)4). Pseudoaneurysms of the cerebral arteries are reported very rarely. Traumatic pseudoaneurysms are commonly located peripherally or near the base of the skull19). However, information on the locations of non-traumatic pseudoaneurysms and those due to other etiologies is not currently available. In our study, three of seven pseudoaneurysms (42.8%) were located in the territory of the distal middle cerebral artery and two cases (28.5%) were located in the posterior cerebral arteries. One pseudoaneurysm was located in the distal intracranial artery, and one was in the vertebral artery. (Table 1)
Lee A. Tan et al. reported that a ruptured lenticulostriate artery aneurysm, of which fewer than 50 cases have been reported in the literature8), with the spot sign was clipped17). Other authors published a case report on endovascular treatment of a pseudoaneurysm that formed due to rupture of an anterior communicating artery aneurysm10). Because of their rarity, the natural history and optimal management of pseudoaneurysms are not well understood. Some papers have suggested that DSA is the gold standard for the diagnosis of cerebral pseudoaneurysms13) and endovascular treatment represents a safe and durable procedure2); however, our results suggest that DSA is appropriate for verifying the pseudoaneurysm when CTA shows the spot sign in a ventricle.
We realize that the sample size in our study is too small to generalize the relationship between the spot sign and a pseudoaneurysm. This paper has a limitation in that patient' data were collected and analyzed retrospectively. Also, the definition of a pseudoaneurysm according to the shapes of angiogram is unclear, and we could not confirm the presence of a pseudoaneurysm pathologically because many cases underwent endovascular treatment. Another limitation of the study is loss to follow-up and comparison of results, complications, and prognosis among the different treatment groups.
CONCLUSION
It is known from previous studies that the spot sign and IVH are associated with hematoma expansion, and the correlation of pseudoaneurysms on DSA and the spot sign in the ventricle has been confirmed. When CTA shows the spot sign in a ventricle, it might be a clue that there is an existing underlying vascular lesion that requires endovascular treatment. In such cases, DSA can provide an accurate diagnosis leading to the proper course of treatment.


 XML Download
XML Download