

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obstructive sleep apnea (OSA) is sleep-disordered breathing that is characterized by periods of obstructed breathing during the night, which lead to intermittent and repetitive hypoxia and recurrent arousals during sleep. The prevalence of OSA varies from country to country and ranges from 9% to 38% among general population (1). Many studies have shown that OSA is associated with a relatively higher prevalence of coronary heart disease, heart failure, and stroke (234). Moreover, Munoz et al. (5) reported that patients with severe OSA have an increased risk of developing a stroke (hazard ratio = 2.52).
Silent cerebrovascular lesions, seen as white matter hyperintensity and lacunar infarcts, are a common incidental finding on brain MRI and are considered to be part of the preconditioning phase of cerebrovascular events such as stroke from a preventive medical point of view (678910). Vermeer et al. (6) reported that the presence of silent cerebrovascular lesions increases the risk of stroke more than three-fold (adjusted hazard ratio 3.0, 95% confidence interval 2.3 to 6.8). Thus, the assessment of silent cerebrovascular lesions may have the ability to predict cerebrovascular disease (CVD). The silent cerebrovascular lesions can be evaluated in various ways on brain MRI and one method is using periventricular hyperintensity (PVH) andpatients with severe OSA show a higher prevalence of silent cerebrovascular lesions than those with mild OSA (8910).
Physicians (dentists or otolaryngologists) in a sleep clinic obtain a cephalometric radiograph or airway CT scan to assess a patient's craniofacial and airway anatomy and to manage the plan for comorbid disease in patients with OSA. Sometimes, carotid arterial calcification (CarAC) is observed in the images of a cephalometric radiograph and airway CT (1112). Several studies demonstrated the feasibility of quantifying CarAC with a three-dimensional (3D) carotid CT scan by using the Agatston's method (Agatston score), which has been widely used to quantify calcification of the coronary arteries and predict cardiovascular events (1314151617). Bos et al. (18) suggested that CarAC is associated with the presence of cerebral infarcts in the elderly. Therefore, it may be meaningful to obtain additional information related to CVD using CarACS. However, according to our findings, there has been no study about the association between the CarACS (carotid arterial calcium score) calculated with CT and silent cerebrovascular lesions graded with MRI in patients with OSA. The purpose of our study is to investigate the relationship of CarACS measured on airway CT with a modified Agatston method and silent cerebrovascular lesions quantified on brain MRI with PVH grading system in patients with OSA.
MATERIALS AND METHODS
SUBJECTS
In total, 489 consecutive patients who had undergone polysomnography (PSG) for OSA problem from March 2011 to March 2018 were enrolled. All patients with OSA were routinely subject to upper airway CT to understand their airway morphology and accompanying diseases. Among the 489 subjects, 60 consecutive OSA patients (45 males; mean age, 54.5 ± 10.8 years old; age range, 19–77 years old) who underwent the brain MRI for clinical necessity [neurologic symptoms (dizziness, headache, etc., n = 42); cognitive impairment (n = 10); anxiety (n = 2)] or for a health checkup (n = 6) were enrolled as subjects (Table 1). In the meantime, we excluded people with silent cerebrovascular lesions mimicking diseases such as adult-onset leukoencephalopathies or demyelinating disease that cause white matter hyperintensities on MRI by using other radiologic findings and medical history (7). However, no patient showed evidence of these problems and thus all 60 patients were included as subjects.
This is a retrospective study. The institutional ethics committee approved this study, and written informed consent was waived (IRB No. DAUHIRB-17-113).
POLYSOMNOGRAPHY
Overnight PSG (Alice 5, 19 channels; Philips Respironics, Inc., Kennesaw, GA, USA) was used to diagnose OSA in all patients. In this study, apnea was identified by > 90% reduction of airflow for at least 10 s and hypopnea was identified by ≥ 30% decrease in airflow for at least 10 s, combined with an arousal and/or 3% oxygen desaturation. The apnea index (AI) and hypopnea index (HI) are the average number of apnea and hypopnea events per hour of sleep, respectively. Respiratory effort related arousals (RERAs) were identified as increased respiratory efforts for at least 10 s, followed by an abrupt arousal from deeper sleep, but which did not meet the criteria for apnea or hypopnea. The apnea-hypopnea index (AHI) was defined as the average number of apnea events plus hypopneas events per hour of sleep. The respiratory disturbance index (RDI) is the average number of combined apnea events, hypopnea events, and RERA events per hour during sleep (RDI = apnea + hypopnea + RERAs per hour of sleep). Lowest O2 saturation during sleep is one of indices, used to express the severity of oxygen desaturation during PSG.
MEASUREMENT OF CAROTID ARTERIAL CALCIFICATION
CT PARAMETER
Within 1 week of the PSG examination, all patients routinely underwent non-contrast airway CT scans with a 320-detector-row scanner (Aquilion ONE; Canon Medical Systems Corporation, Otawara, Japan). The image range of the airway CT scan captured an area from the frontal sinus of the skull to the carina level of the distal trachea to embrace both nasal and intra-thoracic airways (Fig. 1). The airway CT scan was set up with the following parameters: collimation, 320 × 0.5 mm; gantry rotation time, 500 ms; tube voltage, 120 kV; tube current, 80 mA; slice thickness, 0.5 mm. All datasets were processed with iterative reconstruction (3D adaptive iterative dose reduction), with a 3-mm slice thickness and a 3-mm interval. The images were then transferred to commercial software (Vitrea 6.0; Vital Images, Minnetonka, MN, USA) for post-processing and analysis.
ANALYSIS OF CarACS
The CarACS was quantified using the modified Agatston method which is a well-known and validated quantitative parameter adopted to assess calcium in coronary arteries. On axial CT images, the software automatically highlights densities greater than 130 Hounsfield units (HU) in a 1 mm2 area (Fig. 1). The calcium score was calculated as the product of the lesion areas and a cofactor between 1 and 5 (cofactor 1, 0 HU; cofactor 2, 1–10 HU; cofactor 3, 11–100 HU; cofactor 4, 101–400 HU; cofactor 5, > 400 HU). An experienced radiologist performed the measurement of CarACS using semi-automated scoring, and particular attention was paid to exclude bony spurs or calcified ligamentous structures. Calcification in the common, external, and internal carotid arteries was measured to calculate CarACS. The total CarACS was estimated as the sum of these scores.
MEASUREMENT OF SILENT CEREBROVASCULAR LESION
All brain MRIs were scanned within 3 years before or after the airway CT scan. The examinations were performed utilizing a 1.5 Tesla MRI system (Signa Excite: GE Medical Systems, Milwaukee, WI, USA) or a 3 Tesla MRI system (Discovery MR 750: GE Healthcare, Waukesha, WI, USA) for a screening or evaluation of cerebrovascular lesion between March 2011 and March 2018. T2-weighted fluid-attenuated inversion recovery (FLAIR) parameters for the two scanners were as follows: repetition time/echo time = 10000/141 ms, TI = 2569 ms, field of view = 21 × 21 cm, matrix size = 160 × 160, slice thickness = 5 mm, interslice gap = 1.5 mm, b value = 1000 s/mm2. The resulting voxel volumes of FLAIR were 8.61 mm3.
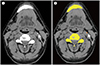
Image analysis was performed using a PACS viewer (INFINITT PiviewSTAR, Infinitt Healthcare, Seoul, Korea). Two trained radiologists blinded to the patients' clinical information such as the degree of CarAC on upper airway CT performed the grading of silent cerebrovascular lesions on brain MRI. The presence of silent cerebrovascular lesions was evaluated on whole brain MRI with T2-weighted and FLAIR images by scoring PVH. The degree of PVH was classified according to Fukuda et al. (1920); PVH 0, no PVH detected; PVH 1, PVH detected in the apex of the frontal or posterior horn; PVH 2, mild PVH detected along the lateral ventricle; PVH 3, PVH strongly detected along the entire lateral ventricle; and PVH 4, diffuse PVH detected in the deep white matter (Fig. 2). If the interpretation of PVH grade differed between two radiologists, it was resolved through a consensus after discussion.
CLINICAL ANALYSIS
The clinical histories of the subjects were reviewed retrospectively within 1 month of the CT study, which included the following: history of comorbid diseases (e.g., hypertension, diabetes mellitus, and smoking), lipid profile (total cholesterol, high-density lipoprotein, and low-density lipoprotein), blood pressure, body weight/height, and body mass index (BMI). Epworth sleepiness scales (ESS), from a simple self-administered questionnaire that is shown to provide a measurement of a subject's general level of daytime sleepiness (0–24 score), were obtained from all subjects just before PSG examination (21).
STATISTICAL ANALYSIS
The results of PSG, the CarACS, and various clinical characteristics were compared among the 5 different PVH groups (PVH grade 0–4). The independent t-test was used for continuous variables, and Fisher's exact test was used for binomial variables. The Kruskal-Wallis test or Mann-Whitney U-test was performed for non-normally distributed variables, according to the results produced by the Kolmogorov-Smirnov test. The CarACS was also analyzed by logarithmic transformation after adding a constant of 1 to each score due to the wide range of values. The associated factors for high PVH grade were first examined using a univariate Cox proportional hazards model, and variables with a significant association (p < 0.20) were applied to a multivariate Cox proportional hazards model. All data was analyzed by SPSS (version 20.0; IBM Corp., Armonk, NY, USA). p-value < 0.05 were considered significant.
We used the intraclass correlation coefficient (ICC), which is an index of concordance about grading of the PVH between two readers. ICC values of 0.00–0.20 were indicative of poor agreement; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, good agreement; and 0.81 or more, very good agreement.
RESULTS
GENERAL CHARACTERISTICS OF THE ENROLLED SUBJECTS
Of the 60 subjects, 75% were of male sex (45 patients), 17 patients were current smokers (28%), 26 patients had hypertension (43%), 8 patients had diabetes (13%), and 11 patients (18.3%) had a history of CVD events (Table 1). According the PSG results, the mean RDI was 31.8 ± 25.9 events/h and the mean AI was 16.3 ± 22 events/h. The mean lowest O2 saturation was 82.8 ± 8.9%. On the airway CT, CarAC was found in 14 patients (23%) and the mean Car-ACS was 45.74 ± 112.3. On the brain MRI, 26 patients (43.3%) showed a PVH grade of 0. There were 14 patients (23.3%) in each of PVH grades 1 and 2, 4 patients (6.7%) having a PVH grade of 3, and 2 patients (3.3%) in PVH grade 4, respectively (Tables 1 and 2). The scoring of PVH showed very good agreement between two radiologists (ICC = 0.961).
COMPARISON OF MEAN VALUES FOR EACH OF THE PVH GRADE GROUPS
The mean patient age showed a significant difference among the 5 PVH groups (p = 0.018), and high grade groups showed relatively older age (PVH grade 0, 50.5 ± 10.3; PVH grade 1, 55.5 ± 6.8; PVH grade 2, 55.9 ± 12.7; PVH grade 3, 63.5 ± 9; PVH grade 4, 68.5 ± 12 years old). Smoking history differed significantly among the PVH groups, with more than half of patients being non-smokers for life in the PVH grade 0 group while all patients were current smokers in the PVH grade 4 group (p = 0.005). Subjects with hypertension were distributed significant differently among groups, and the PVH grade 4 group showed the highest prevalence of hypertension (100% in PVH grade 4, p = 0.036). The other general characteristics including male sex, BMI, prevalence of diabetes, mean cholesterol and ESS score did not differ among the five groups. In the PSG results of the subjects, only AI showed significant differences among the PVH groups, and there were no differences in the other PSG results including mean RDI, HI, RERA, lowest O2 saturation and OSA severity (AI, p = 0.044). Meanwhile, all data related to CarAC such as the presence and absence of CarAC, CarACS, Log (CarACS + 1), and CarACS group demonstrated a significant difference among the PVH grade groups (p < 0.002, p = 0.001, p = 0.001, p = 0.001, respectively) (Table 2).
ASSOCIATED FACTORS WITH HIGH PVH GRADE BY COX ANALYSIS
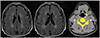
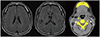
A univariate linear regression model revealed that the Log (CarACS + 1) [standardized coefficient (β) = 0.485, p < 0.001] and age (β = 0.360, p = 0.010) showed significant association with PVH grade. The mean AI and lowest O2 saturation had a weak association with PVH grade, but neither were statistically significant. The male sex, BMI, smoking history, hypertension, diabetes, cholesterol levels, ESS, HI, RERA, and RDI were not statistically associated with PVH grade. In multivariate linear regression analysis, we adjusted for factors reached p < 0.20 by univariate analysis. The Log (CarACS + 1) (β = 0.283, p = 0.038) was the only significant factor for PVH grade and age (β = 0.245, p = 0.065) did not show a statistically significant value (Table 3, Figs. 3, 4).
DISCUSSION
In the comparison of each PVH groups, mean values of age, hypertension, smoking, AI and CarACS showed significant differences among the PVH groups. The associated factors with high PVH grade were AI, lowest O2 saturation and CarACS. Among those, CarACS was statistically significant independent factor after adjusting for the influence of other factors.
In our study, there were statistically significant differences in age, hypertension, and smoking among the five PVH groups. The elderly had a tendency for higher PVH grades, and patients in the PVH 4 group were all smokers and had hypertension. These factors are well known as risk factors for the development of CVD and our results are similar (72223).
In univariate analysis, AI and lowest O2 saturation showed a weak association with PVH grade although the value of RDI showed no significant association with PVH grade. OSA is known as a risk factor for CVD (125). However, it remains unclear whether OSA is an independent or accelerating factor (coexisting with other atherogenic risk factors) for developing silent cerebrovascular lesions, which are the precondition of cerebrovascular events. Davies et al. (24) reported that OSA may be related to an excess of cerebrovascular risk rather than to cerebrovascular damages themselves with qualitatively observed white matter grade evaluation in OSA patients. Kiernan et al. (25) also showed that there is no significant relationship between OSA and white matter changes. However, Gunbatar et al. (26) reported that moderate to severe (AHI ≥ 15/h) OSA patients have a higher prevalence of silent cerebrovascular lesions than a control group (p = 0.028). We found it is worth considering that the AI and lowest O2 saturation correlated with PVH grades.
Various mechanisms are related to apnea or lowest O2 saturation. It is reported that a decreased cerebral perfusion pressure associated with apnea causes abnormal cerebrovascular hemodynamics, which increase intracranial pressure and hypercapnia related apnea, while the subsequent changes in cerebral blood flow velocity and vessel wall tension causes long-term damage of cerebral blood vessels (2728). Patel et al. (29) suggested that nocturnal hypoxemia, which is related to low saturation, may be considered as an independent indicator of silent cerebrovascular lesions among various indicators related to OSA. Zuurbier et al. (30) also reported that oxygen desaturation mainly explains the association between OSA and brain damage. Our results about AI and lowest O2 saturation are relatively concordant with results of these researchers.
PVH grade was associated with CarACS as well as age, which is a conventional risk factor in patients with OSA (2). (Representative cases are shown in Figs. 3, 4). The association between CarACS and PVH grade persisted, even after adjusting for all traditional atherogenic risk parameters, whereas the effect of age disappeared. Although the pathophysiology of silent cerebrovascular lesions is not clearly known in the general population, ischemia, infarction, inflammation, increased vascular permeability, and venous insufficiency have all been suggested as causes of silent cerebrovascular lesions. After all, silent cerebrovascular lesions may be the common result of various pathophysiological disturbances (7). One mechanism related to CarAC is that CarAC induces hyalinization, tortuosity, and elongation of vessels in the periventricular white matter. This may cause a decrease in blood flow in the periventricular white matter, which is vulnerable due to marginal perfusion under physiological circumstances (31). Hougaku et al. (32) suggested that the evaluation of CarAC as a proxy for systemic atherosclerosis could predict latent damage to the brain because the progression of arteriosclerotic change in brain was paralleled by systemic atherosclerosis. There is controversy about the validity of CarAC for the risk of silent cerebrovascular lesion or CVD. Shaalan et al. (33) reported that symptomatic plaques are less calcified and more inflamed than asymptomatic plaques and Fanning et al. (34) suggested that the degree of CarAC does not independently predict future stroke risk. Nevertheless, many researchers have suggested that CarAC is one of the vascular risk factors. Arterial calcification occurs during the atherosclerotic process; after all, CarAC may potentially relate to all parameters for the development of CVD (3536). Cohen at al. (37) explained three reasons why CarAC appears to carry poor cerebrovascular prognosis: CarAC presents a sign of underlying significant carotid stenosis, Car-AC represents simply another indication of a heavy risk factor burden, and CarAC presents an independent risk factor for CVD. The clinical meaning of CarAC and its exact correlation with silent cerebrovascular lesions could not be concluded from this study because there are many confounding and different factors for development of CVD.
There are known biological mechanisms for the association between OSA and silent cerebrovascular lesions during hypoxia, hypercapnia and arousal associated with respiratory events (283839). These mechanisms cause inadequate protection of the brain from rapid fluctuations in pressure that are associated with apnea and long-term damage of cerebral blood vessels (39). With the principle, CarACS may be higher in proportion to the severity of OSA and may be correlated with silent cerebrovascular lesions through CarAC unintentionally found in upper airway CT aside from other examinations including brain MRI.
In this study, several limitations should be acknowledged. First, the study is based on a single medical center, so the number of subjects was relatively small and the proportions of patients in each of the OSA severity, CarAC, and PVH groups were not so even, which may affect the statistical results. Patients who underwent MRI had some limitation for representativity, but they were still consecutive patients and were enrolled without any other exclusion. Second, the brain MRI and airway CT were not performed concurrently because this study is a retrospective study. Third, there were some borderline lesions that were difficult to score with our PVH group definitions for silent cerebrovascular lesions on brain MRI. In some cases, it was difficult to determine the PVH grade, with two observers discussing any discrepancies. However, our study shows very good agreement between radiologists for the grading of PVH (ICC = 0.961). Fourth, we did not sufficiently evaluate the duration or treatment status of OSA, as there was limited information about treatment for OSA in the medical records.
In conclusion, CarAC was an independent risk factor for silent cerebrovascular lesions in patients with OSA. This result may be important for managing co-morbid risk factors for atherosclerosis, to prevent CVD in patients with OSA when high CarACS is incidentally found in airway CT taken for various clinical reasons. The additional analysis of CarACS on OSA patients can be thought to provide more information on their cerebrovascular status.




 XML Download
XML Download