

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
An osteoporotic fracture (OF), is any fall from a standing height or less that results in a fracture, in which the bones had been more fragile due to bone deterioration or low bone mass.[1234] The hip, spine, and wrist are have long been major site for OF and their economic burden is so high.[56] The social burden of fractures will increase throughout the world as the population ages, so the prevention of primary and secondary OFs is essential.[789] Fortunately, OFs are preventable and their understanding of the epidemiology could help us focus efforts on the patients at greatest risk. In addition, it is very important to recognize the risk of secondary fractures that may occur after initial OFs.[1011]
However, many previous studies have focused on characteristics or outcomes of in the general population. Because almost patients with fractures experience abrupt pain or difficulty to walking, they usually visits emergency room rather than outpatient clinic. But we did not find any study that analyzed the characteristics of osteoporosis in patients visiting the emergency room. Therefore, the purpose of this study was to investigate the characteristics of patients who diagnosed as OFs: frequency and distribution of primary and secondary fractures OF, and risk of future fractures.
METHODS
From March 2015 to April 2017, we evaluated 791 patients who were diagnosed with hip (femoral neck or intertrochanteric), spine (vertebrae) or wrist (distal radius fractures). OFs were defined as fractures resulting from low-level trauma equivalent to a fall from a standing height or less and having T-scores ≤−2.5 at either the femoral neck or spine.[12] We included the patients aged from 50 to 90 years and excluded multiple fractures, pathologic fracture, and high energy trauma like traffic accident, fall accident. A total of 406 patients with OFs (316 women and 90 men) with a mean age of 73.7 years were finally included in this study (Fig. 1). This study protocol was approved by Sang-Gye Paik Hospital's Institutional Review Board (No. 2019-10-020).
We grouped our cohort according to fracture site; patients with OF of wrist (W; n=132), spine (S; n=78), and hip (H; n=196). In addition, we classified the patients by their ages into 4 groups (50–59, 60–69, 70–79, and 80–90 years) to analyze differences in fracture location according to age. Finally, all subjects were classified as having first fracture with no history of primary or secondary fracture with past fracture. The risk of future fracture between the 2 groups was evaluated separately.
To analyze the characteristics of OFs, we reviewed medical records to identify patients' fracture site, type of ambulation, lifestyle (bed or floor, family living together), exercise, comorbidities, osteoporosis medication, diagnosis of osteoporosis, body mass index (BMI), and past bone mineral density (BMD) measurements. The types of ambulation were divided into the following 5 categories: independent walking, cane walking, walker walking, wheelchair, or bedridden. The characteristics of the subject group were analyzed. Because patients' lifestyles could be related to the fall, these were divided into bed and floor living, and family living was also investigated. Comorbidities included diabetes mellitus (DM), Parkinson's disease, dementia, thyroid disease, rheumatoid arthritis, and chronic kidney disease (CKD). Osteoporosis drugs were examined only for their presence or absence, because many patients did not remember the type of drug they used or were often prescribed at other hospitals. BMD was measured immediately before or after an acute fracture was confirmed, and bone mass and T-score of the lumbar spine and femoral neck were examined on the dual energy X-ray absorptiomet. The lumbar spine BMD measurement was used as the lowest mean value among 2 or more vertebral bodies.
We analyzed differences in the risk of future fractures among the 3 groups. The FRAX, a Fracture Risk Assessment Tool, was used to assess the risk of future fractures. The FRAX model allows for the estimation of 10-year probability of hip and major OFs using clinical risk factors. In this study, FRAX risk calculation was based on data from Korea.[13141516]
1. Statistical analysis
All data were reported as mean±standard deviation or as numbers and percentages. To compare categorical data between the primary and secondary fracture patients, the χ2 test was used. The χ2 test was performed on the difference of fracture site according to age, and the trend analysis was performed using linear-by-linear association. One-way analysis of variance test and Dunnett's multiple comparison test as a post-hoc analysis were used to compare the FRAX and hip FRAX scores in total patients and the primary fracture groups; Kruskal-Wallis test and Conover multiple comparison test were used in the secondary fracture group. Differences in FRAX and hip FRAX scores between patients with primary fracture and those with secondary fracture were not assumed for equal variance, and the Mann-Whitney test was performed. All results were considered statistically significant when P-values were <0.05. Statistical analyses were performed using SPSS software program version 25.0 (SPSS Inc., Chicago, IL, USA) and MedCalc software (version 19.1; Med-Calc software, Mariakerke, Belgium).
RESULTS
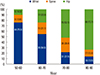
The mean age at fracture site was significantly different among the 3 groups, groups W (66.57±10.03), S (73.50±9.07), and H (78.50±7.72). In post-hoc analysis, groups W, S, and H showed statistically significant difference among all individual groups (P<0.001). There was a statistically significant difference in the fracture site according to age and a tendency for the older age to be associated with fractures in the order of wrist, spine, and hip (P<0.001) (Table 1 and Fig. 2).
In all subjects, there was a significant difference between the FRAX major and hip FRAX scores (P<0.001). In post-hoc analysis, groups W, S, and H showed significant difference among all individual groups (P<0.001) (Fig. 3A). The FRAX major score were significantly different between primary fracture patients (9.83±5.99) and secondary fracture patients (17.34±9.30) (P<0.001). The hip FRAX scores were also significantly different between primary fracture patients (4.40±3.86) and secondary fracture patients (9.56±7.21) (P<0.001).
In the primary fracture patients, the FRAX major scores increased in the order of group W (7.50±4.18), group S (9.76±5.91), and group H (11.93±6.61), and there was a significant difference (P<0.001). In post-hoc analysis, there were statistically significant differences between individual groups in group W vs. group S and group W vs. group H but no significant difference between groups S and H (P=0.065). In primary fracture patients, the FRAX Hip score increased in the order of groups W (2.74±2.85), S (4.35±3.37), and H (5.90±4.23). The post-hoc analysis also showed significant differences among the individual groups (P<0.001) (Fig. 3B).
In the secondary fracture patients, the FRAX major score mean was not significantly different among groups W (16.12±10.37), S (14.86±9.57), and H (18.21±9.02) (P=0.166). The mean FRAX hip score was significantly different between the groups; however, in post-hoc analysis, significant differences were found only between groups W and H (P=0.038) (Table 2).
Past fractures in the secondary fracture patients were W, 14.6% (13/89); S, 16.9% (15/89); and H, 68.5% (61/89). The largest number of past fractures was characterized by matching the secondary fracture sites (Fig. 4).
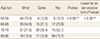
The characteristics of the all patients are shown in Table 3. The mean age of secondary fracture patients (76.89±9.04) was significantly higher than that of primary fracture patients (72.75±10.37). BMI was significantly lower in secondary fracture patients (21.31±3.28) than in primary fracture patients (22.49±2.84) (P<0.001). The rate of diagnosis of osteoporosis and degree of drug administration were lower in primary fracture patients than in secondary fracture patients, and there were statistically significant differences (P<0.001).
DISCUSSION
The average age of the occurrence of OFs was wrist fracture at a lower age, followed by spine and hip fractures. Hip fractures occurred in 73.7% (98/133) of fracture patients over 80 years. As the age increases, the T-score of BMD decreases, thereby increasing the incidence of OFs.[1718] Furthermore, Johnell and Kanis [19] reported that wrist fractures occur at lower ages, whereas hip fractures occur at older ages.
In this study, we examined the fracture sites among the 4 groups classified by age and found that the distribution of wrist fractures decreased with increasing age and hip fractures increased. Among OFs, the most common fracture sites differed according to age. As a result, when the patient is relatively young and has better balance, a hand-holding action is possible, and a wrist fracture often occurs, which may be related to physical activity. In contrast, hip fractures are mainly caused by decrease in exercise ability with increasing age. Gregg et al.[20] reported that the higher the physical activity level, the lower the risk of hip fracture.
Among OFs, 21.9% (89/406) were second fractures with a history of OFs. In case of the second fracture, the prevalence of fracture type followed the same order as the primary fracture, in the order of wrist, spine, and hip fractures. Hip fracture was the most common, at 68.5%. Interestingly, patients with secondary wrist fractures had the highest number of wrist fractures (61.5%), those with secondary spine fractures had the highest number of spine fractures (60%), and those with secondary hip fractures had the highest number of hip fractures (49.2%). This is a little differ from the finding that patients who have experienced vertebral fractures usually develop spine & hip fractures as the next ones.[2122] But, Bynum et al.[23] reported that 4.3% of 273,330 elderly fractures had secondary OFs, and hip fracture was the most common second fracture, regardless of the location of the previous fracture. In the present study, 68.5% (61/89) of patients had secondary hip fractures, making them the most frequent fractures, consistent with the findings of Bynum et al.[23]. Based on this, if the first OF is hip fracture, the subsequent OF is also more likely to be a hip fracture. As a result, hip fractures with a relatively high mortality rate [2425] should be considered to prevent future fractures.
Clinical risk factors for fractures were analyzed, including body weight (BMI), DM, Parkinson's disease, dementia, thyroid disease, rheumatoid arthritis, and CKD. Significant differences in body weight and dementia were found between patients with the primary and secondary fractures. In patients with the second fracture, the body weight was lower and dementia morbidity was higher. As reported in many other studies, smaller body weight is associated with decreased bone size, which can increase the risk of fracture and osteoporosis.[26272829] In this study, the average body weight was smaller in patients with second fracture. In addition, the reason for the higher dementia rate in patients with second fracture may be that they have lower cognitive ability, gait, and sense of balance than those with primary fracture, resulting in a higher probability of falling and higher recurrence rate of fractures. Bohlken et al.[30] studied the relationship between the incidence of dementia and hip fracture and reported that patients with dementia had lower BMD and higher risk of hip fractures than normal subjects. Downey et al.[31] reported that β-amyloid, Apolipoprotein E4, and vitamins K and D were involved in the link between dementia and osteoporosis.
In this study, only 17.7% (72/406) of patients with osteoporosis fractures had previously been diagnosed with osteoporosis, and only 9.4% (38/406) were taking osteoporosis drugs. In particular, patients with secondary OFs were higher than those with primary fracture, but the diagnosis rate of osteoporosis was 30.3% (27/89) and medication rate only 19.1% (17/89), indicating that when OFs occur, BMD examination and diagnosis are active for patients who have not previously been diagnosed with osteoporosis, but medication is not adequately used. Cobden et al.[7] investigated 562 patients with osteoporotic hip fracture aged >65 years and reported that 460 (82%) of them underwent no osteoporosis treatment after hip fracture surgery. And also Kim et al.[32] reported low osteoporosis treatment rates after hip fractures.
Patient cooperation is important in terms of the rate of drug use after diagnosis of osteoporosis, but BMD may be measured at the osteopenia level or higher but not below the World Health Organization diagnostic criteria of osteoporosis, with T-score of −2.5. This may be a reason why the proportion of patients on medication is low. In fact, Miller et al.[33] reported that patients who were not diagnosed with osteoporosis and had T-scores of −2.5 to −1.0 also had a higher risk of developing new fractures within 1 year. Wainwright et al.[34] also reported that 54% of 243 women with hip fractures had no osteoporosis. Based on these findings, osteoporosis fractures may lead to the use of osteoporosis medications to prevent secondary OFs because the T-score may not be lower than the osteoporosis level even when BMD examination is performed.
Because the assessment of fracture risk of BMD is inaccurate, it is used not only for simple BMD examination for the prediction of OF but also for predicting fracture rate using FRAX. The FRAX and hip FRAX scores in this study were gradually increased in the order of wrist, spine, and hip fractures in all subjects and subjects with the primary fracture. In patients with the second fracture, only the hip FRAX score was statistically significant in the order of wrist, spine, and hip fractures. These results suggest that patients with hip fractures with FRAX scores predicting fracture incidence over the next 10 years have a higher incidence of secondary OFs than those with wrist and spine fractures. However, FRAX can also underestimate fracture probability. According to Giangregorio et al.[35], diabetes was also an important risk factor for OFs, and FRAX underestimated its risk in patients with diabetes but showed good concordance in those without diabetes. Leib et al.[36] reported that FRAX scores underestimated the risk when glucocorticoid use was >7.5 mg/day. Therefore, the risk of developing a second fracture may be much greater than the measured FRAX score, suggesting that the risk of future fracture after an OF is higher than the estimated FRAX score, indicating the importance of prevention of future fractures after OFs.
The limitation of this study is that it was only for emergency room patients, except outpatients, which can lead to differences in the number of patients with primary and secondary fractures, especially those who may be outpatients. Furthermore, in case of patients with second fractures, they may visit another hospital for the re-fracture. Therefore, results on the actual incidence of refracture should take into account this possibility.
In this study, OFs were characterized by different incidences according to age. In particular, hip fractures occurred at an older age. If the first fracture occurs in the hip, the subsequent fracture is also likely to occur in the same site, so care should be taken not only for the diagnosis of osteoporosis but also for the prevention of the second fracture.





 XML Download
XML Download